Use of 9.3μm CO2 Laser for Removal of Zirconia Restorations
Objective: The primary aim of this study was to test if a 9.3µm Carbon Dioxide (CO2 ) laser could be used to effectively separate a cemented zirconia restoration from dentin. The secondary aim was to compare shear bond strength (SBS) between RelyXTM Unicem 2 Automix Cement (3M ESPE) (RelyXTM Unicem 2) and RelyXTM Luting Plus Automix Cement (3M ESPE) (RelyX™ Luting Plus). Methods: 40 teeth were prepared to expose dentin and then randomized into four groups of 10 samples. Zirconia slices (non-glazed Yttrium stabilized zirconia samples (2.5 x 3 x 1.5 mm)) were sandblasted with 50 micron aluminum oxide at 30 psi and then cemented onto the dentin samples with RelyX™ Unicem 2 or RelyX™ Luting Plus, dependent on the group. The cements were applied to both the zirconia and dentin with a force of 20 g/mm2 for 30 seconds following manufacturer’s recommendations. After 48 hours, the 9.3µm CO2 laser was used on half the samples for 5 seconds. All 40 zirconia samples were removed with the Instron 5566A in a traditional SBS test. The groups were: 1A - RelyX™ Unicem 2 and Laser, 1B - RelyX™ Unicem 2 and Shear Bond, 2A - RelyX™ Luting Plus and Laser, and 2B - RelyX™ Luting Plus and Shear Bond. The Mann–Whitney U test was used for comparison. Results: Mean SBS of four groups ranged from 0.5 to 4.4 MPa. There was a significant difference in the SBS between 9.3µm CO2 laser and Shear Force methods for RelyX™ Luting Plus. However, the difference between the two methods was not significant for RelyX Unicem 2. RelyX™ Unicem 2 provided significantly higher SBS than RelyX™ Luting Plus for both the CO2 laser and shear force methods (Table 2). Conclusion: The 9.3µm CO2 laser effectively separated the zirconia restoration cemented with RelyX™ Luting Plus from dentin. RelyX™ Unicem 2 provided significantly stronger SBS than RelyX™ Luting Plus.
Introduction
Crown placement involves preparation of the tooth, removing enamel, creation of a crown, adjusting of the crown, and its cementation to the remaining tooth structure [1]. It is important to use restorative materials that can withstand large amounts of occlusal forces. Due to its strength and esthetic properties, zirconia is becoming widely used in dentistry for restorations including crowns [2]. However, when crowns need to be replaced due to development of carious lesions or fractures, the crown removal process is time consuming. It typically includes using diamond burs to cut the zirconia crown with the use of a high-speed handpiece at 150,000 rpm and a 0.9 N cutting force [2]. This process is followed by torquing the edges to shear the crown.
Several lasers have been developed over the last couple of decades in dentistry [3, 4]. Such lasers include CO2, Neodymium Yttrium Aluminum Garnet (Nd: YAG), and Er:YAG and can be used on soft or hard tissues. Soft tissue laser uses include healing of injured tissue, exposing impacted or partially erupted teeth, and cancer therapies [4]. Laser usage on hard tissue includes removing restorative material, bleaching, preventing tooth sensitivity, and preventing cavities [4]. Additionally, the CO2 laser has been successful in increasing caries resistance of enamel [5, 6, 7, 8].
Important factors for selecting a dental technique are patient comfort, chair time, and cost. Concerning crown removal, it is time consuming to use burs and handpiece instruments, which additionally generate heat [3]. Hard tissue lasers provide an alternative form of ceramic crown removal. Reducing the number of burs will decrease the cost of constant bur replacement during crown removal. Another advantage of using a laser is the reduction of the noises and vibrations experienced with a high-speed instrument, and the associated discomfort experienced by the patient [3]. Lasers prove to be successful in increasing efficiency and comfort while decreasing costs of dental procedures.
Many dentists and researchers alike are looking for possible alternatives to using burs and shear force to remove crown restorations. One study was conducted using an Erbium-doped Yttrium Aluminium Garnet (Er:YAG) laser to debond and remove the crown from the tooth structure. Both zirconia and lithium disilicate crowns were removed using this laser with no fractures or damage to the tooth structure or the crown [9]. The ability of the Er:YAG laser on crown removal leads to the potential use of another laser, the CO2 laser, for the same purpose.
A total of 40 blocks of zirconia were used in this study. Molar and premolar teeth were collected from oral surgery offices in the greater Chicago area and stored in a solution of 10% Clorox bleach in water until used. 40 molars and premolars were embedded into cylindrical acrylic resin blocks and sliced with the IsoMet saw at 850 rpm to expose the dentin of each sample. The non-glazed Yttrium stabilized zirconia samples (2.5 mm x 3 mm x 1.5 mm (length x width x thickness)) were obtained from Stanford Advanced Materials. The zirconia samples as well as the dentin samples were randomized into four groups, namely Group 1A (RelyXTM Unicem 2, Laser), Group 1B (RelyXTM Unicem 2, Shear Bond), Group 2A (RelyXTM Luting Plus, Laser), Group 2B (RelyXTM Luting Plus, Shear Bond) with 10 samples in each group. Each zirconia block was cemented to the dentin tooth slice with the cement outlined in Table 1 (as it mimics zirconia crown restorations).
The Er:YAG laser has shown to be successful in eliminating cement from the tooth structure [4]. Due to its affinity for water, it is also useful in hard tissue treatment [4]. Likewise, the CO2 laser has an affinity for water [4]. Since the two lasers share this water affinity characteristic, the removal of cement and restorations which has been confirmed with the use of the Er:YAG laser may also be possible with the use of the CO2 laser. Cemented zirconia restorations can be very challenging to remove, as the bonding can be very strong. Cranska reported the crown was removed within one minute with the use of an Er:YAG laser [3]. An Er:YAG laser is effective in removing all-ceramic restorations including zirconia crowns [3, 9].
Er:YAG lasers, along with CO2 lasers have been used in the dental industry for surface treatment of restorations. Er:YAG lasers were found successful at increasing shear bond strength (SBS) after surface treatment [11]. 9.3µm CO2 lasers also increased SBS after surface treatment [10, 11, 12, 13, 14, 15]. Based on the concept that the Er:YAG laser can successfully debond the crown from the tooth, it was hypothesized that a 9.3µm CO2 laser could also separate zirconia from tooth structure.
The aims of the study were primarily to determine if a 9.3µm CO2 laser could separate cemented zirconia from underlying tooth structure and secondarily to compare SBS between cements.
Materials and Methods
| Group 1A | Group 1B | Group 2A | Group 2B | |
|---|---|---|---|---|
| Cement | RelyXTM Unicem 2 | RelyXTM Unicem 2 | RelyXTM Luting Plus | RelyXTM Luting Plus |
| Treatment | Laser | Shear bond strength | Laser | Shear bond strength |
Table 1: Group Outline and Conditions.
Sample Preparation
All zirconia samples were sandblasted with 50 micron aluminum oxide at a pressure of 30 psi, cleaned with alcohol, and air dried. All cements were applied to both the zirconia and dentin and cemented with a constant force of
20 g/mm2 for 30 seconds, following the manufacturer’s recommendations. More specifically, for Group 1A and 1B with RelyXTM Unicem 2, the samples were tack cured with a DemiTM Plus Curing Light for 2 seconds, excess cement was removed with an explorer while holding the slices together, then light cured for another 20 seconds. Any excess cement was removed after an additional 6 minutes. For Group 2A and 2B with RelyXTM Luting Plus, the working time of the cement is 1.5 minutes according to the 3M manufacturer’s recommendations. The samples were tack cured with a DemiTM Plus Curing Light for 5 seconds, excess cement was removed with an explorer while the slices were held together. The cement was left to set for an additional 5 minutes prior to removing any other cement excess with an explorer.
The cemented samples were stored in water for 48 hours. As recommended by the manufacturer, the 9.3µm CO2 laser (Solea, Convergent Dental, Needham, MA) was set to a 1 mm spot size with an average power of 23.6 W. Laser irradiation was performed for 5 seconds continuously on each sample positioned at the laser’s focal point, which is 10 mm from the tip of the handpiece (Figure 1). The 9.3µm CO2 laser was used only on samples of Group 1A and 2A. Zirconia and dentin separation was determined by visual inspection of each sample. For those samples that the zirconia was not separated with the use of the CO2 laser, the SBS was tested using the Instron 5566A model at 1 mm/minute crosshead speed and recorded. For group 1B and 2B samples, the SBS was tested using the Instron 5566A model at 1 mm/minute crosshead speed and recorded for each sample without treatment of the CO2 laser. This machine is a universal testing device. One of its many tests is cements’ adhesive ability. This study used the Instron 5566A to test the adhesion between the zirconia ceramic and the tooth structure. SBS is important to demonstrate the force needed to separate the zirconia.

Sample Size
The sample size calculation was performed using nQuery Advisor. Since literature on CO2 lasers was sparse and could not be used for calculating sample size, the sample size was calculated based on the secondary aim (comparing SBS of RelyXTM Unicem 2 and RelyXTM Luting Plus) of the study. Based on the results of Blatz MB, et al. the mean±SD SBS of RelyXTM Luting Plus and RelyXTM Unicem 2 were assumed to be 5.75±1.53 MPa and 10.95±4.28 MPa respectively [16]. Based on these assumptions, a sample size of n=10 samples per group would provide 90% power to detect an effect size of 1.618 with a Type I error rate of 0.05.
Statistical Analysis
Means, standard deviations, medians and interquartile ranges were calculated for SBS. Normality of SBS data was assessed graphically and using the Shapiro-Wilk test. The Mann Whitney U test was used to compare SBS between the laser and shear force method for each cement. It was also used to compare SBS between RelyX Unicem and RelyX Luting for each method. Stata version 16 was used for analyses and significant value was set at 0.05.
Results
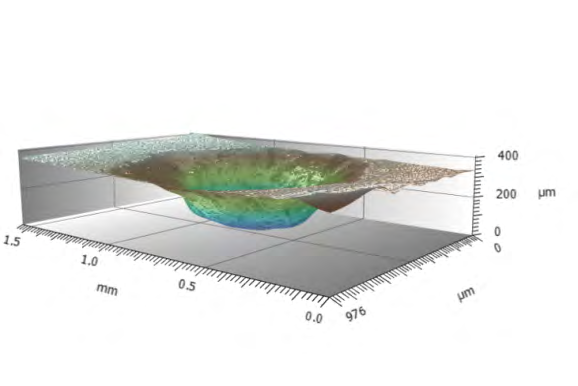
The mean SBS and standard deviations of each of the four groups are presented in Table 2, ranging from 0.5 to 4.4 MPa. 1 of the 10 samples in the RelyXTM Unicem 2 laser group and 5 of the 10 samples in the RelyXTM Luting Plus laser group successfully separated with the use of the laser only and did not undergo the SBS test with the Instron 5566A. It was determined that there was a statistically significant difference in SBS between the use of the laser and shear force method for RelyXTM Luting Plus, with a p-value of 0.01. However, the difference was not statistically significant between the two methods for RelyXTM Unicem 2, with a p-value of 0.20. SBS of RelyXTM Unicem 2 was significantly higher than RelyXTM Luting Plus for both the laser method and shear force method, with p-values of 0.04 and 0.03 respectively. Figure 2 is a 3D rendering of the zirconia block after the CO2 laser was used on the zirconia sample.
| RelyX™ Unicem 2 | RelyX™ Luting Plus | p** | |
|---|---|---|---|
| CO Laser 2 | 3.4 ± 4.3 | 0.5 ± 0.9 | 0.04 |
| Shear Force | 4.4 ± 2.4 | 2.0 ± 2.0 | 0.03 |
| p* | 0.2 | 0.01 |
Table 2: ** Shear bond strength (SBS) in MPa of four groups.
Data was presented as mean and standard deviation. p*: p-value for comparison between methods (primary aim) p: p-value for comparison between cements (secondary aim) Table 2:** Shear bond strength (SBS) in MPa of four groups.
Discussion & Conclusion
The primary aim of this study was to identify the correlation between the use of a CO2 laser to the use of shear force in assessing the separation of zirconia blocks cemented to dentin. The results from this study suggest that the CO2 laser can be used to remove zirconia from underlying tooth structure when cemented with RelyXTM Luting Plus.
The secondary aim of this study was to compare the SBS of the cements. The results were conclusive with previous literature that RelyXTM Unicem 2 has a higher SBS than RelyXTM Luting Plus [16, 17], which may contribute to the difficulty in removing zirconia from dentin with the laser when cemented with RelyXTM Unicem 2 compared to RelyXTM Luting Plus. This may suggest that a longer laser time, higher laser pattern, or modified pulse rate might be needed in order to successfully remove the zirconia from dentin when cemented with RelyXTM Unicem 2.
It is also important to note the solubility and absorption of the two cements. RelyXTM Luting Plus is a resin modified glass ionomer cement, while RelyXTM Unicem 2 is a self- adhesive universal resin cement. RelyXTM Unicem 2 [18, 19] has a lower solubility and lower sorption than RelyXTM Luting Plus [20]. Higher solubility and water sorption signifies higher water content. The water content in the cement affects the laser energy necessary to separate the zirconia from tooth structure. The higher the water content in the cement, a decreased amount of laser energy should be needed to debond the two surfaces [4]. Er:YAG laser energy is mostly absorbed in water [4, 5, 9, 11]. The CO2 laser also has a very large affinity for water [4]. This could yield in less water activation from the laser with the RelyXTM Unicem 2 samples, causing it to be more difficult to separate the zirconia from dentin.
There are currently two theories for the absorption process. The free volume approach hypothesizes that water molecules disperse in the voids of the resin in which they interact with, which may cause hydrolytic degradation [19]. Another theory suggests bonding of water and the cement’s hydrophilic groups, such as phosphate groups, causing hygroscopic expansion [19].
Although both the 9.3µm CO2 laser and the Er:YAG laser have a high affinity for water, the Er:YAG laser’s emission wavelength is located at the peak of water absorption, resulting in a 10 to 15 fold stronger affinity for water than the CO2 laser [21]. On the other hand, the CO2 laser emission wavelength’s absorption is predominantly in ceramics [11, 12, 13, 15]. Because of this, the 9.3µm CO2 laser can cause porosities in the zirconia [11, 13], which in turn may weaken the bond between the zirconia and cement, instead of weakening the cement itself through the cement’s water content.
In practice, it is beneficial to dentists to have additional ways to complete a procedure. Many dentists already use 9.3µm CO2 lasers for surface treatment. This study determined that 9.3µm CO2 lasers could be used to separate zirconia from the tooth structure when cemented with RelyXTM Luting. Based on the results of this study, additional testing will need to be performed to confirm if this bench method could be used clinically. Next steps to consider include using zirconia crowns instead of blocks and using a thermocouple at the interface of the zirconia and tooth structure to measure the heat directed from the laser to the tooth. The zirconia blocks used were 1.5 mm thick to resemble the thickness of a standard zirconia crown. However, when the CO2 laser will be tested on zirconia crowns, modifications may include a higher energy pattern, longer laser time, or other laser settings to successfully remove the zirconia crown from dentin.
Within the limitations of this study, the 9.3µm CO2 laser effectively separated the zirconia restoration cemented with RelyXTM Luting Plus from dentin. RelyXTM Unicem 2 provided significantly stronger SBS than RelyXTM Luting Plus.
Conflict of Interest
This study was sponsored in part by Convergent Dental.
References
-
Dean JA, Donly KJ (2015) Restorative Dentistry. In McDonald and Avery’s Dentistry for the Child and Adolescent, Chapter 11. Elsevier pp: 185-205.
-
Nakamura K, Katsuda Y, Ankyu S, Harada A, Tenkumo T, et al. (2015) Cutting efficiency of diamond burs operated with electric high-speed dental handpiece on zirconia. Eur J Oral Sci 123(5): 375-380.
-
Cranska JP (2013) Removing All-Ceramic Restorations with Lasers. Dentistry Today.
-
Verma SK, Maheshwari S, Singh RK, Chaudhari PK (2012) Laser in Dentistry: An Innovative Tool in Modern Dental Practice. Natl J of Maxillofac Surg 3(2): 124-132.
-
Badreddine AH, Couitt S, Donovan J, Cantor Balan R, Kerbage C, et al. (2021) Demineralization Inhibition by High-Speed Scanning of 9.3 µm CO2 Single Laser Pulses Over Enamel. Lasers Surg Med 53(5): 703-712.
-
Rechmann P, Charland DA, Rechmann BM, Le CQ, Featherstone JD (2013) In-vivo occlusal caries prevention by pulsed CO2-laser and fluoride varnish treatment-A clinical pilot study. Lasers Surg Med: 45(5): 302-310.
-
Rechmann P, Fried D, Le CQ, Nelson G, Rapozo Hilo M, et al. (2011) Caries inhibition in vital teeth using 9.6-μm CO2-laser irradiation. J Biomed Opt 16(7): 071405.
-
Rechmann P, Le CQ, Kinsel R, Kerbage C, Rechmann BMT (2020) In vitro CO2 9.3-μm short-pulsed laser caries prevention-effects of a newly developed laser irradiation pattern. Lasers Med Sci 35(4): 979-989.
-
Rechmann P, Buu NCH, Rechmann BMT, Finzen FC (2014) Laser all-ceramic crown removal-a laboratory proof-of- principle study-phase 2 crown debonding time. Lasers Surg Med 46(8): 636-643.
-
Abdullah AO, Muhammed FK, Yu H, Pollington S, Xudong S, et al. (2019) The impact of laser scanning on zirconia coating and shear bond strength using veneer ceramic material. Dent Mater J 38(3): 452-463.
-
Dede DÖ, Yenisey M, Rona N, Öngöz Dede F (2016) Effects of Laser Treatment on the Bond Strength of Differently Sintered Zirconia Ceramics. Photomed Laser Surg 34(7): 276-283.
-
Gamal AE, Medioni E, Rocca JP, Fornaini C, Brulat Bouchard N (2018) CO2 laser dentin surface treatment most effectively increased ceramic shear bond strength. Laser Ther 27(1): 48-54.
-
Kasraei S, Atefat M, Maryam, Safavi N, Mojtahedi M, et al. (2014) Effect of Surface Treatment with Carbon Dioxide (CO2) Laser on Bond Strength between Cement Resin and Zirconia. J of Lasers Med Sci 5(3): 115-120.
-
Paranhos MP, Burnett LH Jr, Magne P (2011) Effect Of Nd:YAG laser and CO2 laser treatment on the resin bond strength to zirconia ceramic. Quintessence Int 42(1): 79- 89.
-
Ural Ç, Külünk T, Külünk Ş, Kurt M (2010) The effect of laser treatment on bonding between zirconia ceramic surface and resin cement. Acta Odontol Scand 68(6): 354-359.
-
Blatz MB, Chiche G, Holst S, Sadan A (2007) Influence of Surface Treatment and Simulated Aging on Bonded Strengths of Luting Agents to Zirconia. Quintessence Int 38(9): 745-753.
-
Piwowarczyk A, Lauer HC, Sorensen JA (2005) The shear bond strength between luting cements and zirconia ceramics after two pre-treatments. Oper Dent 30(3): 382-388.
-
Marghalani HY (2012) Sorption and solubility characteristics of self-adhesive resin cements. Dent Mater 28(10): 187-198.
-
Müller JA, Rohr N, Fischer J (2017) Evaluation of ISO 4049: water sorption and water solubility of resin cements. Eur J Oral Sci 125(2): 141-150.
-
Sulaiman TA, Abdulmajeed AA, Altitinchi A, Ahmed SN, Donovan TE (2019) Physical Properties, Film Thickness, and Bond Strengths of Resin-Modified Glass Ionomer Cements According to Their Delivery Method. J Prosthodont 28(1): 85-90.
-
Goldberg DJ (1998) Erbium:YAG Laser Resurfacing: What Is Its Role? Aesthet Surg J 18(4): 255-260.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells