Comparison of Live Bacteria Aerosolization during Removal of Dental Enamel Using a 9.3μm CO2 Laser, a 2.78μm Erbium Laser and a High-Speed Dental Drill
Purpose: To measure the amount of viable pathogens in the aerosol/splatter generated during dental procedures using lasers and high-speed drill. Methods: Three systems were used in this in vitro study: 9.3μm CO2 laser, 2.78μm erbium laser and a high-speed drill. 45 uncleaned human molars were randomly selected to be used for the test groups for the three systems. Bacteria ejected while cutting the buccal or lingual surfaces were collected on tryptic soy agar (TSA) plates in identical conditions for each measurement. On the opposite surface of each tooth, a non-cutting mist spray was applied. Results: The CO2 laser resulted in colony-forming units (CFU) with a mean of 1570 ± 3850 CFU/m3/s, which is statistically different (p < 0.001) relative to both the erbium laser and the drill with a mean of 185,000 ± 182,000 CFU/m3/s and 440,000 ± 496,000 CFU/m3/s, respectively. CFU measured from the non-cutting mist spray on the teeth was higher for the drill than for the lasers. Conclusion: The 9.3μm CO2 laser resulted in the lowest CFU in the aerosol/splatter during enamel removal as compared to that of the 2.78μm erbium laser and the traditional high-speed drill. Furthermore, the CO2 laser was the only system that did not increase aerosolization of bacteria while cutting compared to the non-cutting mist spray.
Introduction
The severe acute respiratory syndrome coronavirus (SARS-CoV-2) has presented challenges to healthcare providers worldwide-particularly dental practitioners, who’s proximity to the airways of their patients while working makes them vulnerable for infection by these airborne pathogens. The risk of dental professionals contracting the virus is exacerbated by aerosols produced during dental procedures. Recent studies have shown evidence that SARS- CoV-2 can originate from saliva, [1] and dental procedures that aerosolize the saliva present on tooth surfaces have the potential to infect dental clinicians [2, 3]. The aerosolized droplets also have a potential to contaminate dental clinic surfaces, with a half-life of up 5.6 hours on stainless steel surfaces and 6.8 hours on plastic surfaces, and larger particles may continue to release bioaerosols as they evaporate [4, 5]. These dangers have encouraged recent studies investigating the bacteria contamination of dental aerosols.
Microbiological methods have been used to gauge the level of bacterial contamination in aerosols generated from the use of dental instruments during routine procedures such as cavity preparations. These methods often use agar plates through sedimentation, which are often left open in specified locations throughout the room [6, 7] or held open close to the operating site [8, 9] during the procedure to collect airborne bacteria. After collection, the plates are then incubated at 35-37°C for 24-48 hours [8, 9, 10] so that bacteria colony formation becomes countable. In these studies, colonies are reported by colony forming units (CFU), which corresponds to the number of aerosolized bacteria [11, 12].
This study aimed to compare the live bacterial content during a mock aerosol-generating procedure for the removal of dental enamel using a 9.3μm CO2 laser, a 2.78μm erbium laser and a high-speed dental drill. The use of the laser to vaporize tissues has been thought to drastically increase the temperature of the targeted tissue to the point where any pathogens are destroyed [13, 14]. However, mist water is then used to cool the tooth, and droplets of water may absorb the pathogens and carry them in an aerosol [15, 16]. Drilling instruments use water cooling as well, but with much greater air pressure and mist flow rates [17]. In addition, the use of the drill involves significantly more mechanical force, which, combined with the greater mist flow and air pressure, makes the drill likely to release more live pathogens into the air than laser ablation. As far as we know, this study is the first to directly compare the aerosolization of bacteria while cutting enamel using dental lasers and a high-speed drill.
Materials and Methods
Study Devices
• A 9.3μm CO2 laser (Solea, Convergent Dental, Inc., Needham, MA) was used with laser irradiation at recommended settings of 30% cutting speed (~8.3 W), with a mist flow of 9 mL/min, and low air pressure (10 psi) using the 1.25 mm spot size.
• A 2.7μm Er,Cr:YSGG laser, (Waterlase iPlus, BIOLASE, Inc., Foothill Ranch, CA) in H mode with a Turbo handpiece and MX5 tip was used with selected settings for cutting enamel will be used at common settings of 8.0 W, 15 Hz, air at 70%, and water at 50%. These setting produced a similar mist flow at a similar power to the CO2 laser.
• A dental drilling unit (Adec PAC 1 Institutional Unit, A-dec, Inc., Newberg, OR) was used at the nominal system air pressure of 80 psi. A carbide bur FG 330 was used with a drill handpiece (Midwest Stylus 360S, Dentsply Professional, Des Plaines, IL) at a nominal pressure of 40 psi that corresponds to about ~400,000rpm, and mist flow of the drill was measured at 25 mL/min.
Samples
• A total of 60 fresh human molars were obtained from oral surgery offices within a few weeks of the experiment and initially immersed in a 0.1% thymol solution to prevent additional bacterial growth and stored in a container with paper towels soaked in distilled water to prevent dehydration.
• Test Groups: A total of 45 molars (15 teeth per system) were used. No further pretreatment was performed on the molars prior to running the experiment.
• Control Groups: A total of 15 molars (5 teeth per system) were initially sterilized after extraction in 1.0% thymol solution for several hours and rinsed with DI water. Prior to measurements, the molars were sterilized in 70% ethanol for 30 seconds while gently stirring. The molars were then mounted in clay and air-dried prior to taking measurements. These groups were included in the experiment to check for exogenous sources of bacteria such as from mist lines.
• Background Control Group: 5 background controls measurements were obtained by leaving the plates exposed to the air in the same position as the test plates for the same duration of time at the end of the experiment to check for environmental cross-contamination.
Setup
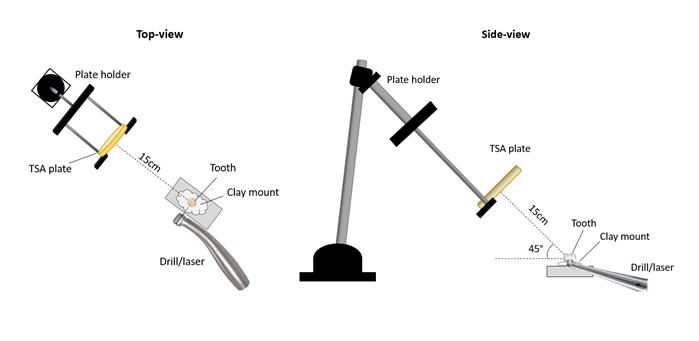
This study was performed in a controlled laboratory benchtop setting in a fume hood environment using trypic soy agar (TSA) plates (Eurofins EMLab P&K laboratories, Marlton, NJ). The plates were positioned at 15 cm from the sample tooth at a vertical angle of ~45°, as shown in Figure 1, which allowed aerosolized live bacteria to be seeded onto the plate in the direction that a practitioner would commonly be seated. The plates were exposed for 10 seconds during each of the aerosol-generating procedures to standardize exposure to the initial maximum output of pathogenic aerosol and splatter from the enamel surface.
Cutting Procedure
For each measurement, the handpieces of the laser or the drill were carefully scanned over an entire buccal or lingual surface for 10 seconds, using the same zigzagging motion for all samples and surfaces. After 10 seconds, the labeled plates were immediately lidded and taped with the lid down to prevent condensation. The plates were incubated at 37oC for 24 hours, after which the bacterial colonies were counted on each plate. The entire experiment was conducted in a fume hood, which was turned off during measurements but turned on for at least 30 seconds between measurements to clear the air and reduce measurement interference. In addition, the mount for holding the TSA plates was cleaned with disinfectant wipes between each measurement. Standard aseptic techniques were followed. All surfaces were wiped with alcohol disinfecting wipes and 70% ethanol prior to the experiment. Gloves were used at all times, and 70% ethanol spray was used to clean gloves before touching sterile plates. Between each measurement, all surfaces around the tooth area and in the path of the plates, including around the mounts for the plates and teeth, were disinfected.
Non-Cutting, Mist Spray Procedure
To determine if the predominate source of aerosolized bacteria is from the mist spray or from the direct action of cutting the enamel, additional testing was performed on the opposite surfaces of the molars (lingual or buccal), using the same 45 molars. This testing used mist spray without cutting. For the lasers, the laser output was turned off, and for the drill, the drill bit was held close to the enamel surface without making direct contact. The movement of the handpiece was identical as for the cutting procedure, and the plates were also handled identically.
Plate Counting
A semi-automated counting was performed using ImageJ [18] to provide bacteria colony counts for each TSA plate. This process involved cropping and filter the countable area of the TSA plate, and adjusting the image thresholds to produce an image that clearly distinguishes the bacteria colonies (in white) from the background (in black), as shown in Figure 2.
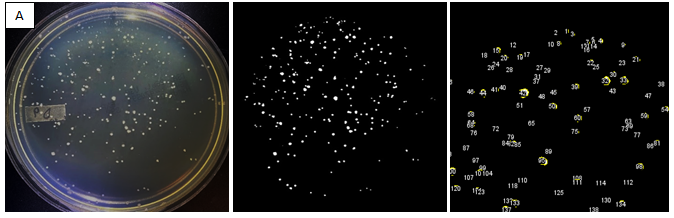
This new image was then checked to ensure the colonies shown aligned with the colonies from the original image before the ‘analyze particles’ feature was used to count them. Any colonies detected near the outer edges of the TSA plate were counted manually and added to the count from ImageJ to provide the total count for each plate.
Colony-Forming Units (CFU) Calculation
CFU values were calculated by the formula (CFU= [5*104*x]⁄([area (cm2 )*time (min)], [19, 20, 21] where x is the number of colonies on a plate. For all measurements, the exposed area of the TSA plates was 63.6 cm2 and the duration of the exposure was 10 seconds.
Statistics
Statistical analysis of the data was performed using Minitab 18 (Minitab LLC, Pennsylvania, USA). Mann-Whitney U tests were performed to report p-values for pairwise comparisons of test groups. These tests have been suggested previously for this type of dataset [22].
Statement of Ethical Approval
The human molar samples used in this study were originally planned for extraction. This is an in-vitro study that did not require an Institutional Review Board approval and inclusion of human subjects.
Results
Figure 3 shows representative images of each test groups used in the study. The top row (A-C) are images of the TSA plates used during collection of the aerosol/splatter while cutting enamel with each device. Plates for the 9.3-μm CO2 laser showed a minimal number of colonies, whereas plates for the 2.78-μm erbium laser showed significantly more. The high-speed drill produced the largest average colony counts. The bottom row of images in Figure 3 are representative TSA plates for measurements of the test groups for non-cutting mist spray to the enamel surfaces for each device.
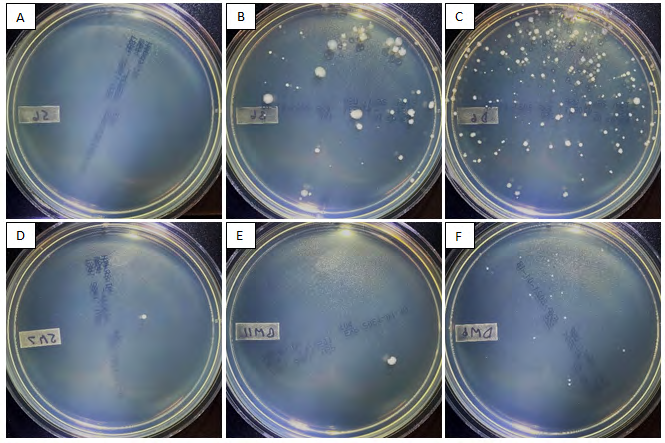
Figure 3: The top row shows representative images of TSA plates with bacteria colonies produced by cutting with (A) CO2 laser (B) Erbium Laser and (C) the high-speed drill. The bottom row shows representative images of TSA plates with bacteria colonies produced by non-cutting application of mist from the (D) CO2 laser handpiece, (E) Erbium laser handpiece, and (F) drill with no contact.
Table 1 lists the average CFU for all groups, as calculated from the number of colonies on each of the TSA plates. For the enamel-cutting procedures, the CO2 laser resulted in the lowest CFU (1570± 3850 CFU/m3/s), the erbium laser produced a mean of 185,000± 182,000 CFU/m3/s, and the high-speed drill produced the highest mean of 440,000± 496,000 CFU/m3/s. The number of colonies measured during the non-cutting spray of mist on the enamel surface for each system showed that the lowest CFU was produced by the erbium laser handpiece (943 ±1940 CFU/m3/s), followed closely by the CO2 laser handpiece (3770 ±12300 CFU/m3/s).
The high-speed drill mist spray (no contact with the drill bit on the enamel surface) produced a substantially higher CFU at 78,900± 148,000 CFU/m3/s).
| Total samples | Mean CFU (std) | |
|---|---|---|
| Ambient air | n = 5 | 0.0 (0.0) |
| CO2 laser control | n = 5 | 943 (2100) |
| Erbium laser control | n = 5 | 943 (2100) |
| Drill control | n = 5 | 943 (2100) |
| CO2 (mist) | n = 15 | 3770 (12300) |
| Erbium (mist) | n = 15 | 943 (1940) |
| Drill (mist) | n = 15 | 78900 (148000) |
| CO2 (cutting) | n = 15 | 1570 (3850) |
| Erbium (cutting) | n = 15 | 185000 (182000) |
| Drill (cutting) | n = 15 | 440000 (496000) |
Table 1: Mean colony-forming units (CFU) for each sample group.
Figure 4a shows a box plot of the CFU data from Table 1 for the cutting procedure on a logarithmic scale, while Figure 4b shows the data for the non-cutting mist spray procedure. During the enamel-cutting procedure, CFU for the CO2 laser were lower on average than those measured for the erbium and high-speed drill systems. During the non-cutting mist spray procedures, CFU for the CO2 and erbium systems were lower on average than for the drill. Mean CFU for the CO2 system was lower during the cutting procedure relative to the non-cutting mist spray procedure. Contrarily, for the erbium and drill systems, cutting enamel produced a higher mean CFU relative to the non-cutting mist spray.
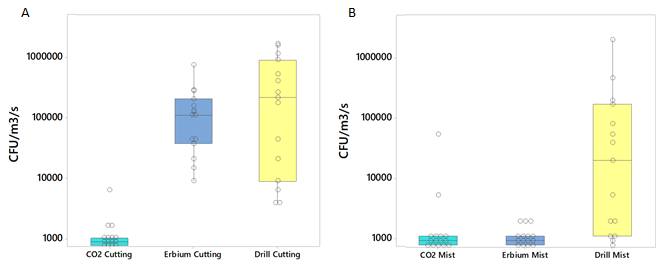
Figure 4: (A) A boxplot of CFU measured in the aerosol/splatter generated while cutting enamel for each test group, shown on a logarithmic scale. Open circles represent a single plate measurement. (B) A boxplot of CFU measured in the aerosol/splatter generated during a non-cutting mist spray from each handpiece on enamel (non-cutting) for each test group are also shown on a logarithmic scale. Open circles represent a single plate measurement.
Pairwise comparisons of the test groups were performed using the Mann-Whitney U test. The p-values from each of these comparisons are shown in Table 2. For the non-cutting, mist spray experiment, CFU measurements of the CO2 laser were not significantly different from the CFU produced by non-cutting mist spray from the CO2 laser handpiece.
However, the CFU produced from non-cutting mist spray with the erbium or drill systems were significantly less than those produced while cutting enamel with either system. The CFU measured from cutting with the erbium laser was not significantly different than that produced from cutting with the drill.
| Drill (cutting) | Erbium (cutting) | CO (cutting) 2 | Drill (mist) | Erbium (mist) | |
|---|---|---|---|---|---|
| CO (mist) 2 | p < 0.001 | p < 0.001 | p > 0.05 | p = 0.001 | p > 0.05 |
| Erbium (mist) | p < 0.001 | p < 0.001 | p > 0.05 | p = 0.001 | − |
| Drill (mist) | p = 0.008 | p = 0.007 | p = 0.001 | − | − |
| CO (cutting) 2 | p < 0.001 | p < 0.001 | − | − | − |
| Erbium (cutting) | p > 0.05 | − | − | − | − |
Table 2: Mann-Whitney U test p-values from pairwise comparisons of test groups.
Discussion
The risk of disease transmission from patient to practitioner has presented a challenge for vulnerable healthcare workers, and in particular dentists [23]. To reduce this risk, much work has been done to identify technologies or techniques that can reduce the aerosol and splatter generation during dental procedures [15, 24, 25]. Laser irradiation may be thought to be a safer alternative to traditional dentistry due to the heating effect from absorbed laser energy [14, 26]. Conversely, the non-heating effect of mechanical removal from a dental drill is expected to eject particles, including live pathogens, from the enamel surface at far distances [3, 12]. In this study in a controlled laboratory environment, we investigated three devices, a 9.3μm CO2 laser, a 2.78μm erbium laser, and a traditional high-speed dental drill, for their relative degrees of safety during a procedure in cutting dental enamel.
The best performance was obtained by the CO2 laser, which aerosolized a minimal number of detected bacteria both during the cutting procedure and during the non- cutting mist spray. The mean CFU was lower for the cutting group, but due to very low colony counts for the CO2 laser, there was no statistical difference between the groups. At a closer distance, a significant difference may be found. Nonetheless, the increased ejection of debris while cutting did not produce a larger number of aerosolized bacteria. This aligns with the hypothesis that the high temperature reached on the enamel surface using 9.3μm CO2 laser irradiation [14] helps to decontaminate at least some of the aerosolized surface debris. Further studies may be done to investigate this.
The significantly lower measurements of bacteria in the air from the CO2 laser may be explained by the strong absorption of CO2 lasers by the phosphate groups in hydroxyapatite (particularly at 9.3 and 9.6 µm) [27], which causes the enamel to heat rapidly to several thousand degrees Celsius from this direct absorption and vaporize, resulting in ablation [14]. Erbium lasers, however, are targeted mainly by water on and in the tooth structure, which causes micro- explosive effects [27, 28] when the water is vaporized inside and around the tooth, which adds to the generation of splatter and aerosol which may harbor bacteria.
Contrary to the CO2 laser, the erbium laser and drill systems both produced significant numbers of aerosolized bacteria while cutting enamel. Furthermore, for the drill and erbium systems, this large number of aerosolized bacteria while cutting was significantly greater than that produced by the non-cutting mist sprays. CFU from the non-cutting mist sprays followed a logical trend of increased mist spray resulting in higher CFU measurements, as demonstrated by the drill system CFU relative to the two laser systems. The same was not true for the cutting groups, in which the erbium laser produced numbers not significantly different from the drill. The drill likely produced large CFU numbers due to the forceful mechanical ejection of surface material with bacteria latched onto the particles [29]. The erbium laser causes micro-explosions of water near the surface that blast particles away, [28] which brings along live bacteria. This was verified with in the study presented here in which a non-cutting spray of mist from the erbium system handpiece was applied to the enamel and generated colony counts similar to the CO2 system handpiece.
No background contamination was detected, and the sterile tooth control measurements showed that the procedure worked as expected, with negligible colonies detected. This indicated that the CFU reported was entirely from bacteria coming from the enamel surface mimicking real dental clinic situation. This study was not done with a high-vacuum evacuation, which would further reduce the detected bacteria, particularly for the smallest particle sizes [30, 31]. Regardless, measurements for the CO2 laser system were already very low. This demonstrates that the 9.3 μm CO2 laser is a safe device to use for dental procedures where a reduction in the risk of disease transmission is paramount.
Conclusion
The 9.3μm CO2 laser generated the lowest number of aerosolized bacteria during an enamel cutting procedure, when compared to a 2.78μm erbium laser or a traditional high-speed dental drill. The CO2 laser while cutting did not produce more bacteria than when simply applying a non- cutting mist spray, unlike for the erbium laser or the drill. This demonstrated that the CO2 is a safe device to use while cutting enamel to reduce the spread of disease in a dental setting.
References
-
Xu J, Li Y, Gan F, Du Y, Yao Y (2020) Salivary glands: potential reservoirs for COVID-19 asymptomatic infection. J Dent Res 99(8): 989.
-
Schwendicke F (2020) Saliva is a potential source of Covid-19, and appropriate protection measures should be applied in dental practice. Evid Based Dent 21(2): 62.
-
Aldahlawi SA, Afifi IK (2020) COVID-19 in Dental Practice: Transmission Risk, Infection Control Challenge, and Clinical Implications. Open Dent J 14(1): 348-354.
-
Ortega KL, de Camargo AR, Franco JB, Azul AM, Sayáns MP, et al. (2020) SARS-CoV-2 and dentistry. Clin Oral Investig 24(7): 2541-2542.
-
Chanpong B, Tang M, Rosenczweig A, Lok P, Tang R (2020) Aerosol-generating procedures and simulated cough in dental anesthesia. Anesth Prog 67(3): 127-134.
-
Rautemaa R, Nordberg A, Saaristo KW, Meurman JH (2006) Bacterial aerosols in dental practice-a potential hospital infection problem?. J Hosp Infect 64(1): 76-81.
-
Bentley CD, Burkhart NW, Crawford JJ (1994) Evaluating spatter and aerosol contamination during dental procedures. J Am Dent Assoc 125(5): 579-584.
-
Nayak SU, Kumari A, Rajendran V, Singh VP, Hegde A, et al. (2020) Comparative evaluation of efficacy of chlorhexidine and herbal mouthwash as a preprocedural rinse in reducing dental aerosols: a microbiological study. Int J Dent 2020: 1-6.
-
McKinley IB, Ludlow MO (1994) Hazards of laser smoke during endodontic therapy. J Endod 20(11): 558-559.
-
Guida M, Gallé F, Onofrio VD, Nastro RA, Battista M, et al. (2012) Environmental microbial contamination in dental setting: A local experience. J Prev Med Hyg 53(4): 207-212.
-
Zemouri C, Volgenant CMC, Buijs MJ, Crielaard W, Rosema NAM, et al. (2020) Dental aerosols: microbial composition and spatial distribution. J Oral Microbiol 12(1): 1762040.
-
Bennett AM, Fulford MR, Walker JT, Bradshaw DJ, Martin MV, et al. (2000) Microbial aerosols in general dental practice. Br Dent J 189(12): 664-667.
-
Cazares LH, Van Tongeren SA, Costantino J, et al. (2015) Heat fixation inactivates viral and bacterial pathogens and is compatible with downstream MALDI mass spectrometry tissue imaging. BMC Microbiol 15(1): 1-11.
-
Fried D, Seka WD, Glena RE, Featherstone JD (1996) Thermal response of hard dental tissues to 9‐ through 11‐μm CO2‐laser irradiation. Opt Eng 35(7): 1976-1984.
-
Harrel SK, Molinari J (2004) Aerosols and splatter in dentistry: A brief review of the literature and infection control implications. J Am Dent Assoc 135(4): 429-437.
-
Epstein JB, Chow K, Mathias R (2020) Dental procedure aerosols and COVID-19. Lancet Infect Dis 21(4): 73.
-
Cavalcanti BN, Serairdarian PI, Rode SM (2005) Water flow in high-speed handpieces. Quintessence Int 36(5): 361-364.
-
Schneider CA, Rasband WS, Eliceiri KW (2012) NIH Image to ImageJ: 25 years of image analysis. Nat Methods 9(7): 671-675.
-
Hayleeyesus SF, Manaye AM (2014) Microbiological quality of indoor air in University libraries. Asian Pac J Trop Biomed 4(1): 312-317.
-
Borrego S, Guiamet P, de Saravia SG, Batistini P, Garcia M, et al. (2010) The quality of air at archives and the biodeterioration of photographs. Int Biodeterior Biodegrad 64(2): 139-145.
-
Sundri MI (2018) Bacteria and fungi levels in crowded indoor areas. IOSR J Environ Sci 12(9): 39-45.
-
Xia Y, Sun J (2017) Hypothesis testing and statistical analysis of microbiome. Genes Dis 4(3): 138-148.
-
Slots J, Slots H (2000) Bacterial and viral pathogens in saliva: Disease relationship and infectious risk. Periodontol 55(1): 48-69.
-
Leggat PA, Kedjarune U (2001) Bacterial aerosols in the dental clinic: A review. Int Dent J 51(1): 39-44.
-
Zemouri C, Soet HD, Crielaard W, Laheij A (2017) A scoping review on bio-Aerosols in healthcare & the dental environment. PLoS One 12(5): e0178007.
-
Jabbar Ali B, Hamzah B, Naji E (2015) Effect of CO2 laser on peri-implant infections. Hamzah al World J Pharm Res World J Pharm Res 4(7): 110-122.
-
Featherstone JDB, Fried D (2001) Fundamental interactions of lasers with dental hard tissues. Med Laser Appl 16(3): 181-194.
-
Diaci J, Gaspirc B (2012) Comparison of Er:YAG and Er, Cr:YSGG lasers used in dentistry. J Laser Heal Accademy 2012(1): 1-13.
-
Allison JR, Currie CC, Edwards DC, Bowes C, Coulter J, et al. (2021) Evaluating aerosol and splatter following dental procedures: addressing new challenges for oral healthcare and rehabilitation. J Oral Rehabil 48(1): 61-
-
Dahlke WO, Cottam MR, Herring MC, Leavitt JM, Ditmyer MM, et al. (2012) Evaluation of the spatter-reduction effectiveness of two dry-field isolation techniques. J Am Dent Assoc 143(11): 1199-1204.
-
Avasthi A (2018) High Volume Evacuator (HVE) in reducing aerosol- an exploration worth by clinicians. J Dent Heal Oral Disord Ther 9(3): 1-2.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells