Minimally Invasive Management of the Edentulous Space in the Anterior Sector without Prosthetic Loading
Introduction: Osseointegration is nowadays considered highly predictable, so minimally invasive surgical approaches are sought in order to allow proper function and a good esthetic result. It is of great importance to determine whether the shape and surface of the implant is an important factor in conjunction with the surgical technique. Objective: To evaluate the use of tomographic surgical guidance for the placement of a V3 implant in edentulous space in the maxillary esthetic zone. Method: A 53-year-old male patient with a vestibularly collapsed edentulous area corresponding to the left upper lateral. The treatment used was the IN2GUIDE system and MIS V3 implant, with evaluation up to 90 days. Results: Bone loss at the level of the implant platform without receiving any type of load. Discussion: Bone and peri-implant soft tissue loss will be similar with any procedure.
Introduction
In oral implantology, osseointegration is nowadays considered highly predictable, so minimally invasive surgical approaches are sought in order not only to allow proper functioning and a good esthetic result, but also to obtain the greatest possible comfort for the patient and, for this purpose, there are several techniques for implant placement [1]. However, it has been reported that several factors are associated with implant placement failure in the anterior maxilla (esthetic). The highest implant failure rate has been due to low insertion torque, immediate or early loading placement, inexperienced surgeons, heavy smokers, type III and IV bone qualities, small bone volumes, shorter implant length, lack of primary implant stability, implants with cylindrical macrogeometry (without thread), implant insertion in recently extracted sockets and smaller implant diameter [2]. Therefore, in this study, the use of tomographic surgical guidance for the placement of a V3 implant will be evaluated.
Material and Methods
53-year-old male patient presented to the Westhill University Dental Clinic for rehabilitation of the edentulous area of the left upper lateral, which has been maintained with a provisional prosthesis for 3 years. Personal history denied. Pathological history referred gastritis with treatment of Omeprazole 20 mg, 1 tablet only in case of crisis. A 3D CBCT tomographic study was requested with OnDemand3DApp Software Version 1.0.0.1, as well as initial study models. These showed absence of the left upper lateral and vestibular collapse of this area (Figure 1).
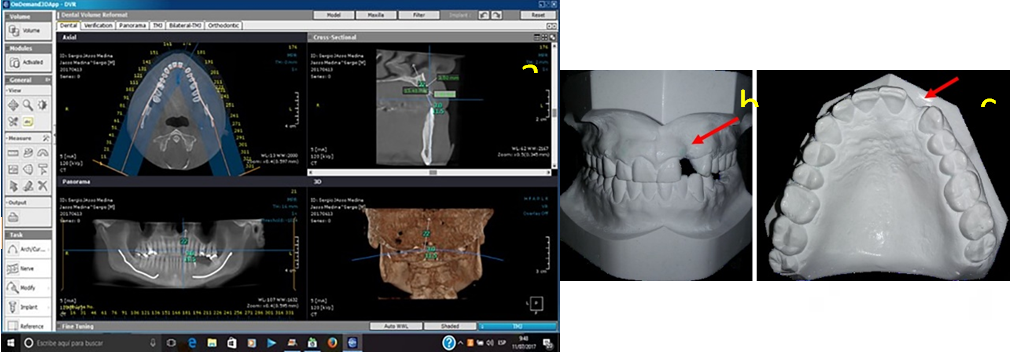
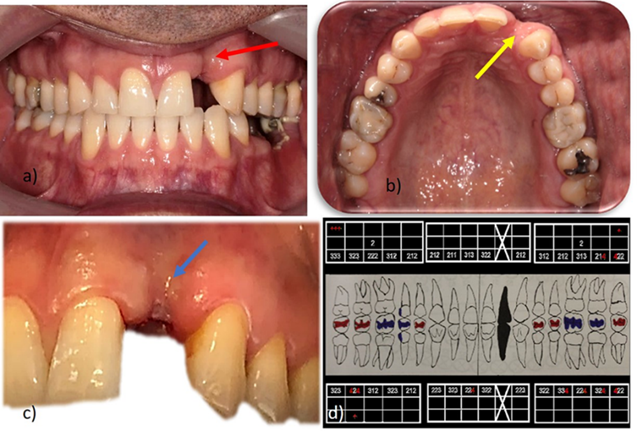
Clinically, healthy periodontal tissues were observed, slightly dry, flattened papillae, firm resilient consistency, sufficient inserted gingiva and absent in the area of the upper left lateral tooth. The color of the gingiva was pale pink with a thick gingival biotype; a collapse in the vestibular area of the upper left lateral tooth was also observed in the vestibular area of the same tooth (Figure 2).
To determine the bone defect in the area of the left lateral incisor, an initial three-dimensional tomographic analysis of the implant to be placed was performed to obtain the measurement of the crest, which was 3.86 mm; alveolar middle third 6.55 mm and length 12.95 mm. Subsequently, the mapping was carried out with the planning of the tomographic surgical guide obtaining a scan of the study model and later of the waxed model, to perform an overlay of these models in the OnDemand3DApp software, with the virtual placement of the implant and the ring indicated for the type of implant diameter. In order to obtain greater certainty of the spaces between the apex of the implant and the roots of the teeth, both mesial and distal measurements of the adjacent teeth were taken, obtaining 3.73 mm distally and 3.40 mm mesially (Figure 3).
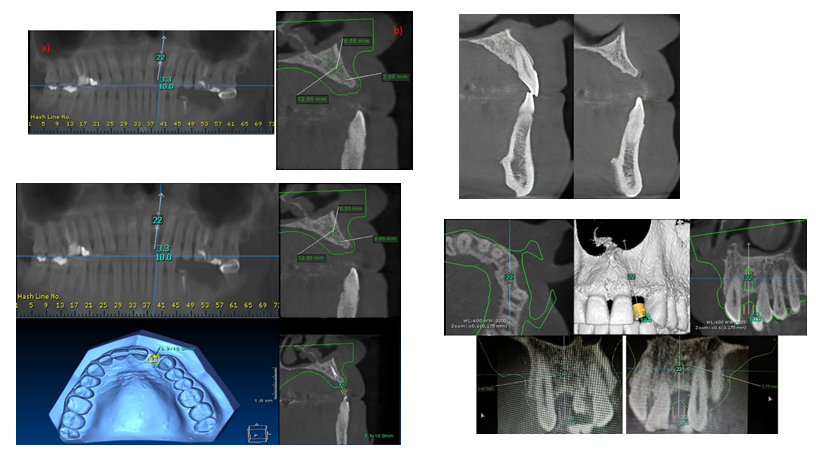
The OnDemand3DApp software was also used to measure the Hounsfield Units (HU) around the implant to know what type of bone we obtained around the implant, which as a result and according to Misch’s classification we obtained a type III bone. In order to obtain greater security of the guide and to ensure that it was in the desired conditions, a stability test was carried out to later corroborate again the position of the surgical guide ring with respect to the alveolar crests of the adjacent teeth, for which a periapical radiograph of parallel planes was taken with the help of the XCP.
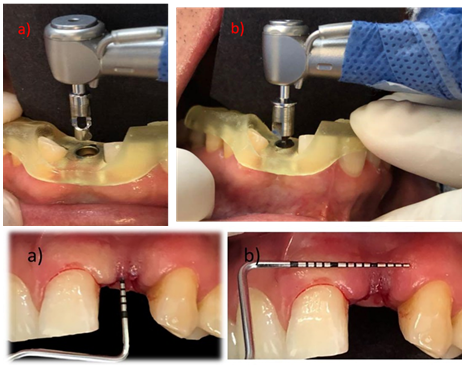
To start the surgical procedure, the drilling protocols of the In2Guide system were followed. We started with the 3.0 mm Mini Tissue Punch at 100 rpm to prepare the surgical bed until contacting the crestal bone and continued at 1500 rpm with the initial drill of the system. We continued with the restrictors, starting with M 2.0, continuing with M 2.8 and finishing according to the protocol with R 3.0, which will be stabilized inside the guide ring to avoid micro displacements inside. This same bur was manipulated with entry and exit movements at 800 RPM with continuous irrigation. Once the drilling was finished and prior to implant placement, we proceeded to verify the length with a periodontal probe, in order to obtain the measurement of our connective tissue, in a trapezoidal shape with a length of 5 mm and a thickness of 6 mm. The insertion of the V3 MIS implant was performed manually with the special implant transporter, where the torque meter (MIS) was used until reaching 40 N and it was decided to place the cover screw. At the end of the procedure a periapical radiograph was taken to validate the placement of the implant at the level of the alveolar ridge and to observe the distance between the roots of the teeth (Figure 4).
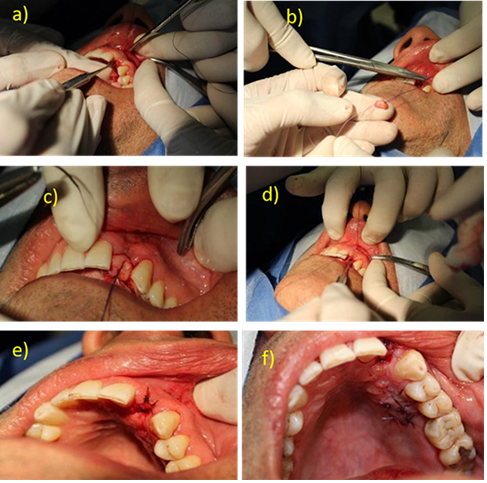
The area of the greater palatal nerve was reinforced and a horizontal incision was made with a scalpel blade #15C starting from mesial of the first molar to mesial of the first premolar; then internal cuts were made detaching the connective tissue of the epithelium. Once detached, vertical incisions were made to remove it and it was placed in a sterile gauze moistened with physiological solution to moisten it and remove the adipose tissue. The receptor bed was prepared, for which an envelope-shaped detachment of the epithelium was previously performed in the vestibular area in the mucoperiosteal type (onlay technique) with the help of the Hu-Friedy P20. Subsequently, the PGA 3-0 suture was placed in order to perform the knotting and transport of the connective tissue to the recipient site with a traction technique; the first intention closure of the donor site was performed with PGA 3-0 suture with tension stitches, thus achieving that the edges of the tissue were adequately faced.
No plaque was placed or made in order to obtain hemostasis and protection of the wound, since at the end of the knotting the correct closure was observed, so the patient was only given indications of postoperative care and oral hygiene, which consisted of using Chlorhexidine 0.12% in gel applied in the area twice a day for 15 days (Figure 5).
Results
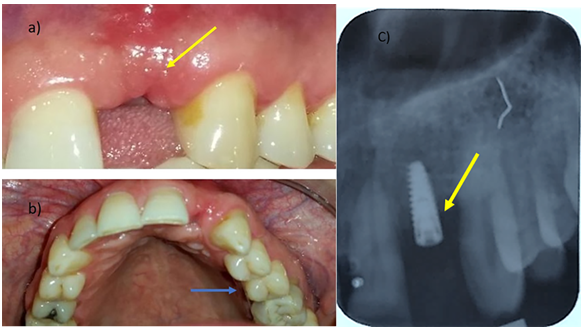
After 3 months of the atraumatic procedure and control of the scarring process, both of soft and hard tissues, we observed bone loss at the level of the alveolar ridge without the implant having received prosthetic load and could alter the osseointegration. Bone loss was inevitable at crestal level, an area where the manufacturer mentioned that bone tissue would be gained or at least not lost. In the case of the soft tissues, considerable repair and increase in keratinized gingiva was found, which helped to establish an adequate emergence profile at the time of prosthetic rehabilitation (Figure 6).
Discussion
Successful single implant placement in the esthetic zone, mainly in the maxillary zone comprises four areas: [1] peri-implant augmentation surgery, [2] implant placement accuracy (angulation >10° and labially positioned), [3] peri-implant soft tissue management, and [4] the quality of the prosthetic restoration [3, 4]. There should also be sufficient space between implant and tooth (>1 mm) to allow reconstruction or preservation of the interdental papilla, otherwise there will be insufficient blood supply, which would cause loss of this tissue [3, 4].
Some treatments usually require only adequate implant placement and minimal soft tissue manipulation in the second stage of surgery. Severe situations may require additional hard and soft tissue surgical procedures before, during or after implant placement [5].
In our study, in order to find these characteristics, it was decided to perform a technique that would allow us to establish the mentioned parameters [4], using a computerized surgical guide to measure the required spaces and obtain the expected esthetic results. During the process of the surgical guide, the protocols established by the different authors mentioned in this work, as well as some other authors, were established to estimate the correct depth of the implant. The thickness of the mucosa was decided before the insertion of the implant using a periodontal probe with a calibration of 1 mm and the measured thickness was added to the length of the implant as reported by D’Souza [6].
On the other hand, the flapless technique used in this work was used to reduce the resorption of peri-implant tissues, as established by the advantages of performing an atraumatic surgical technique, which has been mentioned by several authors who have approved protocols to reduce or compensate crestal resorption, including the use of the flapless technique (minimally invasive implant surgery) and subcrestal implant placement [3], however, in our study we obtained considerable bone resorption in the area where the authors mention that following these protocols would not result in loss of peri-implant tissues [7]. This makes us think that even when using the Flapless technique with computerized surgical guidance as an alternative, better results are not always obtained in comparison to conventional surgery, according to what was observed in this work, Carr BR demonstrated in his study that flapless implant placement is associated with a higher failure rate and that early failures will occur when a resident performs the flapless technique due to lack of skill and experience along with more careful case selection [8]. Since the loss of peri-implant tissues can be similar when using any procedure. Something similar could be observed in the study performed by Voulgarakis [4], where guided surgery without 3D navigation was used and reported an average marginal bone loss of 1.12 mm after an observation period of 1 year and 0.89 mm after an observation period of 2 years; during this study the bone loss observed radiographically is approximately 1.5 to 2 mm in a period of 90 days. For his part, Mora recommends that the flapless implant placement technique should continue to be evaluated for a longer period of time to observe the stability of the soft and hard tissues after loading on the implant together with studies with a larger sample size to confirm the results [9]. In contrast to what Collins and Altinci report in their studies, there are no disadvantages to place implants with platform switch prosthetic attachment, using a flapless surgical technique in relation to the preservation of the peri- implant tissues [10, 11]; although unfortunately there is not enough literature where we can corroborate the benefits that we can have when using this type of attachment. It is worth mentioning that we consider that it is of utmost importance to acquire a wide knowledge of the different software and systems that exist for the development of this type of surgical technique, as well as to be in constant communication with the designer of the guide and to have more scientific evidence.
In the case of the implant used in this study, the manufacturer mentions the benefits obtained according to the macrogeometry of the implant, where the desired effects were not obtained, even when following the manufacturer’s standards and protocols [2]. This is clearly seen in the results obtained in the present study, since in spite of having performed a minimally invasive procedure and with the help of guided surgery, the obtaining or integration of bone tissue in the platform area was not as expected.
References
-
Chiapasco M, Casentini P, Zaniboni M, Corsi E, Anello T (2012) Titanium-zirconium alloy narrow-diameter implants (Straumann Roxolid) for the rehabilitation of horizontally deficient edentulous ridges; Prospective study on 18 consecutive patients. Clin Oral Implants Res 23(10): 1136-1141.
-
Medvedev A, Molotnikov A, Lapovok R, Zeller R, Berner S, et al. (2016) Microstructure and mechanical propierties of Ti-15Zr alloy used as dental implant material. J Mech Behav Biomed Mater 62: 384-398.
-
Gamborena I, Lee J, Fiorini T, Susin C. Effect of Platform Shift / Switch and Concave Abutments on Crestal Bone Levels and Mucosal Profile following Flap and Flapless. Clin Implant Dent Relat Res 17(5): 908-916.
-
Voulgarakis A, Strub JR, Att W (2014) Outcomes of implants placed with three different flapless surgical procedures: A systematic review. Int J Oral Maxillofac Surg 43(4): 476-486.
-
Palacci P (2004) Aesthetic treatment of the anterior maxilla: Soft and hard tissue considerations. Oral and Maxillofacial Surgery Clinics of North America 16(1): 127-137.
-
D Souza KM, Aras MA (2012) Types of Implant Surgical Guides in Dentistry: A Review. J Oral Implantol 38(5): 643-652.
-
Laleman I, Bernard L, Vercruyssen M, Jacobs R, Bornstein M, et al. (2017) Guided Implant Surgery in the Edentulous Maxilla: A Systematic Review. Int J Oral Maxillofac Implants 31: 103-117.
-
Carr BR, Rekawek P, Gulko JA, Coburn JF, Boggess WJ, et al. (2022) Does implant placement using a minimally invasive technique increase early failures among trainees at an academic center?. Oral Maxillofac Surg.
-
Mora MA, Chenin DL, Arce RM (2014) Software tools and surgical guides in dental-implant-guided surgery. Dental Clinics of North America 58(3): 597-626.
-
Collins J, Sued M, Rodriguez I, Berg R, Coelho P (2013) Evaluation of Human Peri-implant Soft Tissues Around Alumina-Blasted/Acid-Etched Standard and Platform- Switched Abutments. Int J Periodontics Restorative Dent 33(2): 51-57.
-
Altinci P, Can G, Gunes O, Ozturk C, Eren H (2016) Stability and Marginal Bone Level Changes of SLActive Titanium-Zirconium Implants Placed with Flapless Surgery: A Prospective Pilot Study. Clin Implant Dent Relat Res 18(6): 1193-1199.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells