Dental Caries Experience and Associated Oral Health Determinants of 5-6 Year Old Schoolchildren in Kandy District, Central Province of Sri Lanka
The aims of the present study were to measure the prevalence of dental caries in schoolchildren aged 5-6 years in Kandy district, in Sri Lanka and the influence of determinants of health on dental caries. A descriptive cross sectional analytical study was conducted in October to December 2010 and a total of 410 children at mean age of 67.3 months (5 years and 7.3months) were selected from schools located in different geographic regions in Kandy district. A calibrated examiner performed the clinical examinations and collected data according to the World Health Organization (WHO) standards in 1997. Data analyses were subsequently conducted to identify differences and association between dmft and schoolchild oral health behavioral and parent socio-behavioral determinants using Chi square test and odds ratio analysis respectively. In the sample of schoolchildren analyzed in this study, the mean dmft was 3.5 (±0.36), mean dmfs was 6. 8 (± 0.8) for deciduous teeth and mean DMFT was 0.02 (± 0.01) for permanent teeth. Caries prevalence was 68%. There was no statistically significant difference between male and female children. The decayed, missing and filled components of the dmft were respectively 76.26%, 10.61% and 12.9% respectively. The Care Index of the present study sample was very low as10.61%. According to the results of this study, a significant difference was observed in dmft between children who used and who did not use fluoride toothpaste (p ≤ 0.005). In conclusion prevalence of dental caries among 5-6 year old children in Kandy district is relatively high (68.8%) with high dmft level of 3.5±0 highlighting the urgent need of interventional programmes aimed at improving oral hygiene among them.
Introduction
Over the past two decades the incidence and prevalence of dental caries among children have declined in industrialized countries, while developing countries have experienced an increasing trend [1, 2]. Therefore, dental caries has become a significant public health problem among children especially in developing countries like Sri Lanka. However, dental caries is a disease of multifactorial etiology which can be prevented using established, evidence-based preventive methods such as fluoride applications, fluoride mouth rinsing, diet modifications and good oral hygienic practices. In fact, the WHO oral health report-2003 [1] noted that the prevalence and incidence of dental caries can be controlled by the joint action of the community, professionals and individuals.
National Oral Health Survey (NOHS) of Sri Lanka in 2003 [3] which traditionally assess the oral health status and treatment needs of Sri Lankan population, reported that mean decayed, missing, and filled teeth (dmft – for deciduous teeth) among the 5 year old children is at a moderate level of 3.51 consisting of 3.26 mean number of decayed teeth (d), 0.12 mean number of missing teeth (m) and 0.13 mean number of filled teeth (f). Furthermore, the prevalence of dental caries in the 5 year old group was reported as 65.31% and 2.21% for deciduous and permanent dentition, respectively. In addition, it has been reported that the prevalence of dental caries varies in different regions of Sri Lanka. For example, the prevalences of dental caries in Galle (southern province), Kandy (central province) and Kalutara (western province) for the 5 year age group were reported as 74.2%, 67.5% and 77.5% respectively. Further, the fluoride levels in water bases have shown a great diversity from less than 0.05ppm to 5ppm [4] in different parts of Sri Lanka. From the published data on NOHS, the prevalence of dental caries in different geographical regions emphasizes the fact that the caries level and water fluoride concentration in water are interrelated in different regions of the country. For example, 14 year old children in Colombo city where levels of fluoride in communal water supply systems was 0.1- 0.5ppm have shown moderate caries level as 3.2 in DMFT and 4.3 in DMFS [5] for permanent teeth. A study conducted to assess caries and fluoride levels in drinking water and their association in children aged 14 living in Uda Walawe; an area with high concentration of fluoride in drinking water, showed that both the caries prevalence and the mean caries experience were significantly lower as DMFS (0.25 + 0.7) for diffuse enamel opacities, and DMFS (1.1 + 1.7) for severe form of enamel opacities [6]. Further they showed that caries prevalence varied between 18- 25% whilst the mean DMFT and DMFS values ranged from 0.29-0.54 and 0.45-0.67 respectively [7]. Further it is noteworthy that only 14.7% of the Sri Lankan population received the desired level of fluoride concentration around 1mg/liter through natural drinking water supplies and the majority of the population is unaware of this fact [8].
Lack of studies on caries prevalence and contributory factors in different age groups in different regions of Sri Lanka emphasize the necessity of further studies in this milieu. This study was undertaken to assess the prevalence and severity of dental caries and the effectiveness of socio- behavioral factors in caries reduction in 5–6 year old school children in Kandy district of Sri Lanka where the naturally occurring water borne fluoride level is low.
Materials and Methods
Ethics Approval and Consent to Participate
The study was approved by Research and Ethical Review Committee of the Faculty of Dental Sciences, University of Peradeniya, Sri Lanka under the ethical clearance certificate No: FDS-RERC/2009/13/Herath 2. The permission to conduct the study in schools was obtained from the Zonal Education Authority, Kandy, Sri Lanka. Following an explanation of the study objectives, verbal and written consent were obtained from the school, schoolchildren enrolled in the study and their parents or guardians. Informed written consent to publish the data received from the participants was obtained in the same consent form which was used to get the consent for the participation. The current study does not contain any form of images and videos. Basic personal data were used only to identify the participant.
Participants
The study population of schoolchildren at the age of 5- 6 years was drawn from schools in Kandy district in Central Province Sri Lanka. Since, attrition was expected during the study period; an additional 100 children were added to the calculated sample size of 360. Thus, the final sample became 460, which was sufficient to achieve the objectives of the study, and exceeded the sample size recommended by WHO for a national basic oral health survey [9]. Children with congenital diseases affecting the dentition and mentally retarded children were excluded from the study. Oral health education was given prior to the clinical oral examination. All the children received elaborated oral health instructions and routine dental treatment when necessary from the Teaching Hospital (Dental), Faculty of Dental Science, University of Peradeniya, Sri Lanka.
Sample and Data Collection
Denuwara education zone was randomly selected from six education zones in Kandy district. According to the categorization of schools as popular (urban), unpopular (semi-urban) and rural in Sri Lanka, two schools were randomly selected from each category of schools in Denuwara education zone in Kandy District. All the children at the age of 5-6 years were invited to participate the study and they were at mean age of 67.3 months (5 years and 7.3months). The required number of schoolchildren in the sample was achieved by sampling with probability proportion to size from each category of schools. The data were collected from October to December 2010 in randomly selected six schools in Kandy district. Clinical examination for dental caries was performed by a single examiner; a specialist in Dental Surgery, who was trained and calibrated for the entire study. Intra-examiner variability was tested using Kappa statistics and it became 0.849 (95%CI 0.760, 0.937 with SE ±0.045).
The examination was done within the school premises under natural light using autoclave sterilized dental mirrors and explorers and no radiographs were taken. Caries was diagnosed using criteria set by the WHO (1997) [9] and quantified using decayed (d/D), missing (m/M) and filled (f/F) teeth index (dmft/DMFT) and tooth surface index (dmfs/DMFS). Dental caries in terms of prevalence and severity were measured based on the dmft/DMFT and dmfs/DMFS indices. Children's age, sex, health, determinants and oral health behavior as well as the parents’ socio demographic data were collected from parents’ on the day of oral health examination by a trained interviewer (Table 1). After exempting the data of 50 children based on exclusion criteria, the data of 410 children were analyzed.
Statistical Analysis
Care Index was adopted to assess the oral health care level of the population. It was calculated by dividing the total number of filled teeth by the total dmft of the study sample and then into hundred percent (f/dmft x100) which is equal to the filled component of the sample. Statistical analysis was carried out using Minitab 16 statistical software.
Difference and association between dmft and child oral health behavior and parent socio-demographics of children at mean age of 67.3 months (5 years and 7.3months) were assessed using Chi-square test and odds ratio analysis respectively. During this assessment the questionnaires with non-responses were considered. Chi- square test was applied to measure differences between two or more categorical variables while considering the dmft cut off point as 50th percentile. Parent demographic factor; the knowledge of oral health was collected by three closed questions; “whether inappropriate brushing affects development of caries or not”, “whether frequent sugar intake affects development of caries or not” and “whether fluoride reduces caries or not”. If the parent answered “yes”, then he/she has been given one point for each question. Thereby, individual parent knowledge score was assessed as the sum of these points. Odds ratio was employed to identify any association between determinant of health variables and dental caries. Adjusted odds ratios with 95% confidence intervals were calculated for all significant variables in the final model.
| Oral health behavioural determinants of children | Socio-demographic determinants of parents |
|---|---|
| Frequency of tooth brushing | Income |
| Usage of tooth paste with fluoride | Father's education level |
| Frequency of intake of sweet food | Mother's education level |
| Parents who brush children teeth | Knowledge on factors that influence the tooth decay of a child |
Table 1: Oral health determinants of survey sample.
Results
Out of the 410 schoolchildren who completed the study and at mean age of 67.3 months (5 years and 7.3 months), 224 were boys and 186 were girls representing
54.63% and 45.37% of the study sample respectively. Table 2 shows their caries experience according to the sex and to the total sample.
| Sex | No | % of caries free | % of dental caries | Mean dmft(±SD) | Mean dmfs(±SD) |
| Male | 224 | 72 (32%) | 152 (68%) | 3.7 (±0.5) | 7.2 (±1.1) |
| Female | 186 | 60 (32%) | 126 (68%) | 3.3 (±0.5) | 6.3 (±1.1) |
| Total | 410 | 132 (32%) | 278 (68%) | 3.5 (±0.4) | 6.8 (±0.8) |
Table 2: Shows the caries prevalence and the severity of the total sample.
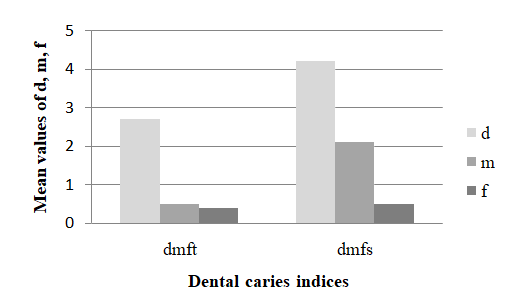
Out of the total sample, 32% of the children were caries-free and 68% were caries active. The index for decayed, missing and filled teeth for tooth surfaces (dmfs) was high as 7.2 (±1.1) (Table 2). The mean dmft index of the children was 3.5 (±0.4), and the mean dmfs index was 6.8 (± 0.8) while mean DMFT and DMFS indices were 0.02 (±0.01) and 0.02 (±0.01) respectively (Figure 1). Although, the dmft and dmfs indices levels of boys and girls are not statistically significant in this sample, the boys had higher dmft and dmfs than girls.
The decayed, filled and missed components of dmft comprised of 76.42%, 10.61% and 12.97%, respectively (Table 4), which were not statistically significant between boys and girls. The oral health care level of the population was assessed by means of Care Index and it was 10.61% (Table 3). According to the chi-square analysis on parent socio-demographics, children who used fluoride toothpaste showed lower incidence of caries than others, (OR=0.24, p<0.05) emphasizing that fluoride toothpaste has a positive impact on prevention of dental caries in primary schoolchildren (Table 4).
| d | f | m | |
| Female | 75.10% | 11.60% | 12.30% |
| Male | 76.90% | 9.90% | 13.20% |
| Total | 76.42% | 10.61% (Care index) | 12.97% |
| p-value p<0.05 | 0.616 | 0.3 | 0.691 |
Table 3: Percentages of decayed, missing and filled teeth in 5-6 year old children in Sri Lanka.
| Model 1 number of dmft | P value | Model 2 number of dmft | P value | ||||
|---|---|---|---|---|---|---|---|
| 0 | 1+ | 0-2 | 3+ | ||||
| Gender | Males | 72(32.1%)* | 152(67.9%) | NS | 105(46.9%)* | 119(53.1%) | NS |
| Gender | Females | 60(32.4%) | 125(67.6%) | NS | 94(50.3%) | 92(49.7%) | NS |
| Children's Oral health behavior | NS | ||||||
| Frequency of tooth brushing | 1 time or less/day; 2-3 times/day | 15(26.3%) | 42(73.7%) | NS | 23(40.4%) | 34(59.6%) | NS |
| Frequency of tooth brushing | 1 time or less/day; 2-3 times/day | 78(33.1%) | 158(66.9%) | NS | 119(50.4%) | 117(49.6%) | NS |
| Usage of tooth paste with fluoride | No or don't know Yes | 3(15.0%) | 17(85.5%) | NS | 4(20.0%) | 16(80.0%) | 0.008 |
| Usage of tooth paste with fluoride | No or don't know Yes | 89(33.2%) | 179(66.8%) | NS | 136(50.7%) | 132(49.3%) | 0.008 |
| Frequency of intake sweet foods | Rarely or never | 5(31.3%) | 11(68.8%) | NS | 9(56.3%) | 7(43.8%) | NS |
| Frequency of intake sweet foods | Rarely or never | 88(32.1%) | 186(67.9%) | NS | 133(48.5%) | 141(51.5%) | NS |
| Person who brush children's teeth | Sometime or frequently by themselves and helped by parents | 33(28.4%) | 83(71.6%) | NS | 54(46.6%) | 62(55.3%) | NS |
| Person who brush children's teeth | Sometime or frequently by themselves and helped by parents | 58(33.5%) | 115(66.5%) | NS | 85(49.1%) | 88(50.9%) | NS |
| Person who brush children's teeth | Sometime or frequently by themselves and helped by parents | 1(33.3%) | 2(66.6%) | NS | 2(66.7%) | 1(33.3%) | NS |
| Parents' socio- behavioral determinants | |||||||
| Income | < Rs. 10000 (100 USD)/month | 42(35.9%) | 75 (64.1%) | NS | 56(47.9%) | 61(52.1%) | NS |
| Income | >= Rs. 10000 (100 USD)/month | 48(30.2%) | 111 (69.8%) | NS | 77(48.4%) | 82(51.6%) | NS |
| Farther's education level | Below grade 10/ Ordinal level examination© | 67(32.7%) | 138 (67.3%) | NS | 97(47.3%) | 108(52.7%) | NS |
| Farther's education level | Advanced level examination/University level | 21(36.8%) | 36(63.2%) | NS | 33(57.9%) | 24(42.1%) | NS |
| Mother's education level | Below grade 10/ Ordinal level examination© | 71(33.0%) | 144(67.0%) | NS | 101(47.0%) | 114(53.0%) | NS |
| Mother's education level | Advanced level examination/University level | 19(27.5%) | 50(72.5%) | NS | 37(53.6%) | 32(46.4%) | NS |
| Knowledge** | Score 0-1 | 70 (28.0%) | 173 (71.2%) | NS | 112(46.1%) | 131(53.9%) | NS |
| Knowledge** | Score 2-3 | 62(37.3%) | 104(62.7%) | NS | 86(51.8%) | 80(48.2%) | NS |
Table 4: Difference in the determinants of oral health and deciduous dental caries.
*Number (%), NS: not significant © Grade 10 Final Examination/ Selection Exam for the Advanced level studies dmft1: the model was divided into 2 groups as a cut-off by caries free or not. dmft2: the model was divided into 2 groups as a cut-off point by median (50th percentile of children with number of dmft). The adapted scoring method was explained in the materials and methods. Table 4:** Difference in the determinants of oral health and deciduous dental caries.
were not significantly associated with dmft of the children (Table 5).
| Independent variable | Dependent variable {1:dmft>=3} | |||
| OR | P value | 95% CI | ||
| Usage of tooth paste with fluoride | No | 1 | 0.013* | 0.079-0.745 |
| Usage of tooth paste with fluoride | Yes | 0.243 | 0.013* | 0.079-0.745 |
| **Negelkerke R² | 0.034* |
Table 5: Association between usage of tooth paste containing fluoride and dmft.
Discussion
According to the results of this study, the prevalence of dental caries among children at mean age of 67.3 months (5 years and 7.3months) in Kandy District is 68% and it is in line with the reported prevalence for Ragama area in Gampaha district [10]. It is also similar to that of NOHS of Sri Lanka in 2003 [3, 11] in which the prevalence of 5 year age group was 65.31% after seven years. Therefore, Sri Lanka might belongs to the group that did not achieve the goal set by WHO and the FDI (International Dental Federation) in 1981, with focused effort on 50% caries free 5-6 year old children by the year of 2000 [12]. Further, when comparing the dmft of our study of 3.5±0 with the NOHS of Sri Lanka in 2003 [3] where it was 2.21 and with the study of Ragama where it is 1.41 [10] pointed out the high level of caries in our sample. These results indicate continuing moderate level of dental caries in the study area (Kandy, Central province) according to the WHO guidelines [9] in caries levels.
The high proportion of restored teeth (Care index – 10.6%) reported in this study is consistent with the findings of other developing countries [13, 14, 15] and comparable with the care index of the United Kingdom which is 12% across the country [16]. In contrast to our finding the reported CI was 4.72 for preschool children living in Ragama area in Gampaha district [10]. Our result indicates the high perception of treatment need with improvement of oral health care facilities both in the public and private sectors in the study area. Further it highlights the inadequacy of preventive programmes in Kandy District. It is interesting to note that this is inspite of the routine dental care offered to all public schoolchildren in Sri Lanka [3]. A study conducted in New South Wales in Australia has reported a mean dmft score of 1.5 where there oral health programmes which consist of oral health education, risk assessment and clinical care for preschool children [17].
Therefore, we suggest implementing oral health education, risk assessment and clinical care at preschool level to change the symptom-oriented dental treatment seeking pattern to prevention-oriented routine dental care seeking patterns in Sri Lanka. Since Sri Lanka has very effective immunization programmes, preventive dental care clinics may be effortlessly organized in parallel with them. As shown in the Table 4, the only oral health behavioral factor of 5-6 year old children which has a significant effect on the dental caries experience is the use of fluoridated tooth paste. A policy statement of World Dental Federation (FDI) has stated “fluoride tooth paste remains the most widespread and significant vehicle for fluoride used in prevention of tooth decay. Its effectiveness has been confirmed since the 1950’s in over one hundred clinical trials in children, adults and the elderly”. Further fluoride toothpaste is safe to use irrespective of low, normal or high exposure to fluoride from other sources [18, 19].
A Limitation of our study is lack of data on the quality of the tooth paste fluoride content, extent of brushing behavior, time spend for a single brushing process, frequency of tooth brushing and quality of tooth brushing. However, these factors may also affect the efficacy of tooth brushing with fluoride toothpastes. Therefore, further studies are warranted to elucidate the use of fluoride toothpaste in reduction of dental caries in our population.
Conclusion
According to the results of this study, prevalence of dental caries among 5-6 year old children in Kandy district is relatively high (68.8%) with approximately 90% (Care Index of 10.61%) of them having untreated caries. High dmft level of 3.5±0 in the study highlights the urgent need of interventional programmes aiming the improvement of oral hygiene among the children of this age group in Kandy District. Further, our results show that brushing teeth with fluoridated tooth paste is an important factor that reduces dmft of this population.
References
-
Petersen PE (2003) The World Oral Health Report 2003: continuous improvement of oral health in the 21st century-the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol 31(1): 3-23.
-
Jürgensen N, Petersen PE (2009) Oral health and the impact of socio- behavioural factors in a cross sectional survey of 12-year old schoolchildren in Laos. BMC Oral Health 9: 29.
-
(2003) Ministry of Health and Indigenous Medicine, Sri Lanka, National Oral Health Survey of Sri Lanka. Dental caries 28-39.
-
Ranasinghe N, Kruger E, Tennant M (2019) Spatial distribution of ground water fluoride levels and population at risk for dental caries and dental fluorosis in Sri Lanka. Int Dent J 69(4): 295-302.
-
Perera I, Ekanayake L (2010) Relationship between dietary patterns and dental caries in Sri Lankan adolescents. Oral Health Prev Dent 8(2): 165-172.
-
Ekanayake L, van der Hoek W (2002) Dental caries and developmental defects of enamel in relation to fluoride levels in drinking water in an arid area of Sri Lanka. Caries Res 36(6): 398-404.
-
Ekanayake L, van der Hoek W (2003) Prevalence and distribution of enamel defects and dental caries in a region with different concentrations of fluoride in drinking water in Sri Lanka. Int Dent J 53(4): 243- 248.
-
https://www.researchgate.net/publication/3314309 02_Determination_of_the_optimum_level_of_fluoride_f or_drinking_water_in_different_climatic_zones_of_Sri_ Lanka_based_on_the_ambient_temperature [accessed Aug 05 2019].
-
World Health Organization (1997) Basic principles of clinical oral health surveys: Dentition status: Oral Health Surveys, Basics Methods, 4th (Edn.), WHO, Geneve.
-
Perera PJ, Abeyweera NT, Fernando MP, Warnakulasuriya TD, Ranathunga N (2012) Prevalence of dental caries among a cohort of preschool children living in Gampaha district, Sri Lanka: A descriptive cross sectional study. BMC Oral Health 12: 49.
-
Ministry of Health, Nutrition and Indigenous Medicine, Sri Lanka. Annual health bulletin of Sri Lanka. (2014). Oral health services, 45-46.
-
Hobdell M, Petersen PE, Clarkson J, Johnson N (2003) Global goals for oral health 2020 Leader of FDI Joint Working Group. International Dental Journal 53: 285- 288.
-
Gao J, Ruan J, Zhao L, Zhou H, Huang R, et al. (2014) Oral health status and oral health knowledge, attitudes and behavior among rural children in Shaanxi, western China: a cross-sectional survey. BMC Oral Health 14: 144.
-
Kundu H, Patthi B, Singla A, Jankiram C, Jain S, et al. (2015) Dental Caries Scenario among 5, 12 and 15- Year-old Children in India- A Retrospective Analysis. J Clin Diagn Res 9(7): 1-5.
-
Hiremath A, Murugaboopathy V, Ankola AV, Hebbal M, Mohandoss S, et al. (2016) Prevalence of Dental Caries among Primary School Children of India-A Cross- Sectional Study. J Clin Diagn Res 10(10): 47-50.
-
Public Health England (2012) National Dental Epidemiology Programme for England: Oral health Survey of five-year-old children 2015. A report on the prevalence and severity of dental decay, 12.
-
Blinkhorn AS, Byun R, Johnson G, Metha P, Kay M, et al. (2015) The Dental Health of primary school children living in fluoridated, pre-fluoridated and non- fluoridated communities in New South Wales, Australia. BMC Oral Health 15: 9.
-
http://www.fdiworldental.org/media/11323/Promo ting-dental-health-through-fluoride-toothpaste- 2008.pdf.
-
Marinho VCC, Higgins JPT, Logan S, Sheiham A (2003) Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev (1): CD002278.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells