Association between Dental Agenesis and Cancer-A Systematic Review of Literature
Cancer is a heterogeneous disease with clinical and etiological diversity. Teeth are formed from neural crest-derived mesenchyme and epithelium of the first branchial arch and part of the frontonasal process. Dental agenesis is characterized by congenital absence of teeth, affecting approximately 5% to 7% of the population, being more prevalent in the permanent dentition. Some types of cancers such colorectal, ovarian, lung and breast are described as containing association with dental agenesis, having induction factors in association where the mutation in some genes functions as these induction factors for the two pathologies. Through the model of the PRISMA review platform, literature databases were analyzed, where keywords of association of dental agenesis and cancer were used. We found 151 articles that made the association, but only 7 specifically met the search requirements. Some genes such as AXIN2, EDA, FGF3, FGFR2, FGFR10, MSX1 and PAX9 are directly associated with dental agenesis and cancers, such as colorectal, ovarian, lung and breast, since the inactivation of some of them also acts as an induction factor in the developmental predisposition neoplastic. More genetic studies are needed to prove the association between dental agenesis and other types of cancers. However, it is observed that people with dental agenesis already have pre-established genetic alterations, which acts as a facilitator of the development of cancer.
H2,3
Brazil
rodrigosoares002@hotmail.com facilitator of the development of cancer.
Keywords: Cancer; Dental agenesis; Tooth anomalies; Cancer association reviews; JNK: Jun N-terminal Kinase; NSCLC: Non-Small Cell Lung Cancer; SCLC: Small Cell Lung Cancer.
Introduction
Cancer is a heterogeneous disease with clinical and etiological diversity. Although the exact environmental and genetic risk factors associated with cancer remains unclear, the understanding of the mechanisms involved in this disease are evolving [1]. In the other hand, more than 32 million people live with the disease worldwide nowadays and according to the World Health Organization (WHO), the number of new cases of cancer will continue to increase despite the huge investment in the fight against the disease. The most common cancers are lung, breast, intestine, prostate and stomach, respectively [2].
Family history is one of the factors most consistently associated with increased risk of developing cancer [3]. They occur through vertical transmission (from one generation to another), by means of a pattern of Mendelian inheritance. Well defined, in general of the autosomal dominant type, that is, 50% risk of transmission to the offspring in gestation, regardless of gender. Also, high penetrance rate: the individual carrying the mutation has a high risk of developing it. Some characteristics are associated with cancer, such as early age at diagnosis, more than one neoplasia in the same individual, several members of the same family presenting the same neoplasm or related neoplasms and multiple generations [4].
Teeth are formed from neural crest-derived mesenchyme and epithelium of the first branchial arch and part of the frontonasal process [5]. Dental agenesis is characterized by congenital absence of teeth, affecting approximately 5% to 7% of the population, being more prevalent in the permanent dentition [6]. The most common outcome of defective dental morphogenesis in human patients is dental agenesis (absence of teeth). This may affect either the primary or permanent dentition and can range from 5 or fewer missing teeth (hypodontia), 6 or more (oligodontia), to complete absence of teeth (anodontia). Dental agenesis may occur in isolation or as part of a syndrome [7].
Agenesis occurs more with the lower second premolars, followed by the upper lateral incisors and the upper second premolars [8]. In general, agenesis a occurs by mutation in genes AXIN2, EDA, FGF3, FGFR2, FGFR10, MSX1 and PAX9, because all these genes have a direct role in the formation of the teeth [9]. In some cases, dental agenesis may be associated with certain syndromes, such as Down syndrome and ectodermal dysplasia; however, patients with congenital deformities (oral clefts) are more likely to have agenesis and cancer [10].
Some types of cancers are described in the literature as containing association with dental agenesis, having some induction factors in association, where the mutation in some genes serves as these induction factors for the two diseases [11]. Cancer in colorectal, ovarian, lung and breast are examples of cancers already described as containing association with dental agenesis [12]. For exemple, a mutation in the AXIN2 gene was identified in families with oligodontia and colorectal cancer, suggesting that tooth agenesis might be an indicator of colorectal cancer susceptibility [13]. Important studies have shown the relationship between cancer and dental anomalies [8]. So, this study has as the main objective review in the literature the main types of cancers that contain association with dental agenesis.
Material and Methods
Preferred Reporting Items for Systematic reviews (PRISMA) guidelines was adopted to report this systematic review [14]. Database search included PubMed/MEDLINE, Scopus, Google Scholar and The Cochrane Library was carried out by two independent reviewers until December 2018, when we searched the following terms: ‘Dental agenesis’ [Mesh] OR ‘Tooth anomalies’ [title/abstract] AND ‘Cancer association’ [title/abstract]. Association studies between agenesis and cancer were included. There was no restriction regarding language, publication date, and place of publication. Reference list of other articles were used to locate additional studies.
After choosing the papers, and adopting the inclusion criteria, the articles that were selected were analysed meticulously, so that the information contained in one home could be cross-checked by checking the association of the cancer mentioned in the text with dental agenesis, and between them to know if the mutations found in each type of cancer are common among them, when we have as a common cofactor when observed, between cancer and dental agenesis.
Inclusion and Exclusion Criteria
Selection of papers through the inclusion and exclusion of criteria, data extraction, and quality assessment. Meta-analysis was not possible since selected studies did not observe the same variables, methods, participants, and outcomes, which prevented comparisons. A manual search by reading the references of the selected studies was also performed.
Study Selection
Prospective or retrospective cohort studies, case series and case reports describing clinical and/or laboratorial characteristics of patients with dental anomalies associated with any type of cancer were included. The titles and abstracts of all reports in the electronic searches were individually read by two investigators. The studies that fulfilled the inclusion criteria, and those that did not present sufficient information in the title or in the abstract, were fully assessed. A cross check assessment of the articles was performed by another author to guarantee that the proper studies were selected according to the inclusion and exclusion criteria.
Data Extraction
We independently extracted study data through specific extraction forms using Microsoft Excel software. For the study selected, the following information was extracted (when available): Abstracts of eligible studies were first screened by three researchers separately to examine whether they addressed the association between tooth anomalies and cancer. In case of disagreement, a fourth member was invited to assess whether it should be included or not in the study. First author, publication year, country of publication, type of study, sample size, period, age, gender, and type of tumor were extracted from each study. All potential differences in interpretation between the reviewers were discussed to ensure that all the articles reviewed presented a satisfactory level of evidence.
Analysis
All the clinical information of the patients and diagnostic criteria were evaluated for descriptive cross- referencing of the data, considering the information given by the authors. After the analyzes were done and the articles were related carefully, the prevalence of the most common dental agenesis associated with each cancer was observed, making a comparative analysis between cancerous individuals and individuals without cancer incidence, so that we could observe if there was or does not differentiate between the prevalence of agenesis- related teeth in affected and non-affected patients.
Results
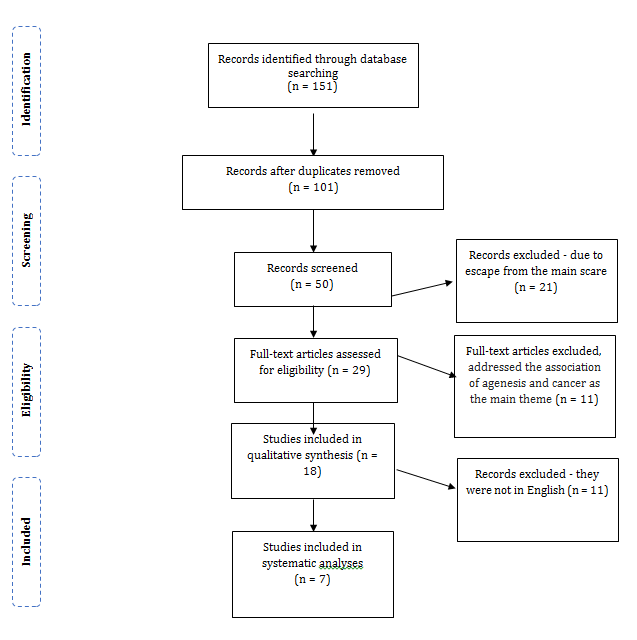
All the papers search retrieved a total of 151 publications. One Hundred articles were withdrawn because they contain duplicates between databases. Then of 21 were excluted because they did not fulfill the criterion of inclusion in the approach of the subject selected, 11 were excluded due to the escape of the subject and because they were not focusing on the changes in the crown that may be common in the two conditions observed. Were excluded 11 articles, because they were not in their original English language publication, and in the end 7 articles were selected due to their eligibility and for complying with the inclusion criteria (Figure 1).
7 deal directly with the dental agenesis associated at cancer (Table 1).
| Methodology | Cancer | Dental agenesis | Results | |
|---|---|---|---|---|
| Lammi, et al. [13] | 11 members of a family lacked at least eight permanent teeth, two of whom developed only three permanente Teeth. Colorectal cancer or precancerous lesions of variable types were found in eight of the patients with oligodontia. | Colorectal | No specified | Oligodontia and predisposition to cancer are caused by a nonsense mutation, Arg656Stop, in the Wnt-signaling regulator AXIN2. |
| Chalothorn, et al. [25] | 50 individuals with epithelial ovarian cancer and 100 control. Dental examination and family history of cancer and dental agenesis were performed. | Ovarian | Maxillary lateral incisors and second premolars. | 20% of individuals with ovarian cancer and 3% of control had dental agenesis. Women with ovarian cancer are 8.1 times more likely to have hypodontia than are without ovarian cancer. |
| Küchler, et al. [6] | 82 individuals with tooth agenesis and 328 control. Familial historic of cancer and oral cleft were analyzed. 14 SNPs in AXIN2, FGF3, FGF10, and FGFR2 were genotyped. | Bladder, Brain and nervous system, Bone Breast, Cervical, Uterus, Esophagus, Head and neck, Intestine, Colon, Lymphoma, | Premolar, upper lateral incisor, Lower incisor, Molar | Breast and prostate cancer were the most common cancer reported in group with dental agenesis. AXIN2, FGF3, FGF10 and FGFR2 were associated with dental agenesis |
Table 1: Specific articles that addressed agenesis and cancer, in this systematic review of the literature.
19.2% of women with ovarian cancer and in 6.7% of women control showed hypodontia. Of family history of hypodontia compared with no report in the control group of women with hypodontia.
4.8% of cases and 5.7% of controls reported having at least one missing tooth.
No association was established with the studied genes and dental agenesis.
One half of the dually affected patients had an independent causation of the two conditions.
In the analysed studies, we can observe a consolidation in the association in the prevalence of cancer in colorectal, lung and breast with patients with dental agenesis. In the study of Küchler, et al. [6], also showed that there is a discrete association between dental agenesis and cancers in bladder, brain and nervous In ovarian cancer, the most frequently absent dental elements were upper lateral incisors, second pre molars and lower molars. In lung cancer was the lower molar. In breast cancer were the superior lateral incisors, second pre molars and lower molars. In colorectal cancer, the lower pre molar and the upper canine were the most absent teeth.
Discussion
- Liver, Lung, Ovary,
- Pancreas, Prostate
- Kidney, Skin,
- Stomach.
- 120 women with epithelial ovarian cancer and 120 women control were reviewed
- Maxillary second
- Fekonja, et al. [1]
- Ovarian premolars and lateral incisors. for the presence and family history of hypodontia.
- 1636 individuals with colorectal cancer and 2788 control. Self-reported information on congenitally missing teeth was collected.
- Lindor, et al. [24]
- Colorectal
- No specified
- MLH1, MSH2, MSH6 and
- PMS2n MUTYH genes were analyzed.
- 4 groups of participants, between affected and control, where the association of agenesis with ovarian cancer
- Maxillary premolars and lateral incisors.
- Bonds, et al. [5]
- Ovarian was analysed. SNPs in
- WNT10A, EDA, PAX9, MSX1,
- AXIN2, BARX1, 2 and BRCA1 were genotyped.
- Critical review on molecular association for genes involving
- Lateral incisor,
- Coloretal, ovarian,
- Win W, et al. [9] premolar and tooth agenesis and breast and lung molar. tumorigenesis.
Table 2: Specific articles that addressed agenesis and cancer, in this systematic review of the literature.
Dental morphogenesis is a complex process that involves epithelial-ectomesenchymal interactions. Numerous transcription factors, growth factors, and their receptors, as well as extracellular matrix components have been associated with early tooth development [14, 1]. The genetic basis of tooth development is supported by the identification of mutations in genes that participate in dental development (AXIN2, MSX1 and PAX9) [16, 17].
The majority of previous studies have revealed that the most common congenitally missing teeth in the white population are the mandibular second premolar, followed by the maxillary lateral incisor [18, 19] and the maxillary canine [20]. Accurate reports of cancer by relatives, combined with family history data often form the basis for inferences about cancer risk factors and patterns of susceptibility, but individual self-reports may be inaccurate and biased [6]. Some results proved a strong evidence that familial colorectal cancer can be caused by mutations in AXIN2. Colorectal neoplasia in the family described in this study was found only in association with oligodontia and the AXIN2 mutation and affected all those of the oldest generation who had the mutation. The causative role of the AXIN2 mutation is also corroborated by earlier findings of somatic mutations in AXIN2 in tumor tissues [9, 21, 22]. The APC gene, mutations of which cause Familial Adenomatous Polyposis, is a key component of the WNT-signaling pathway. In addition, AXIN2 and APC mutations can be associated with dental anomalies including missing or supernumerary teeth [23].
Identification of AXIN2 as a new gene that is responsible for hereditary cancer reduces the remarkable 40% proportion of hereditary colorectal cancers without known molecular causes. It appears that colorectal neoplasia caused by loss of function of AXIN2 has very high or full penetrance. It is interesting that there is a large intrafamilial variation in type and number of colorectal neoplasias and polyps caused by the AXIN2 mutation [24].
Ovarian cancer represents the seventh most common cancer among women in the world. It is also the fourth leading cause of cancer death in women. Researchers found 3% prevalence of hypodontia and microdontia in a control group, and 20% prevalence of hypodontia and microdontia in patients with ovarian cancer. The initial cause of reduced AXIN expression is still undetermined. Promoter hypermethylation of Dab2 or AXIN genes is one possibility. The methylation of AXIN was noted in many tumors, such as breast cancer, head and neck, esophageal, and nasopharyngeal carcinoma [25]. AXIN2 can also promote oncogenicity in colon cancer through the upregulation of Snail1 [21] and a gain-of function mutation; not a nonsense mutation, in AXIN2 would be more compatible with its double role as suppressor of tooth development and promoter of colon cancer. A double role is easier to fathom in the case of alterations in MSX1, a protein that is able to interact with both DNA and other proteins and can act as a transcriptional suppressor or as an activator depending on cellular context [5].
The tumor suppressive role of AXIN is further supported by its participation in the SAPK/Jun N-terminal kinase (JNK) signal transduction pathway, which is activated in cells in response to stress and is involved in many normal physiological processes. Overexpression of AXIN in cells is considered to stimulate SAPK/JNK, inducing apoptosis through the activation of mitogen activated protein/extracellular regulated kinase (MEK) kinase, which may be directly related to the induction of breast cancer, and to the mutation responsible for the agenesis of some dental elements [11].
The AXIN2 gene may be the gene for dental agenesis that makes the connection to breast cancer. First, the AXIN2 gene has been mapped to chromosome 17q23-q24, which is a region that has a heterozygosity (LOH) in breast cancer [26]. Second, it was identified in high-grade breast tumors [26]. Third, it was found that the SNPs in AXIN2 were breast cancer. The rs3923087 polymorphism in AXIN2 is related to reduced risk of breast cancer and the rs3923086 polymorphism is significantly associated with early-onset breast cancer (age ≤43 years). The tooth agenesis gene, MSX1, also showed connections with breast cancer including gene and expression mutations [27].
Lung cancer is classified into two major subtypes, non- small cell lung cancer (NSCLC) and small cell lung cancer (SCLC). Although the mutation of AXIN2 in lung cancer is rare, there is a link between AXIN2 and lung cancer. The AXIN2 gene has been shown to have a connection with lung cancer as well as dental agenesis. Decreased expression of AXIN2 was associated with low survival in early-stage patients, associated with accumulation of b- catenin [8].
PAX9 protein expression was detected. In NSCLC, the activation state of PAX9is correlated with the tissue subtype. Adenocarcinoma has a high probability of PAX9 activation in relation to squamous cell carcinoma [28]. The MSX1 gene showed high methylation in lung cancer, especially in squamous cell carcinomas [29].
This could have important clinical implications in determining whether families with tooth agenesis segregated with severe AXIN2 mutations may have an increased susceptibility for cancer [10]. It is expected that a genetic link between cancer and tooth agenesis would manifest more strongly in first-degree relatives [30]. Küchler [6] says why a cancer was twice as frequent in the second-degree relatives of individuals with agenesis as compared with that in control individuals, while in first-degree relatives the incidence was approximately the same in the two groups. However, this could be explained by the fact that the tooth agenesis case was young, and their parents and siblings were also young and have yet to develop any kind of cancer.
Congenital absence of permanent teeth has direct clinical (visual) implication, and early evaluation of hypodontia phenotype could help us to identify patients at risk for ovarian cancer and serve as a possible marker for ovarian cancer detection. Identification of these high- risk individuals should result in earlier screening regimens for these individuals, an increased number of early diagnoses, and thus the potential to save many lives [31].
Therefore we can observe that several genes that participate directly with the formation of the dental element, can be altered causing agenesis or oligondontia in a person with cancer as in a non-affected person. Tooth agenesis and cancer have some associated genes (AXIN2, MSX1, PAX9 and WNT10A genes). MSX1 and PAX9 genes are related to premolar and molar missing, respectively; while AXIN2 and MSX1 genes with the cancer in breast, colon, lung and ovary. However, the occurrence of mutation in these genes in patients with cancer almost doubled when the comparison was made. Future studies are necessary to better understand this relationship, which may be a signal for early examination.
Conclusion
Genetic studies in the literature show us that some types of cancer as rectal, ovary, lung and breast have a direct association between cancer and dental agenesis. This happens because genes that participate in dental development, when mutated, provide greater viability development of some cancers. More genetic studies are needed to prove this association in other types of cancers. What we can conclude is that people with dental agenesis are more likely to develop some type of cancer because they already contain a mutated pre-established genotype expression.
Acknowledgments
The Minas Gerais State Research Foundation-FAPEMIG, Minas Gerais, Brazil and the National Council for Scientific and Technological Development-CNPq and CAPES, Brazil.
References
-
Fekonja A, Čretnik A, Takač I (2014) Hypodontia prevalence and pattern in women with epithelial ovarian cancer. Angle Orthod 84(5): 810-814.
-
Hafiz A, Mufeed A, Bharadwaj P, Rao D (2016) Dental root agenesis following radiation and antineoplastic therapy: A Case Report. J Indian Soc Pedod Prev Dent 34(1): 96-99.
-
Alvarenga M, Cotta AC, Dufloth RM, Schmitt FCL (2003) Contribuição do patologista cirúrgico para o diagnóstico das síndromes do câncer hereditário e avaliação dos tratamentos cirúrgicos profiláticos. J Brasil Patol Med Lab 39(2): 167-177.
-
Bonds J, Pollan-White S, Xiang L, Mues G, D'Souza R (2014) Is here link between ovarian cancer and tooth agenesis? Eur J Med Genet 57(5): 235-239.
-
Küchler EC, Lips A, Tannure PN, Ho B, Costa MC, et al. (2013) Tooth agenesis association with self-reported family history of cancer. J Dent Res 92(2): 149-155.
-
Fournier DM, Bazzell AF, Dains JE (2018) Comparing Outcomes of Genetic Counseling Options in Breast and Ovarian Cancer: An Integrative Review. Oncol Nurs Forum 45(1): 96-105.
-
Pillas D, Hoggart CJ, Evans DM, O’Reilly PF, Sipila¨ K, et al. (2010) Genome-wide association study reveals multiple loci associated with primary tooth development during infancy. PLoS Genet 6(2): e1000856.
-
Win W, Bian Z (2016) Hypodontia, a prospective predictive marker for tumor? Oral Dis 22(4): 265- 273.
-
Liu W, Dong X, Mai M, Seelan RS, Taniguchi K, et al. (2000) Mutations in AXIN2 cause colorectal cancer with defective mismatch repair by activating b- catenin/TCF signalling. Nat Genet 26(3): 146-114.
-
Yue H, Liang J, Yang K, Hua B, Bian Z (2016) Functional analysis of a novel missense mutation in AXIN2 associated with non-syndromic tooth agenesis. Eur J Oral Sci 124(3): 228-233.
-
Irini T, Paraskevi A, Ioanna G, Christos P, Lydia N (2013) Preserved Axin expression is associated with an aggressive phenotype in invasive breast carcinomas. APMIS 121(9): 797-805.
-
Lammi L, Arte S, Somer M, Jarvinen H, Lahermo P, et al. (2004) Mutations in AXIN2 cause familial tooth agenesis and predispose to colorectal cancer. Am J Hum Genet 74(5): 1043-1050.
-
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J Clin Epidemiol 62(4): 1006-1012.
-
Thesleff I, Nieminen P (1996) Tooth morphogenesis and cell differentiation. Curr Opin Cell Biol 8(6): 844- 850.
-
Miletic I, Sharpe PT (2003) Normal and abnormal dental development. Hum Mol Genet 12(4): 69-73.
-
Stockton DW, Das P, Goldenberg M, D’Souza RN, Patel PI (2000) Mutation of PAX9 is associated with oligodontia. Nat Genet 24(1): 18-19.
-
Vastardis H, Karimbux N, Guthua SW, Seidman JG, Seidman CE (1996) A human MSX1 homeodomain missense mutation causes selective tooth agenesis. Nat Genet 13(4): 417-421.
-
Polder BJ, Vant Hof MA, Van der Linden FPGM, Kuijpers Jagtman AM (2004) A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent Oral Epidemiol 32(4): 217-226.
-
Pemberton TJ, Das P, Patel PI (2005) Hypodontia: genes and future perspectives. Braz J Oral Sci 4(6): 695-706.
-
Letra A, Menezes R, Granjeiro JM, Vieira AR (2009) AXIN2 and CDH1 polymorphisms, tooth agenesis, and oral clefts. Birth Defects Res A Clin Mol Teratol 85(2): 169-173.
-
Wu R, Zhai Y, Fearon ER, Cho KR (2001) Diverse mechanisms of b-catenin deregulation in ovarian endometrioid adenocarcinomas. Cancer Res 61(4): 8247-8255.
-
Taniguchi K, Roberts LR, Aderca IN, Dong X, Qian C, et al. (2002) Mutational spectrum of b-catenin, AXIN1, and AXIN2 in hepatocellular carcinomas and hepatoblastomas. Oncogene 21(31): 4863-4871.
-
Lindor NM, Win AK, Gallinger S, Daftary D, Thibodeau SN, et al. (2014) Colorectal cancer and self-reported tooth agenesis. Hered Cancer Clin Pract 12(1): 7-14.
-
Chalothorn LA, Beeman CS, Ebersole JL, Kluemper GT, Hicks EP, et al. (2008) Hypodontia as risk marker for epitelial ovarian cancer: a case-controlled study. J AmDent Assoc 139(2): 163-169.
-
Yang LH, Han Y, Li G, Xu HT, Jiang GY, et al. (2013) Axin gene methylation status correlates with radiosensitivity of lung cancer cells. BMC Cancer 13: 368-378.
-
Yook JI, Li XY, Ota I, Hu C, Kim HS, et al. (2006) A Wnt- Axin2-GSK3beta cascade regulates Snail1 activity in breast cancer cells. Nat Cell Biol 8(12): 1398-1406.
-
Alanazi MS, Parine NR, Shaik JP, Alabdulkarim HA, Ajaj SA, et al. (2013) Association of single nucleotide polymorphisms in Wnt signaling pathway genes with breast cancer in Saudi patients. PLoSOne 8(3): e59555.
-
Hsu DS, Acharya CR, Balakumaran BS (2009) Characterizing the developmental pathways TTF-1, NKX2-8, and PAX9 in lung cancer. Proc Natl Acad Sci USA 106(13): 5312-5317.
-
Rauch TA, Wang Z, Wu X, Kernstine KH, Riggs AD, et al. (2009) DNA methylation biomarkers for lung cancer. Tumour Biol 33(2): 287-296.
-
Vieira AR, Khaliq S, Lace B (2012) Risk of cancer in relatives of children born with isolated cleft lip and palate. Am J Med Genet A 158(6): 1503-1504.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells