Effects on Facial Aesthetics and Apnoeic Snoring after Mandibular Advancement with Bilateral Sagittal Split Osteotomy: Two Case Reports
Mandibular advancement surgery is usually indicated in skeletally mature patients with hypoplastic mandible for restoration of harmonious maxillomandibular relationship in all the three planes apart from improving facial aesthetics, oro-facial functions and overall quality of life. Mandibular advancement is also an effective modality for treatment of Obstructive Sleep Apnea with minimal incidence of post-operative complications. This case series describes interdisciplinary management of two skeletal Class II cases with hypoplastic mandible and associated Obstructive Sleep Apnea with mandibular advancement surgery. This would help the clinician in diagnosis and treatment planning of such cases
S6
forces medical college, India
India
forces medical college, Pune, India, Email: docshivagarwal@rediffmail.com cases.
Keywords: Mandibular Advancement Surgery; OSA; Orthognathic Surgery
Appliane; SS: Stainless Steel; GA: General Anesthesia; CPAP: Continuous Positive Airway Pressure; MMA: Maxillo-mandibular Advancement; DO: Distraction Osteogenesis; LI: Lower Incisors; UI: Upper Incisors; NLA: Nasolabial Angle.
Introduction
Orthognathic surgery is usually performed in adult patients with compromised facial aesthetics and/or orofacial function when it is not possible to restore the same with orthodontics alone and/or orthodontics in combination with growth modification [1, 2]. Surgery in these patients bring about restoration of harmonious maxillomandibular relationship in all the three planes i.e., sagittal and vertical apart from improving facial aesthetics, oro-facial functions and overall quality of life transverse [3]. Mandibular Advancement (MA) with Bilateral Sagittal Split Osteotomy (BSSO) is usually indicated in skeletally mature patients with retrognathic mandible. Apart from aesthetic improvement, MA in these patients also increases upper airway dimensions by advancing the tongue, soft palate and associated musculature and thereby widening the upper airway [1].
Obstructive Sleep Apnea (OSA) is characterized by repetitive episodes of upper airway obstruction during sleep and is commonly associated with excessive snoring, excessive daytime sleepiness, impaired memory and fatigue [2]. MA is an effective modality in treatment of OSA with reported mean Apnea-Hypopnea Index (AHI) decrease from 63.9/sleep hour to 9.5/sleep hour with minimal incidence of post-operative complications [4].
For successful management of these patients, a meticulous diagnosis and treatment planning with an interdisciplinary approach holds the key. Pre-operative airway assessment, prediction of post-treatment airway and possibilty of any post-operative airway related adverse events should be meticulously done to achieve favourable results [5].
This paper describes successful interdisciplinary management of two cases of moderate OSA due to retrognathic mandible with combined orthodontics and MA surgery. This would assist the ortho-surgical team in formulating proper diagnosis and treatment plan in such cases.
Case 1
Case evaluation
A 24 years old male reported with complains of poor facial aesthetics and low self esteem because of forwardly placed upper front teeth. He also gave history of excessive day time sleepiness, excessive snoring while asleep and frequent awakening in night with feeling of choking. On extra-oral examination, he had a convex facial profile, acute nasolabial angle (NLA), potentially incompetent lips, a deep mentolabial sulcus and reduced Lower Anterior Facial Height (LAFH) (Figures 1A & B). Intraorally, there was Class II molar and canine relationship bilaterally along with spacing of 4mm in maxilla, an overjet of 10mm along with an impinging deep bite (Figures 1C & D). Orthopantomogram (OPG) (Figure 1E) showed absence of any obvious jaw pathology and 18, 28 and 38 were missing. Lateral cephalogram (Figure 1F) revealed an ortho-positioned maxilla and a retrognathic mandible [SNA=82˚, SNB=76˚, ANB =6˚, Point A-Nasion vertical=1mm, Pog-Nasion vertical= -10mm]. Upper incisors (UI) were proclined [UI-NA = 37˚(9mm)] and lower incisors (LI) were upright [LI-NB =24˚(4mm), IMPA=92˚]. A horizontal growth pattern was evident from reduced Frankfort Mandibular Plane Angle [FMA = 20˚]. The upper lip was protrusive and lower lip was retrusive in relation to Rickett's Esthetic line (E-line). The NLA was reduced (92˚).
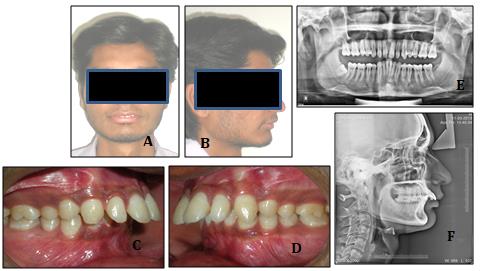
Lateral cephalogram also showed reduced Superior Airway Space (SAS), Posterior Airway Space (PAS) and Minimum Airway Sace (MAS) as seen from values of 8mm, 8mm and 9mm respectively. Acoustic Pharyngometry (AP) findings (Figure 2) indicated reduced mean airway volume (22.08 cc) and area (2.21 cm2). The above findings regarding a compromised airway were confirmed by an overnight Polysomnography (PSG) evaluation which confirmed modearte OSA (AHI=22.5/sleep hour).
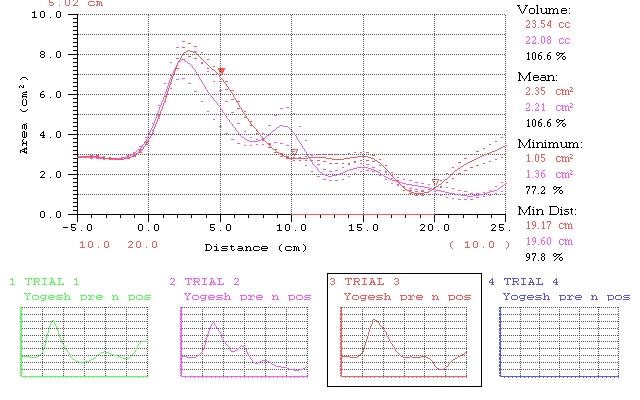
(Pre surgery-Trial 2, Post surgery-Trial 3) Figure 2: Acoustic Pharyngometry report.
Diagnosis
He was diagnosed as a case of skeletally Class II due to retrognathic mandible and dentally Class II Div 1 associated with a horizontal growth pattern along with moderate OSA.
Treatment Objectives
Treatment objectives were to improve facial profile and smile aesthetics; achieve Class I molar and canine relationship bilaterally; optimise overjet and overbite; increase LAFH; and improve airway.
Treatment Planning and Alternatives
The following two treatment options were considered. 1. Extraction of 48 followed by MA of 6mm with BSSO. 2. Orthodontic camouflage with extraction of 14, 24, 35 and 45. Both these options were discussed in detail with the patient and the surgical team. Option 1 was collectively agreed upon. An informed written consent was obtained from the patient.
Treatment Progress
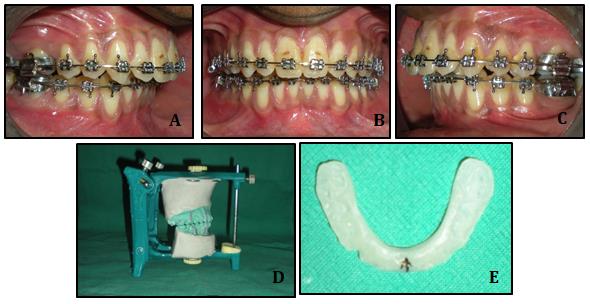
After extraction of 48, the case was banded and bonded with 0.22 MBT Preadjusted Edgewise Appliane (PEA). Leveling and alignment was carried out. Pre- surgically, both arches were stabilised with 0.021X0.025 Stainless Steel (SS) arch wire (Figures 3A-C). The casts were articulated in desired occlusion with tripod contacts on a three point articulator (Figure 3D) and surgical splint was fabricated in self cure acrylic resin (Figure 3E). The orthognathic surgery was carried out under General Anesthesia (GA) and mandible was advanced by 6mm with BSSO as guided by surgical splint. Rigid fixation was done with titanium plates and screws. The surgical splint was luted on maxillary arch 02 days post-surgically for neuromuscular deprogramming and Class II guiding elastics were placed. The splint removed after 06 weeks and settling elastics were placed. The case was debonded after completion of settling. A removable wrap-around retainer in the upper arch and bonded fixed retainer in lower arch were placed for retention.
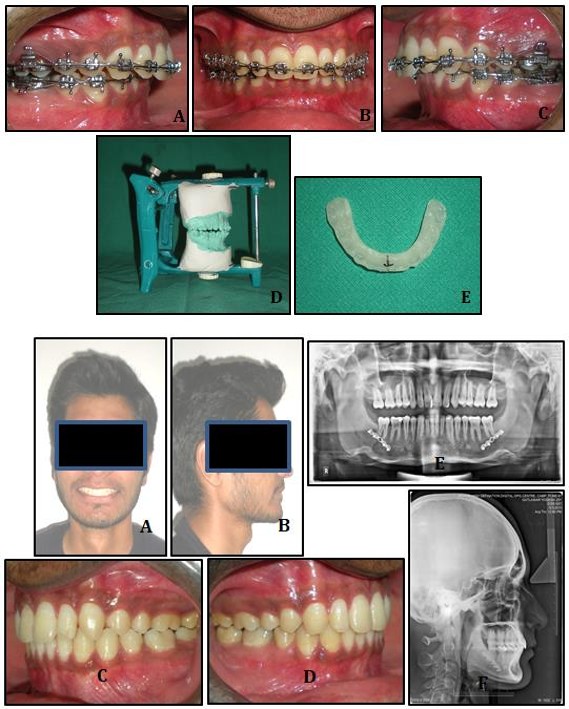
Figures 3A-3E: Pre surgical records.
Treatment Results
Post treatment results showed significant improvement in profile and smile aesthetics of the patient along with improved self-esteem and confidence. Bilateral Class I molar and canine relationship along with an optimised overjet and overbite were achieved (Figures 4A-D). Post-treatment OPG showed achievement of root parallelism (Figure 4E). Lateral Cephalogram (Figure 4F) showed achievement of Class I skeletal bases (ANB value=2˚), optimal incisor positioning [UI-NA = 25˚(5mm), LI-NA = 25˚(4), IMPA = 94˚], improved NLA (100˚) and optimal lip prominence. AP (Figure 2) showed 6.6% increase in both mean airway volume and area. The subjective OSA related symptoms showed marked improvement which was objectively confirmed by PSG (AHI reduction to 4.2/sleep hour).
Figures 4A-4F: Post treatment records.
Case 2
Case Evaluation
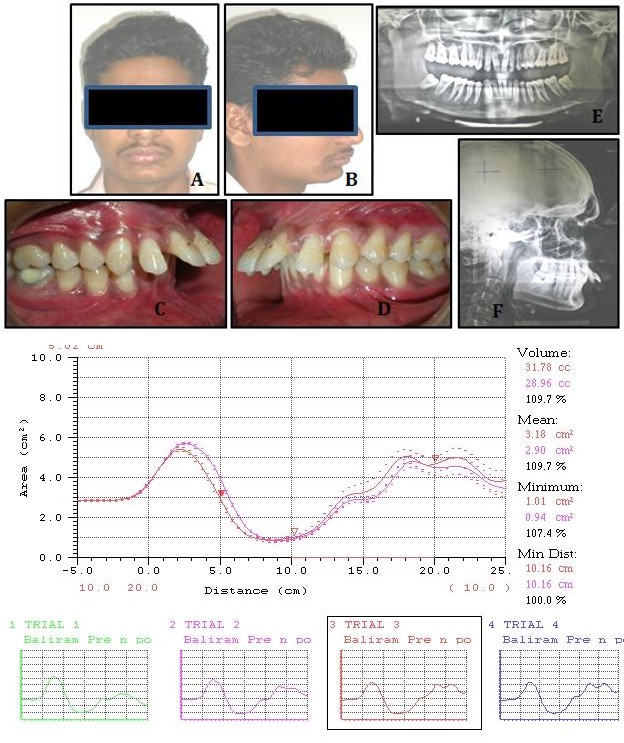
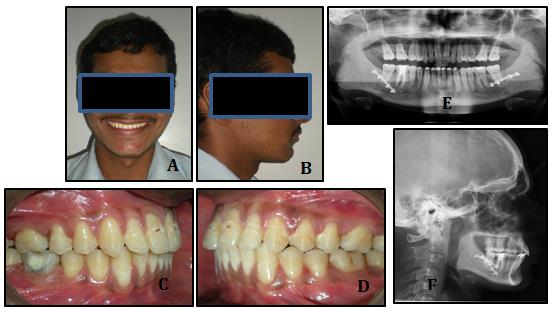
A 26 years old male reported with complains of forwardly placed upper front teeth. He also elicited history of excessive day time sleepiness and snoring while asleep. On extra-oral examination, he had a convex facial profile, reduced NLA, deep mentolabial sulcus and decreased LAFH (Figures 5A & B). Intraorally, there was Class II molar and canine relationship bilaterally along with spacing of 8mm in maxilla, an overjet of 12mm along with an impinging deep bite (Figures 5C & D).
OPG (Figure 5E) showed absence of any bony pathology and all third molars were present. Lateral cephalogram (Figure 5F) revealed an ortho-positioned maxilla and a retrognathic mandible [SNA=82˚, SNB=74˚, ANB =8˚, Point A-Nasion vertical=1mm, Pog-Nasion vertical= -12mm]. Upper incisors were proclined [UI-NA = 38˚(10mm)] and lower incisors were upright [LI-NB =25˚(5mm), IMPA=94˚]. A horizontal growth pattern was evident from reduced FMA [20˚]. The upper lip was protrusive and lower lip was retrusive in relation to E- line. The NLA was reduced (90˚).
Figures 5A-5E: Pre-treatment records.
Lateral cephalogram revealed reduced SAS, PAS and MAS values (8mm, 7mm and 9mm respectively). AP recording (Figure 6) indicated redued mean airway volume (28.96 cc) and area (2.90 cm2). PSG evaluation confirmed modearte OSA (AHI=26.4/sleep hour).
Diagnosis
Similar to case 1, he was also diagnosed as a case of skeletally Class II due to retrognathic mandible and dentally Class II Div 1 with a horizontal growth pattern associated with moderate OSA.
Treatment Objectives
After extraction of the third molars, the case was bonded with 0.22 MBT PEA and arches were leveled and aligned. Pre-surgically, both arches were stabilised with 0.021X0.025 SS arch wire (Figures 7A-C). The casts were articulted in desired occlusion with tripod contacts on a three point articulator (Figure 7D) and surgical splint was fabricated as in case 1 (Figure 7E). The surgery was carried out under GA and mandible was advanced by 6mm with BSSO. The surgical and post-surgical protocol was similar to case 1.
Treatment objectives were to improve facial profile and smile aesthetics; achieve Class I molar and canine relationship bilaterally; optimise overjet and overbite; increase LAFH; and improve airway.
Treatment Planning and Alternatives
The following two treatment options were considered. 1. Extraction of 18, 28, 38 and 48 followed by MA of 6mm with BSSO;
2. Orthodontic camouflage with extraction of 14, 24, 35
and 45. Both these options were discussed in detail with the patient and the surgical team. Option 1 was collectively agreed upon. An informed written consent was obtained from the patient.
Treatment Progress
Figures 7A-7E: Pre surgical records.
Treatment Results
Post treatment results showed marked improvement in facial aesthetics and self-belief in the patient. Bilateral Class I molar and canine relationship along with an optimised overjet and overbite were achieved (Figures 8A-D). Post-treatment OPG showed achievement of root parallelism (Figure 8E). Lateral Cephalogram (Figure 8F) showed achievement of Class I skeletal bases (ANB value=1˚), optimal incisor positioning [UI-NA=26˚(5mm), LI-NA=26˚(4), IMPA=95˚], improved NLA (96˚) and optimal lip prominence. AP (Figure 6) showed 9.7% increase in both mean airway volume and area. Post treatment PSG showed AHI reduction to 3.8/sleep hour indicating marked improvement in OSA. The subjective OSA related symptoms also showed marked improvement.
Figures 8A-8F: Post treatment records.
Discussion
Continuous Positive Airway Pressure (CPAP) is considered as a gold standard in management of OSA in adults. But due to problems like poor compliance and portability related issues associated with CPAP, alternative modalities like Maxillo-mandibular advancement (MMA) surgeries and oral appliance therapy have been employed in these patients [6, 7, 8, 9]. MMA surgeries are well recognised treatment modalities for management of OSA in patients with posteriorly positioned maxilla/mandible and in patients not who are not amenable to behaviour modification, CPAP and/or oral appliance therapy. Various degrees of success and long term stability with MMA have been reported in literature [6, 7, 8, 9, 10]. Orthognathic surgery in these patients is usually performed after skeletal maturity is achieved in order to prevent growth related relapse. Distraction osteogenesis (DO) is a viable option in younger children and in syndromic patients [11]. Both cases described in this paper were skeletally mature with moderate OSA secondary to mandibular retrognathism and desired simultaneous aesthetic enhancement along with improvement in OSA. Hence, MA with BSSO was undertaken in these patients.
Various modalities have been reported to evaluate airway in literature which includes Lateral cephalogram, 3D modalities like CT and MRI and more recently Acoustic Pharyngometry (AP). Lateral cephalogram has limited acceptability in airway evaluation as it is a two dimensional (2D) representation of three dimensional (3D) structures. CT and MRI are not frequently used due high cost and radiation exposure related shortcomings [12, 13, 14]. AP provides valuable information about airway by locating the exact site of airway obstruction, providing mean values of pharyngeal volume and area which can be compared with population norms and also by providing base line data with which post treatment results can be compared [15]. Therefore, AP was additionally used in both cases along with Lateral cephalogram to evaluate airway. In both patients, pre-treatment Lateral cephalogram and AP evaluation showed reduced airway dimensions (PAS, SAS and MAS). The possibility of OSA was confirmed by an overnight PSG which is considered gold standard. PSG confirmed moderate OSA in both cases [16].
Elshaug et al in their study8 considered post-surgical AHI between 5 and 10/hour as an indicator of successful treatment. A meta-analysis involving 22 studies concluded post treatment AHI<5/hour as a successful treatment result [4]. In both cases, MA brought about significant reduction in OSA with post treatment AHI<5 in both cases indicating success. AP and Lateral Cephalogram also showed improvement in airway post surgically in both cases.
Literature reveals that MA brings about significant improvement in profile, smile aesthetics and overall quality of life [3]. The same were achieved in both the cases as seen from both subjective and objective post treatment evaluation. Both cases are under regular follow up and 01 year post treatment skeletal and airway stability is satisfactory.
Conclusion
The case reports in this paper highlight management protocol in cases of skeletal Class II malocclusion due to mandibular retrognathism associated with OSA. Orthodontics combined with orthognathic surgery brings about positive improvement in such cases. Meticulous diagnosis and treatment planning with active participation of the patient holds the key to success. The main limitations of this study are: limited sample size (two case reports) and absence of long term follow up. The authors recommend prospective studies with a larger sample size to validate the finding of this paper.
References
-
Nguyen T, Phillips C, Paniagu B (2016) The use of SPHARM-PDM and mean latitude axis to evaluate airway changes. Angle Orthod 86(6): 943-948.
-
Agarwal SS, Nehra K, Jayan B, Sahoo NK, Roy ID, et al. (2017) Ortho-surgical management of skeletal Class III malocclusion with severe tooth size arch length discrepancy. Journal of Contemporary Orthodontics 1(3): 45-51.
-
Shelly AD, Southard TE, Southard KA, Casko JS, Jakobsen JR, et al. (2000) Evaluation of profile esthetic change with mandibular advancement surgery. Am J Orthod Dentofacial Orthop 117(6): 630- 637.
-
Holty JC, Guilleminault C (2010) Maxillomandibular advancement for the treatment of obstructive sleep apnea: A systematic review and meta-analysis. Sleep Medi Rev 14(5): 287-297.
-
Proffit WR, Phillips C, Turvey TA (1991) Stability after surgical orthodontic correction of skeletal Class III malocclusion. 3. Combined maxillary and mandibular procedures. Int J Adult Orthod Orthognath Surg 6(4): 211-225.
-
Goodday R (2009) Diagnosis, treatment planning, and surgical correction of obstructive sleep apnea. J Oral Maxillofac Surg 67(10): 2183-2196.
-
Edmonds JC, Yang H, King TS, Sawyer DA, Rizzo A, et al. (2015) Claustrophobic tendencies and continuous positive airway pressure therapy non-adherence in adults with obstructive sleep apnea. Heart Lung 44(2): 100-106.
-
Elshaug AG, Moss JR, Southcott AM, Hiller JE (2007) Redefining success in airway surgery for obstructive sleep apnea: a meta analysis and synthesis of the evidence. Sleep 30(4): 461-467.
-
Nimkarn Y, Miles PG, Waite PD (1995) Maxillomandibular advancement surgery in obstructive sleep apnea syndrome patients: long- term surgical stability. J Oral Maxillofac Surg 53(12): 1414-1418.
-
Vicini C, Dallan I, Campanini A, De Vito A, Barbanti F, et al. (2010) Surgery vs ventilation in adult severe obstructive sleep apnea syndrome. Am J Otolaryngol 31(1): 14-20.
-
Pattanaik S, Mohammad N, Parida S, Sahoo SN (2016) Treatment modalities for skeletal class III malocclusion: early to late treatment. IJSS Case Reports & Reviews 2(8): 28-33.
-
Irani SK, Oliver DR, Movahed R, Kim YI, Thiesen G, et al. (2018) Pharyngeal airway evaluation after isolated mandibular setback surgery using cone-beam computed tomography. Am J Orthod Dentofacial Orthop 153(1): 46-53.
-
Chang MK, Sears C, Huang JC, Miller AJ, Kushner HW, et al. (2015) Correlation of airway volume with orthognathic surgical movement using cone-beam computed tomography. J Oral Maxillofac Surg 73(12): 67-76.
-
Kamburoglu K (2015) Use of dentomaxillofacial cone beam computed tomography in dentistry. World J Radiol 7(6): 128-130.
-
Viviano JS (2002) Acoustic Reflection: Review and Clinical Applications for Sleep Disordered Breathing. Sleep and Breathing 6(3): 129-149.
-
Van de Water AT, Holmes A, Hurley DA (2011) Objective measurements of sleep for non-laboratory settings as alternatives to polysomnography--a systematic review. J Sleep Res 20(1): 183-200.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells