Prevalence of Ponticulus Posticus (PP): A Cross-Sectional Study Using Digitized Lateral Cephalograms
Background: Ponticulus Posticus (PP) is described as an anomalous malformed bony bridge between the posterior portion of the superior articular process and the posterolateral portion of the superior margin of the posterior arch of the atlas. Many terms, including foramen sagittale, Kimmerle anomaly, foramen arcuale, and arcuate foramen, have been used in the literature to describe this anomaly. Presence of this anomaly can result in occlusion of vertebral artery which can lead to various head and neck symptoms. Objectives: The purpose of this study was to investigate the prevalence of PP in digitized lateral cephalograms. Methodology: The presence and types of PP were assessed in 212 digitized cephalograms. Presence of PP in 64 digitized lateral cephalograms was confirmed after using Adobe Photoshop® (for image enhancement). Results: PP was found in 30.18% (64 out of 212) subjects out of which 31.45% (39 out of 124) were females and 28.41% (25 out of 88) were males in an age group of 8 to 44 years (mean age = 26years, SD+/- 18years). Significant difference in number of PP cases in males and females was tested by Chi square test (p-value=0.003). Out of 64 patients, bilateral complete were 5 (7.81%), bilateral partial 40 (62.50%), unilateral complete 6 (9.37%), unilateral partial 12 (18.75%) and complete partial 1 (1.56%). Conclusion: Lateral cephalogram can act as a baseline screening tool for detection of PP. Detecting a PP in lateral cephalogram has an importance as it can prove beneficial for the diagnosis of head and neck symptoms and can be sent for further investigations. Also, digitized Lateral cephalograms had an edge over the conventional lateral cephalograms in detecting PP.
Introduction
Ponticulus Posticus (PP) is a variation seen in the cervical atlas vertebra. Ponticulus Posticus, a Latin term that means “the little posterior bridge,” is described as an anomalous malformed bony bridge between the posterior portion of the superior articular process and the posterolateral portion of the superior margin of the posterior arch of the atlas [1]. During ossification of the vertebra, frequently bony spurs arise from the anterior and posterior margins of the groove for the vertebral artery. These are sometimes referred to as ponticles, and they occasionally convert the groove into a foramen [2]. A variety of terms have been used for this anomaly, including Ponticulus Posticus, canalis vertebralis, foramen sagittale, foramen arcuale, foramen atlantoideum posterior, foramen retroarticulare superior, Kimmerle’s anomaly, retroarticular canal, retroarticular vertebral artery ring and retrocondylar vertebral artery.
PP has been evaluated using dry skulls and various radiographic techniques like lateral cephalograms, computed tomography (CT) and cone beam computed tomography (CBCT). The paper aims (1) to investigate the prevalence of PP in digitised lateral cephalograms; (2) to evaluate the usefulness of the digitised lateral cephalogram in detecting PP; (3) to categorize the types of the detected cases and (4) to present a review of literature.
Materials and Methods
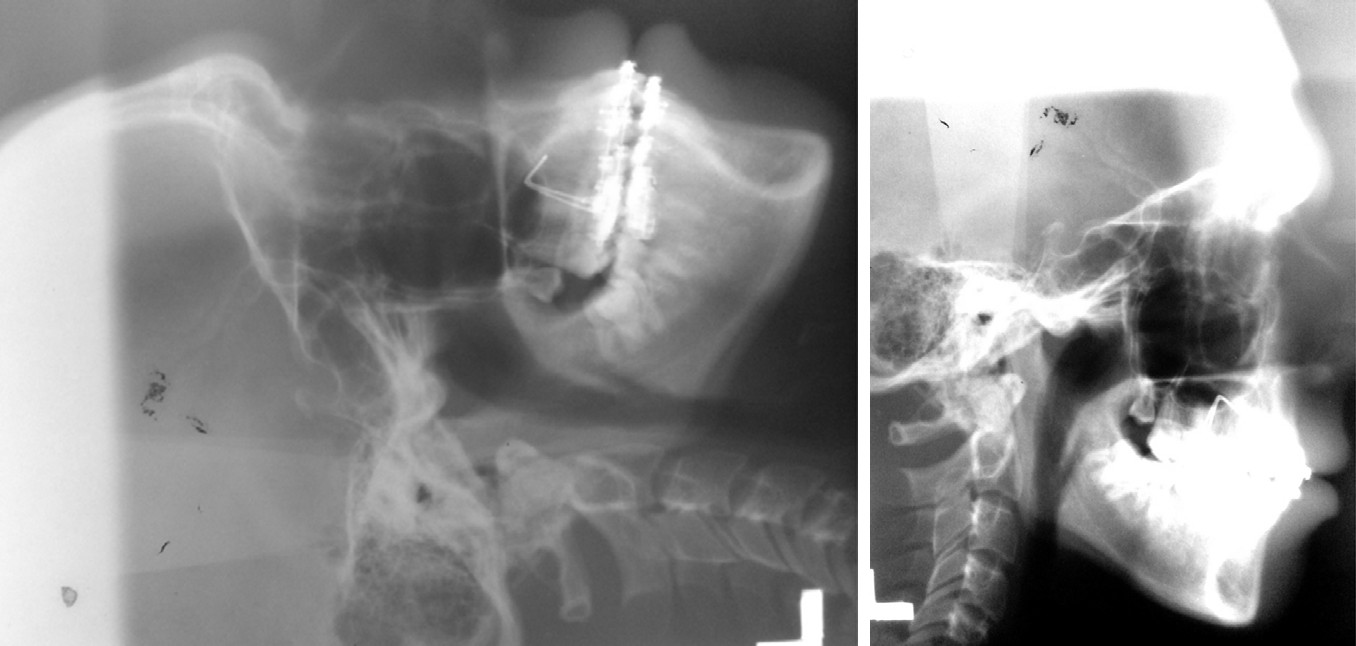
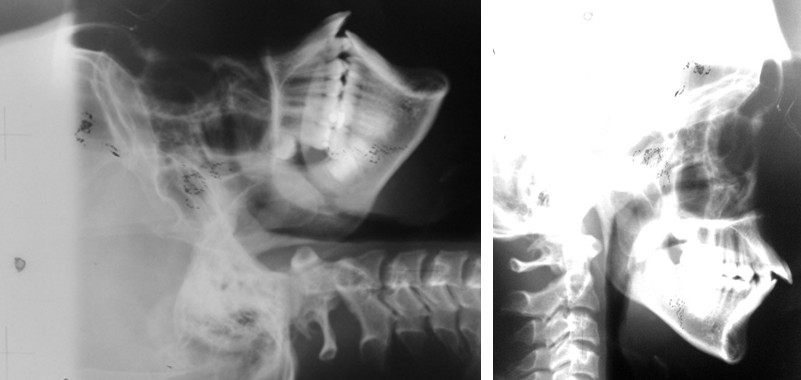
Conventional Lateral Cephalograms (Carestream® E speed TMX 8x10 film) of 212 subjects out of which 88 were males and 124 females; were digitised by using Canon PowerShot SX120 IS® (exposure time: 1/30sec; ISO speed: 200; F-stop: f/3.5) mounted on tripod stand with a distance of 60cm from the GDP SLIM XRAY viewer - LED®. Lateral cephalograms with poor visualization of the posterior arch of the atlas due to overlapping of the mastoid process or the occiput and with congenital anomalies or other syndromic conditions of craniofacial region were excluded [1]. Presence and type of PP in digitised lateral cephalograms was confirmed after using Adobe Photoshop® (for image enhancement) and were classified as: (1) Bilateral complete – complete ossification on both sides; (2) Bilateral partial – incomplete ossification on both sides; (3) Unilateral complete – complete ossification on one side, absent on other side; (4) Unilateral partial – incomplete ossification on one side, absent on other side; (5) Complete partial – complete on one side, partial on other side.
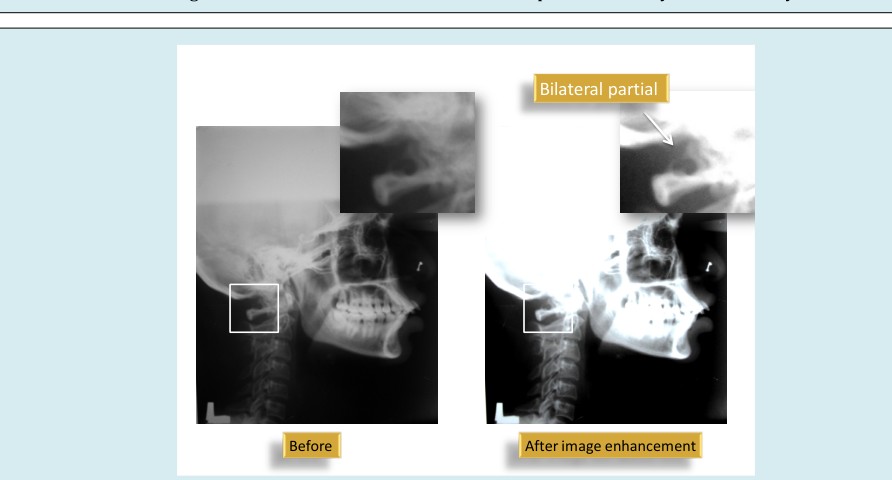
Before
The literature was searched using the PubMed, Cochrane and Google Scholar database till December 2014. The keywords “Ponticulus Posticus,” “posticus ponticus,” “foramen arcuate,” “foramen arcuale,” “foramen sagittale,” “foramen atlantoideum posterior,” “Kimmerle’s anomaly,” “foramen retroarticulare superior,” “canalis vertebralis,” “retroarticular vertebral artery ring,” “retroarticular canal” and “retrocondylar vertebral artery” were used for search.
Evaluation of Images
A complete PP is one continuous bridge that extends from the posterior aspect of the lateral mass to the anterior aspect of the posterior tubercle. A partial PP is one that does not extend fully from the posterior lateral mass to the posterior tubercle. A PP can possibly be identified incorrectly as a broad dorsal arch of the atlas. A normal posterior arch of the atlas thins out laterally and does not curve up cranially, whereas a PP broadens laterally and extends cranially [3]. Two authors examined each image for the presence of PP in any of its forms as explained above. Each image was assessed by two authors, who noted whether any type of PP (i.e., partial or complete) was present. There were some cases where the authors disagreed about the presence of partial PP, and only images that both authors agreed upon with regard to the presence or absence of PP in any of its forms (i.e. complete or partial) were included in the calculation of the prevalence. The Figure 1 through 4 show the different types of PP before and after the image enhancement, and how the enhanced images were better in diagnosing the type of PP.
$$ \mathrm {型 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 Unilateral complete $$
\mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2}
$$
Results
PP was found in 30.18% (64 out of 212) subjects out of which 31.45% (39 out of 124) were females and 28.41% (25 out of 88) were males in an age group of 8 to 44 years (mean age = 26years, SD+/- 18years). Statistical analysis was performed by entering the data in Microsoft office 2007® using chi square test with p-value < 0.05 considered as significant (Graph 1, Table 1).
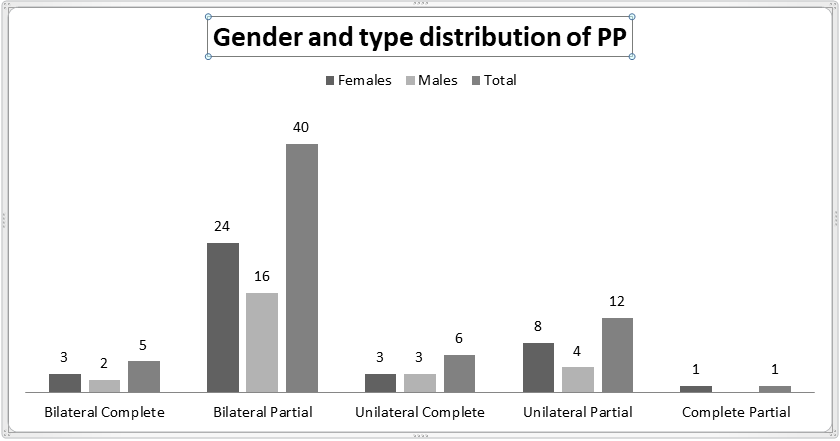
Graph 1: Gender and types distribution of PP showing maximum number of Bilateral Partial PP present in women.
| Total (64) | Females (39) | Males (25) | |
|---|---|---|---|
| Bilateral Complete | 5 (7.81%) | 3 (7.69%) | 2 (8%) |
| Bilateral Partial | 40 (62.50%) | 24 (61.53%) | 16 (64%) |
| Unilateral Complete | 6 (9.37%) | 3 (7.69%) | 3 (12%) |
| Unilateral Partial | 12 (18.75%) | 8 (20.51%) | 4 (16%) |
| Complete Partial | 1 (1.56%) | 1 (2.56%) |
Table 1: Using Chi square test the difference among types of PP was found to be non-significant (p value = 0.89; p value < 0.05 w
Discussion
Studies have been done on the Ponticulus Posticus since 1881 [4]. In the western population, prevalence has been reported to range from 5.1 to 37.8% [1]. (present study = 30.18%). Varying incidences of posterior ponticuli and their study methods are shown in Table 2. Though considered as a simple anatomic variant on the cervical atlas vertebrae, it is an important, common anomaly. Paraskevas, et al. [5] had put forward a possibility that the calcification of the bony bridge progresses over time from an incomplete bony arch to complete ossification, the present study also found 3 unilateral partial PP in children under 10 years of age. But in contrast Shilling J, et al. [6] who found complete ossification in children under 10 years of age; and Lamberty & Zivanovic [7], who observed the Ponticulus Posticus cartilage in fetuses and children suggesting that while ossification is most likely a gradual process, its initiation is least likely to be age related. Various studies till date have been reported associating PP with various conditions, including vertebrobasilar insufficiency, headache, cervical pain syndrome, migraine without aura, acute hearing loss, and chronic tension-type headaches [1, 7, 8, 9, 10]. The PP is a bony arch on the cervical atlas vertebrae that gets converted from a groove on the upper surface of the arcus posterior atlantis to the foramen called arcuate foramen [3]. This foramen chiefly contains important anatomic structures, like the vertebral artery and the suboccipital nerve [5, 7, 10].
Lamberty and Zivanovic [7] have shown that PP is closely attached to the atlantooccipital membrane, and it is identified that the membrane is connected to the dura. When the head moves, the neurodynamic process may lead to the conditions enlisted (vertebrobasilar insufficiency, headache etc) because of traction on the dura, and can result in pain. The authors define PP as the causative factor in headaches, vertigo, Barré-Lieou syndrome, eye pain, and photophobia because these lead to ischemia of the vertebrobasilar circulation through compression of the vertebral artery which was also supported by Barsukov et al. [3, 11]. Surgical excision of PP relieved the symptoms [12, 13, 14]. Cushing, et al. [15] studied the children with vertebrobasilar artery stroke and suggested a contributory relationship between PP and dissection of the vertebral artery. On the other hand, Wight, et al. [13] reported a correlation between the presence of PP and migraine without aura, linking migraine and cervicogenic headache to the upper cervical spine. The relationship between PP and acute hearing loss could be based on a functional disturbance in the area of cervico- occipital junction. [13, 16] Schilling J, et al. [6] suggested that PP is an anatomic condition with a protective function though any literature couldn’t be found supporting the same.
PP has been identified as an important anomaly since the lateral mass screws began being used for the treatment of atlantoaxial instability [1, 16, 17, 18, 19, 20, 21, 22, 23, 24].
| Authors(Year) | Sample size | Prevalance (%) | Method of study |
|---|---|---|---|
| Loth-Niemerycz (1916) | N.A | 7.4 | Dry bone specimens |
| Selby, et al. (1955) [25] | 306 | 27.12 | Plain radiographs |
| Pyo & Lowman (1959) [26] | 300 | 12.67 | Plain radiographs |
| Kendrick & Biggs (1963) [27] | 353 | 15.8 | Plain radiographs |
| Romanus & Tovi (1964) [28] | 105 | 14.29 | Dry bone specimens |
| Lamberty & Zivanovic (1973) [7] | 60 | 36.67 | Dry bone specimens |
| Lamberty & Zivanovic (1973) [7] | 990 | 13.64 | Plain radiographs |
| Saunders & Popovich (1978) [29] | 592 | 29.22 | Plain radiographs |
| Malhotra, et al. (1979) [30] | NA | 5.14 | Dry bone specimens |
| Takaaki, et al. (1979) [31] | 307 | 4.89 | Plain radiographs |
| Farman, et al. (1979) [24] | 220 | 26.82 | Plain radiographs |
| Dugdale (1981) [32] | 316 | 15.51 | Plain radiographs |
| Taitz & Nathan (1986) [33] | 672 | 7.8 | Plain radiographs |
| Sweat & Crowe (1987) [4] | 1000 | 13 | Plain radiographs |
| Ruprecht, et al. (1988) [34] | 419 | 32.94 | Plain radiographs |
| Stubbs (1992) [35] | 1000 | 18.7 | Plain radiographs |
| Prescher (1997) [36] | 200 | 11 | Plain radiographs |
| Mitchell (1998) [37] | 1354 | 9.8 | Plain radiographs |
| Wight (1999) [13] | 895 | 18 | Plain radiographs |
| Cederberg (2000) [38] | 255 | 11 | Plain radiographs |
| Hasan (2001) [30] | 350 | 6.57 | Dry bone specimens |
| Manjunath (2001) [39] | 60 | 11.7 | Dry bone specimens |
| Unur (2004) [40] | 351 | 7.2 | Plain radiographs (lat spine) |
| Kavakli (2004) [23] | 86 | 22.09 | Dry bone specimens |
| Young, et al. (2005) [16] | 464 | 15.5 | Plain radiographs |
| Young, et al. (2005) [16] | 20 | 15 | Dry bone specimens |
| Paraskevas, et al. (2005) [5] | 176 | 34.66 | Dry bone specimens |
| Cakmak (2005) [41] | 416 | 13.46 | Plain radiographs |
| Cakmak (2005) [41] | 60 | 15 | Dr bone specimens |
| Krishnamurthy, et al. (2007) [42] | 1044 | 13.79 | Dry bone specimens |
| Kim, et al. (2007) [17] | 312 | 14.1 | Plain radiographs |
| Kim, et al. (2007) [17] | 225 | 25.78 | CT scan |
| Kobayashi (2008) [21] | 50 | 10 | Dry bone specimens |
| Gupta, et al. (2008) [22] | 55 | 10.91 | Dry bone specimens |
| Hong, et al. (2008) [43] | 1013 | 15.6 | CT |
| Sharma, et al. (2009) [1] | 858 | 4.3 | Plain radiographs |
| Cho (2009) [18] | 200 | 15.5 | CT |
| Karau, et al. (2010) [44] | 102 | 52.94 | Dry bone specimens |
| Yeom, et al. (2012) [19] | 52 | 17.31 | CT |
| Chitroda, et al. (2013) [8] | 500 | 68.4 | Plain radiographs |
| Bayrakdar, et al. (2013) [3] | 730 | 17.4 | CBCT |
| Giest, et al. (2014) [45] | 576 | 52.9 | CBCT |
| Sabir, et al. (2014) [46] | 200 | 42 (migraine) | CBCT |
| 19 (healthy) | |||
| Present Study | 212 | 30.18 | Digitised plain radiographs |
Table 2: Prevalence of PP in the literature.
A broad posterior arch of the atlas offers the best way for applying this procedure, but PP has the possibility of being incorrectly identified as the broad posterior arch. Inaccurate placement of the screw can result in injury to the vertebral artery and can lead to stroke and death by thrombo- embolism, or arterial dissection [1, 16, 17, 18, 20]. As the present study was cross sectional, any special patient groups i.e.
Before
with various signs and symptoms could not be included. For confirmation of presence and types of PP, higher imaging modalities like CBCT are required. However, considering the importance of this anomaly, digitized lateral cephalograms can be considered as a cost effective and easily available screening tool (Figures 2-4).
$$ \mathrm {型 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 形 Bilateral partial $$
\mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2}
$$

$$ - \mathrm {I} $$ $$ \mathrm {型} = \mathrm {型} $$
$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$

$$ - \frac {1}{2} x - 1 > 3 - \frac {3}{2} x $$
Lateral cephalogram can act as a baseline screening tool for detection of PP. Detecting a PP in lateral cephalogram has an importance as it can prove beneficial for the diagnosis of head and neck symptoms and can be sent for further investigations. Also, digitised Lateral cephalograms had an edge over the conventional lateral cephalograms in detecting PP.
1. Sharma V, Chaudhary D, Mitra R (2010) Prevalence of Ponticulus Posticus in Indian Orthodontic Patients. Dentomaxillofac Radiol 39(5): 277-283.
2. Williams A, Newell, RLM (2008) Gray’s Anatomy. 40th (Edn.), In: Standring S (Eds.), Churchill Livingston: Elsevier.
3. Bayrakdar IS, Miloglu O, Oguzhan A, Gumussoy I, Durna D, et al. (2014) Cone Beam Com Puted Tomography Imaging of Posticus Ponticulus: Prevelance, Characteristics and Review of Literature. Oral Surg Oral Med Oral Pathol Oral Radiol 118(6): 210-219.
4. Sweat RW, Crowe HS (1987) The Ponticulus Posticus. Today’s Chiropr 16: 95-97.
5. Paraskevas G, Papaziogas B, Tsonidis C, Kapetanos G (2005) Gross Morphology of the Bridges over the Vertebral Artery Groove on the Atlas. Surg Radiol Anat 27(2): 129-136.
6. Schilling J, Schilling A, Suazo GI (2010) Ponticulus Posticus on the Posterior Arch of Atlas: Prevalence Analysis in Asymptomatic Patients. Int J Morphol 28(1): 317-322.
7. Lamberty BG, Zivanovic S (1973) The Retro-Articular Vertebral Artery Ring of the Atlas and Its Significance. Acta Anat (Basel) 85(1): 113-122.
8. Chitroda PK, Katti G, Baba IA, Najmudin M, Ghali SR, et al. (2013) Ponticulus Posticus on the Posterior Arch of Atlas, Prevalence Analysis in Symptomatic and Asymptomatic Patients of Gulbarga Population. J Clin Diagn Res 7(12): 3044-3047.
9. Bernal SM, HörmannK, Weh L (1990) Sudden Hearing Loss and the Craniocervical Junction. Acta Otorrinolaringol Esp 41: 93-95.
10. Li S, Li W, Sun J (1995) Operative Treatment for Cervical Vertigo Caused by Foramen Arcuale. Zhonghua Wai Ke Za Zhi 33(3): 137-139.
11. Barsukov SF, Grishin GP (1991) The Vertebrobasilar Blood Circulation of the Brain in the Presence of Kimmerle’s Anomaly. Voen Med Zh 6:42-45.
12. Koutsouraki E, Avdelidi E, Michmizos D, Kapsali SE, Costa V, et al. (2010) Kimmerle’s Anomaly As A Possible Causative Factor Of Chronic Tension-Type Headaches And Neurosensory Hearing Loss: Case Report And Literature Review. Int J Neurosci 120(3): 236-239.
13. Wight S, Osborne N, Breen AC (1999) Incidence of Ponticulus Posterior of the Atlas in Migraine and Cervicogenic Headache. J Manipulative Physiol Ther 22(1): 15-20.
14. Travan L, Saccheri P, Sabbadini G, Crivellato E (2011) Bilateral Arcuate Foramen Associated with Partial Defect of the Posterior Arch of the Atlas in A Medieval Skeleton: Case Report and Review of the Literature. Looking Backward to Go Forward. Surg Radiol Anat 33(66): 495-
500.
15. Cushing KE, Ramesh V, Gardner Medwin D, Todd NV, Gholkar A, et al. (2001) Tethering of the Vertebral Artery in the Congenital Arcuate Foramen of the Atlas Vertebra: A Possible Cause of Vertebral Artery Dissection in Children. Dev Med Child Neurol 43(7): 491-496.
16. Young JP, Young PH, Ackermann MJ, Anderson PA, Riew KD (2005) The Ponticulus Posticus: Implications for Screw Insertion into the First Cervical Lateral Mass. J Bone Joint Surg 87(11): 2495-2498.
17. Kim KH, Park KW, Manh TH, Yeom JS, Chang BS, et al. (2007) Prevalence and Morphologic Features of Ponticulus Posticus in Koreans: Analysis of 312 Radiographs and 225 Three-Dimensional CT Scans. Asian Spine J 1(1): 27-31.
18. Cho YJ (2009) Radiological Analysis of Ponticulus Posticus in Koreans. Yonsei Med J 50(1): 45-49.
19. Yeom JS, Kafle D, Nguyen NQ, Noh W, Park KW, et al. (2012) Routine Insertion of the Lateral Mass Screw Via the Posterior Arch for C1 Fixation: Feasibility and Related Complications. Spine J 12(6): 476-483.
20. Goel A (2013) Screws, Facets, and Atlantoaxial Instability. World Neurosurg 80(5): 514-515.
21. Kobayashi Y, Kikuchi S, Konno S, Sekiguchi M (2008) Insertion of Lateral Mass Screw of the Atlas Via the Posterior Arch: Anatomical Study of Screw Insertion Using Dry Bone Samples of the Atlas from Japanese Cadavers. J Orthop Sci 13(5): 452-455.
22. Gupta T (2008) Quantitative Anatomy of Vertebral Artery Groove on the Posterior Arch of Atlas in Relation to Spinal Surgical Procedures. Surg Radiol Anat 30(3): 239-242.
23. Kavakli A, Aydinlioglu A, Yesilyurt H, Kus I, Diyarbakirli S, et al. (2004) Variants and Deformitiesof Atlas Vertebrae in Eastern Anatolian People. Saudi Med J 25(3): 322-325.
24. Farman AG, Nortje CJ, Joubert JJ (1979) Radiographic Profile of the First Cervical Vertebra. J Anat 128(3): 595- 600.
25. Selby S, Garn SM, Kanareff V (1955) The Incidence and Familial Nature of A Bony Bridge on the First Cervical Vertebra. Am J Phys Anthropol 13(1): 129-141.
26. Pyo J, Lowman RM (1959) The Ponticulus Posticus of the First Cervical Vertebra. Radiology 72(6): 850-854.
27. Kendrick GS, Biggs NL (1963) Incidence of the Ponticulus
Posticus of the First Cervical Vertebra between Ages Six to Seventeen. Anat Rec 145: 449-453.
28. Romanus T, Tovi A (1964) A Variation of the Atlas, Roentgenologic Incidence of a Bridge over the Groove of the Atlas for the Vertebral Artery. Acta Radiol Diagn (Stockh) 2: 289-297.
29. Saunders SR, Popovich F (1978) A Family Study of Two Skeletal Variants: Atlas Bridging and Clinoid Bridging. Am J Phys Anthropol 49(2): 193-203.
30. Hasan M, Shukla S, Siddiqui MS, Singh D (2001) Posterolateral Tunnels and Ponticuli in Human Atlas Vertebrae. J Anat 199(3): 339-343.
31. Takaaki M, Masanori O, Hidenori U, Eikazu H, Seisuke T, et al. (1979) Ponticulus Ponticus: Its Clinical Significance. Acta Medica Kinki Univ 4: 427-430.
32. Dugdale LM (1981) The Ponticulus Posterior of the Atlas. Australas Radiol 25(3): 237-238.
33. Taitz C, Nathan H (1986) Some Observations on the Posterior and Lateral Bridge of the Atlas. Acta Anat (Basel) 127(3): 212-217.
34. Ruprecht A, Nashashibi I, Lambourne A (1988) Ponticles of the Atlas. Dentomaxillofac Radiol 17(1): 67-71.
35. Stubbs DM (1992) The Arcuate Foramen: Variability in Distribution Related to Race and Sex. Spine 17: 1502- 1504.
36. Prescher A (1997) The Craniocervical Junction in Man, the Osseous Variations, their Significance and Differential Diagnosis. Ann Anat 179(1): 1-19.
37. Mitchell J (1998) The Incidence and Dimensions of the Retroarticular Canal of the Atlas Vertebra. Acta Anat (Basel) 163(2): 113-120.
38. Cederberg RA, Benson BW, Nunn M, English JD (2000)
Arcuate Foramen: Prevalence by Age, Gender, and Degree of Calcification. Clin Orthod Res 3(3): 162-167.
39. Manjunath KY (2001) Posterior Bridging of the Atlas Vertebra in South Indians. Indian J Med Sci 55(9): 488- 490.
40. Unur E, Erdogan N, Ulger H, Ekinci N, Ozturk O (2004) Radiographic Incidence of Complete Arcuate Foramen in Turkish Population. Erciyes Med J 26(2): 50-54.
41. Cakmak O, Gurdal E, Ekinci G, Yildiz E, Cavdar S (2005) Arcuate Foramen and Its Clinical Significance. Saudi Med J 26(9): 1409-1413.
42. Krishnamurthy A, Nayak SR, Khan S, Prabhu LV, Ramanathan LA, et al. (2007) Arcuate Foramen of Atlas: Incidence, Phylogenetic and Clinical Significance. Rom J Morphol Embryol 48(3): 263-266.
43. Hong JT, Lee SW, Son BC, Sung JH, Yang SH, et al. (2008) Analysis of Anatomical Variations of Bone and Vascular Structures Around the Posterior Atlantal Arch Using Three-Dimensional Computed Tomography Angiography. J Neurosurg Spine 8(3): 230-236.
44. Karau PB, Ogengo JA, Hassanali J, Odula P (2010) Anatomy and Prevalence of Atlas Vertebrae Bridges in a Kenyan Population: An Osteological Study. Clin Anat 23(6): 649-653.
45. Geist JR, Geist SM, Lin LM (2014) A Cone Beam CT Investigation of Ponticulus Posticus and Lateralis in Children and Adolescents. Dentomaxillofac Radiol 43(5): 20130451.
46. Sabir H, Kumbhare S, Rout P (2014) Evaluation of Ponticulus Posticus on Digital Lateral Cephalograms and Cone Beam Computed Tomography in Patients with Migraine and Healthy Individuals: A Comparative Study. Oral Surg Oral Med Oral Pathol Oral Radiol 118(3): 348- 354.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells