Prevalence of Dental Caries among Sugar Factory Workers - A Cross Sectional Survey
Introduction: Workers in sugar factories are considered to be at high risk for dental caries which is attributed to chronic exposure to sugar dust. Aims: Aim of the survey was to assess the prevalence of dental caries among the sugar factory workers in Davangere district, Karnataka, India. Settings and Design: A cross sectional survey Methods and Material: Voluntary written informed consent was obtained from the study participants. Data pertaining demographic characteristics, oral habits, dietary habits was collected using pretested study Performa along with details of caries experience and oral hygiene status (Decayed Missing Filled Teeth - DMFT Index and Oral Hygiene Index Simplified- OHI S Index). Examiners were trained and calibrated for the recording of indices. Statistical analysis used: Mann Whitney U tests, Kruskal Wallis ANOVA and Linear regression analysis. Results: A total of 315 participants were screened and the prevalence of dental caries was 88.4% among study population with the mean DMFT 3.58 ± 2.94. There was no significant difference in the caries experience of two different sugar factory workers. The caries experience of lower /lower middle class (3.97± 3.23) was significantly higher than the middle/ upper class (p<0.05). Conclusions: The prevalence of dental caries and mean DMFT was high among sugar factory workers in Davangere district. The caries experience was more among workers who brushed less frequently and had poor oral hygiene and who were engaged in pan chewing and alcohol consumption. The caries experience was significantly higher among low socio economic group compared to high and middle class groups.
Introduction
Dental caries is one of the universal diseases which are prevalent in all parts of the world irrespective of the socio demographic characteristics. It is a multifactorial disease in which there is interplay of three primary factors, host, microflora and substrate [1]. Prevalence of dental caries in India is 84.9% considering all the age groups [2]. Industrial workers are placed in a highly complicated environment which is getting more complicated as man is becoming ingenious in nature. As industries are developing, occupational diseases are also becoming more prominent. In many occupations, environmental pollutants like sugar dust, bone dust, flour dust, saw dust etc. contribute to poor oral health. Studies have shown high prevalence of dental caries among industrial workers who had easy access to sugar cane (sugar cane cutters) [3]. According to few studies, workers in bakeries, chocolate and in the candy industries have increased dental caries experience as well as periodontal disease because of high level of sugar dust in the working environment [4]. The Indian sugar industry contributes to about 20% of sugar mills and 15% of the sugar production in the world. It has been shown that confectionary workers have poor oral health than the general population. Sugar dust has been considered to be the main reason for the high incidence of caries among the workers in the confectionery industries and bakeries [5]. Karnataka ranks 3rd in terms of its total sugar production in India. Davangere district is a major contributor to this widespread sugar cultivation in Karnataka [6].
Since no study had been conducted to know the prevalence of dental caries among the sugar factory workers of Davangere district, a study was done to know the prevalence of dental caries among the sugar factory workers in Davangere district and we came with a research question what is the dental caries prevalence among the sugar factory workers in Davangere district? There for the aim of the study was to assess the prevalence of dental caries among the sugar factory workers in Davangere district, Karnataka, India.
Materials and Methods
The present study is a descriptive cross sectional survey, conducted among workers of two sugar factory in Davangere district, Karnataka (M/S Shamanur Sugar Company, Duggavathi, and Davangere Sugar Company Ltd Kukkuwada). All the participants of two sugar factories were male, who fulfilled the eligibility criteria (i.e.) Workers from both production and administrative line workers working in the sugar factories for at least 1 year were included, workers who gave consent to participate and Workers suffering from any systemic diseases and on medications were excluded.
The Study sample was a whole sample of both the factories who participated on the days of survey and examination. The duration of the survey was 2 months (April- May, 2016). A total of 413 participants were present on the days of survey among which 315 were eligible and participated in the survey. Post hoc power analysis was calculated using G Power software inputs were a moderate fixed effect size of 0.3, alpha error probability of 0.05 and total sample size 315 in a z test model and the power of the study is 93%. Ethical approval was obtained from the Institutional Review Board of Bapuji Dental College and Hospital, Davangere. Permission was obtained from the manager of respective sugar factories to conduct the survey. Voluntary written informed consent was obtained from the study participants after explaining them about the purpose of conducting the study Data was collected using pre-tested study proforma. Dental caries experience was recorded using Decayed Missing Filled Teeth and Surfaces Index (DMFT/S Index) given by Henry T. Klein, Carrole E Palmar and Knutson JW (1938) with WHO modification in the year 1997 [7]. Assessment of oral hygiene was done using Oral Hygiene Index- Simplified (OHI-S Index) given by John C Greene, et al. [8]. Examiners were trained and calibrated with respect to recording of indices. The inter examiner reliability was satisfactory with cronbach’s alpha value 0.94 and interclass correlation of 0.96.Data was systematically compiled and analyzed using SPSS software version 20. The prevalence of dental caries was expressed in percentages and the mean Decayed Missing Filled Teeth (DMFT) of sugar factor workers was calculated. Mann whitney U test was used to compare between two groups, Kruskal Walis ANOVA for multiple groups and linear regression to know the relationship between age and socio economic status.
Results
The mean age of the participants were 36.1± 12.24 years. The prevalence of dental caries was 88.4% among study population with mean DMFT 3.58± 2.94. (Table 1) The data was not normally distributed when subjected to normality test using Kolmogrorov- Smirnov and Shapiro Wilk Test at p<0.05. There was no significant difference in the caries experience of two different sugar factory workers (Table 1).
| Sugar Factory | N | Prevalence of dental caries | DMFT Mean ± S. D | P Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kukuwada | 209 | 86.60% | 3.5 ± 2.61 | |||||||||
| Dugawathi | 106 | 90.60% | 3.6 ± 3.52 | 0.46 | ||||||||
| Total | 315 | 88.40% | 3.58 ±2.94 |
Table 1: Distribution of study population based on caries experience DMFT (Mean ± S.
| Type of Employment | F | % | DMFT Mean ± S. D | P value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Production | 252 | 80% | 3.56 ± 2.69 | 0.518 | |||||||||
| Administration | 63 | 20% | 3.65 ± 3.81 | ||||||||||
| Total | 315 | 100% | 3.58 ± 2.94 |
Table 2: Caries experience based on type of employment.
| Duration of employment (In years) | f | % | DMFT Mean ± S. D | P value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| <1 year | 28 | 8.90% | 2.82 ± 2.05 | |||||||||
| 1-5 years | 117 | 37.10% | 3.65 ± 3.26 | |||||||||
| 5-20 years | 134 | 42.50% | 3.52 ± 2.78 | 0.324 | ||||||||
| >20 years | 36 | 11.40% | 4.17 ± 3.04 |
Table 3: Distribution of caries experience among study subjects based on duration of employment.
| Socio-economic status | F | % | DMFT Mean ± S. D | P value | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Class A | Upper/ Upper middle | 32 | 10.2 | 2.81± 1.83 | 0.021⃰ | ||||||||||
| Class B | middle | 93 | 29.5 | 3.04± 2.53 | |||||||||||
| Class C | Lower middle/ lower | 190 | 60.3 | 3.97± 3.23 |
Table 4: Caries experience among study participants based on socio-economic status according to BG Prasad *statistically signific
| Socio-economic status | M. D. | 95% C. I. | p value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| L. B | U. P. | |||||||||||
| Class A | Class B | -0.231 | -1.41 | 0.95 | 0.973 | |||||||
| Class A | Class C | -1.161 | -2.26 | -0.06 | 0.059 | |||||||
| Class B | Class C | -.931* | -1.66 | -0.2 | .016⃰ |
Table 5: Post hoc analysis to assess the significant difference in caries experience between different Socio economic *statistica
Table 5: Post hoc analysis to assess the significant difference in caries experience between different Socio economic *statistically significant at p<0.05; M. D. -Mean difference; C. I. -Confidence interval; L. B. and U.P. - lower bound and upper bound Table 5: Post hoc analysis to assess the significant difference in caries experience between different Socio economic Status groups.
There was no significant difference in the caries experience of subjects who were engaged in pan chewing, tobacco usage and alcohol consumption compared to those without these habits. Caries experience of subjects
- who consumed sugar less than/ equal to five tea spoons per day and more than five tea spoons per day were more or less similar. The mean DMFT of study participants with poor oral hygiene was maximum (3.84±2.16) compared to those with fair and good oral hygiene but this result was not significantly significant.
- *statistically significant at p<0.05
- Multiple linear regression analysis was applied to know the relationship between the variable such as age, socio economic status, sugar consumption and oral hygiene status. The analysis should positive correlation to the variables such as age and socio economic status. The stepwise regression method elicited age as a contributory factor for the significant difference in the socio economic status variable (Table 7).
- Model
- Intercept slope
- R
- R Square
- Adjusted R
- Square
- Change
- Age
- 2.188
- 0.039
- 0.164
- 0.027
- 0.024
- 2.92
- 0.027
- Age, socio economic
- 0.615
- 0.037
- 0.222
- 0.049
- 0.043
- 2.891
- 0.022
- 0.657 status
Table 6: Linear regression analysis for variables with maximum correlation.
| Oral hygiene habits and other | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Type | f | % | DMFT Mean ± S. D | P value | |||||||||||||
| Habits | |||||||||||||||||
| Oral hygiene aids | Tooth brush and paste | 305 | 96.5 | 3.59 ± 2.96 | 0.886 | ||||||||||||
| Fingers and others | 10 | 3.5 | 3.33 ± 2.73 | ||||||||||||||
| Frequency of tooth brushing | Once | 234 | 74.3 | 3.74 ± 3.03 | 0.086 | ||||||||||||
| Twice | 81 | 25.7 | 3.12 ± 2.65 | ||||||||||||||
| Pan chewing | Yes | 110 | 34.9 | 3.65 ± 2.87 | 0.577 | ||||||||||||
| No | 205 | 64.8 | 3.55 ± 3.00 | ||||||||||||||
| chewing tobacco/ smoking | Yes | 45 | 14.3 | 3.29 ± 2.45 | 0.171 | ||||||||||||
| No | 270 | 85.7 | 3.64 ± 3.02 | ||||||||||||||
| consumption of alcohol | Yes | 30 | 9.5 | 3.93 ± 2.91 | 0.791 | ||||||||||||
| No | 285 | 90.5 | 3.54 ± 2.95 | ||||||||||||||
| Sugar consumed each day | <5 tea spoons per day | 180 | 57.1 | 3.36±2.792 | 0.186 | ||||||||||||
| >5 tea spoons per day | 135 | 42.9 | 3.85 ±3.120 |
Table 7: Distribution of Mean DMFT among study participants based oral hygiene habits and other Habits.
Discussion
Occupation has a relationship on health and well-being and there are diverse aspects on the effect of occupation on health [9]. Also studies have provided its positive impact towards oral health i.e. dental caries and its association with occupation [10]. Occupation can affect health through direct impacts, such as physical job conditions, psychosocial job characteristics and stress, and social support. Occupation may also affect health through indirect mechanisms via income, health insurance, prestige, and authority that are related to occupation. Occupational factors like workplace environment, rules and regulations affecting health habits and influence of coworkers might also have significant impact on general as well as oral health [11]. Hence, it is essential to analyze the influence of occupation on health. Same holds true for Sugar Industry in our country (Graph 1).
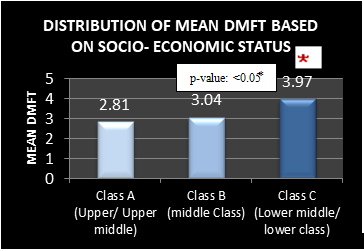
Graph 1: Distribution of Mean DMFT based on Socio- economic status India was the first to begin with the production of sugar following the process of pressing sugarcane to extract juice and boil it to get crystals. Jobs in Indian Sugar Industry have created ample employment opportunities in rural India. Today the Indian Sugar Industry has absorbed about 5 lakh rural people. The working environment in the sugar mills of our country creates a unique environment which might have tremendous influence on the general and oral health of production line and administrative workers. Since no study had been conducted to know the prevalence of dental caries among the sugar factory workers of Davangere district.
Prevalence of dental caries was found to be 88.4% in the present study with mean DMFT of 3.58±2.94. This findings is in accordance with study of Khushboo, et al. where the caries experience of administrative staff of sugar mill workers was similar but caries experience of production line workers was high 7.67 ± 2.99 (mean DMFT) compared to present study results. There was no significant difference in the caries experience of production line workers and administrative workers in the present study. Contradictory finding where, significant difference was observed in the study by khushboo, et al. between production line workers and administrative workers [3, 5, 12].
In another study by Grover S, et al. done on Bakery workers, caries prevalence was seen in 67.6% of the workers [13]. This could most probably be attributed to the relationship between type of work and the relevance of sugar dust as an occupational hazard to dental health as documented in previous studies. Increase in caries experience may also be the result of the increased duration of exposure to sugar dust in the form of airborne contaminants (gases and vapours) or as aerosols [14, 15]. Also, the easy access to sugar in the sugar mills might have contributed to the increased dental caries experience among production line workers as compared to administrative staff. In Post hoc power analysis was done using G power software. Effect size F= 0.215, for sample of 315 the power of the study is 93% Therefore power of 80 the sample size should have been 213 participants.
In the present study there was no significant difference in the caries experience of sugar factory workers with different duration of employment .This result is in accordance with study results of JE Frencken, et al. [3]. However the caries experience increased with duration of employment according to findings of few studies [14, 16]. The caries experience of lower socio economic group was significantly higher than the middle and upper class groups. The results of this study are in accordance with results of systematic review and meta analysis where low SES was associated with high risk of dental caries experience [17]. The major factor for this result could be due to minimal affordability to preventive procedures leading to poor oral hygiene. However, caries experience was high among smokers and workers who did not brush regularly in a study done by DZ Tohidast, et al. [16, 17, 18]. Although not significant, the mean DMFT of pan chewers was more among the workers than non-pan chewers in the present study. Alcohol consumption is considered to be risk factor for dental caries development [19, 20]. The findings of the present study are in accordance with this where dental caries experience was more among alcohol consumers than non-consumers but the difference was not statistically significant. A Meta- analysis done by Kumar S [20] revealed that frequency of tooth brushing had influence on caries experience but was non-significant in our current study.
In the present study, caries experience was high among workers with poor oral hygiene. A systematic review done by Rebba Harris et al revealed that poor oral hygiene may be a contributing factor for dental caries [21]. In a review done by Erik Peterson it has been proposed that poor oral hygiene is one of the risk factors for dental caries [17]. The present study has few limitations. Since the design of the study is cross sectional it is difficult to draw clear cut association between etiologic factor and disease. A comparative group was not considered in the present study which makes it difficult to arrive at conclusions.
Conclusion
The prevalence of dental caries (88.4%) and mean DMFT (3.58± 2.94) was high among sugar factory workers in Davangere district. The caries experience was more among workers who brushed less frequently and had poor oral hygiene and who were engaged in pan chewing and alcohol consumption. The caries experience was significantly higher among low socio economic group compared to high and middle class groups. There was no significant difference in caries experience among administrative and production line workers. There was no significant difference in caries experience of workers with varying duration of employment.
Acknowledgement
We thank the team lead by Divya JM, Divya Rani, Emy Rose John, Anjany Chowdary, Haritha, Jayashri M, Mary
Jose, Jineshwar, Kahon, Kailash, Kanchana, Kavya, Keerthi and Bhargav who conducted the camping survey. We also would like to express our appreciation to the manager and workers of the sugar factory in Davangere district, Karnataka (Kukkuwada, and M/S Shamanur Sugar Company, Duggavathi) for their warm welcome and co- operation during the data collection.
References
-
Rajandran R, Sivapathasundharam B (2012) Shafer’s Textbook of Oral Pathology. 7th (Edn.), Elsevier, pp: 419.
-
Patro BR, Kumar RB, Goswami A, Mathur VP, Nongkynrih B (2008) Prevalence of dental caries among adults and elderly in an urban resettlement colony of New Delhi. Indian J Dent Res 19(2): 95-98.
-
Frencken JE, Rugarabamu P, Mulder J (1989) The effect of sugar cane chewing on the development of dental caries. J Dent Res 68(6): 1102-1104.
-
Anaise JZ (1980) Prevalence of dental caries among workers in the sweets industry in Israel. Community Dent Oral Epidemiol 8(3): 142-145.
-
Singh K, Pandita V, Patthi B, Singla A, Jain S, et al. (2015) Is Oral Health of the Sugar Mill Workers Being Compromised?. J Clini Diagnostic Res 9(6): 7-10.
-
http://business.mapsofindia.com/sugar- industry/karnataka.html. Accessed on 29/03/2016.
-
World Health Organization (1997) Oral Health surveys: Basic Methods. Geneva, WHO.
-
Grenne JC, Vermillion JR (1964) The simplified oral hygiene index. J Am Dent Assoc 68: 7-13.
-
Krantz G, Ostergren P (2001) Double exposure: The combined impact of domestic responsibilities and jobstrain on common symptoms in employed Swedish women. Eur J Public Health 11(4): 413-419.
-
Akrad ZT, Beitollahi JM, Khajetorab AA (2006) DMFT (Decayed, Missing, Filled, Teeth) oral health index in sweets and cable industry workers. Iranian J Publ Health 35(2): 64-68.
-
Gueorguieva R, Sindelar JL, Falba TA, Fletcher M, Keenan P, et al. (2009) The Impact of Occupation on Self-Rated Health: Cross-Sectional and Longitudinal Evidence from the Health and Retirement Survey. J Gerontol B Psychol Sci Soc Sci 64(1): 118-124.
-
Petersen PE (1989) Evaluation of a dental preventive program for Danish chocolate workers. Community Dent Oral Epidemiol 17(2): 53-59.
-
Grover S, Grover R (2013) Assessment of dentition status and treatment needs of bakery workers in lucknow city. Int J Oral Health Res Rev 1(2): 40-45.
-
Rekha R, Hiremath S (2002) Oral health status and treatment requirements of confectionary workers in Banglore city. A comparative study. Indian J Dent Res 13(3-4): 161-165.
-
Hazard Prevention and Control in the Work Environment: Airborne Dust. Protection of the Human Environment Occupational Health and Environmental Health Series, Geneva, 1999, World Health Organization WHO/SDE/OEH/99.14: English only.
-
Schwendicke F, Dörfer CE, Schlattmann P, Foster Page L, Thomson WM, et al. (2015) Socioeconomic inequality and caries: a systematic review and meta- analysis. J Dent Res 94(1): 10-18.
-
Vellappally S, Fiala Z, Smejkalová J, Jacob V, Shriharsha P (2007) Influence of tobacco use in dental caries development. Cent Eur J Public Health 15(3): 116-121.
-
Petersen PE (2005) Sociobehavioural risk factors in dental caries–international perspectives. Community Dent Oral Epidemiol 33(4): 274-279.
-
Jansson L (2008) Association between alcohol consumption and dental health. J Clin Periodontol 35(5): 379-384.
-
Kumar S, Tadakamadla J, Johnson NW (2016) Effect of Tooth brushing Frequency on Incidence and Increment of Dental Caries. J Dent Res 95(11): 1230- 1236.
-
Harris R, Nicoll AD, Adair PM, Pine CM (2004) Risk factors for dental caries in young children: a systematic review of the literature. Community Dent Health 21: 71-85.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells