Relationship between the Shape of the Dental Arch and the Presence of Traumatic Lesions on the Lateral Borders of the Tongue
The aim of this descriptive, prospective, cross-sectional study was to evaluate clinical signs, to relate the shape of the dental arches with the occurrence of lesions of traumatic origin on the lateral borders of the tongue, and then determine which form of dental arches is prevalent in relation to the development of lesions of traumatic origin on the borders of the tongue. Each of the forms of the dental arch described in the work, present a different way in which they relate to the tongue. The link between the hard structures (dental arches) and the voluminous soft mobile structure (tongue) lead us to suspect that each of the forms found, may develop a lesion of relative importance. Chronic trauma of the oral mucosa, is the result of the irritative and repeated mechanical action of an aggressive intraoral agent, in this case the teeth, acting individually or together, causing mechanical irritation. The risk factors that stimulate carcinogenesis, classically described in the literature, are tobacco and alcohol, but nowadays it is known that there are other emerging risks such as chronic mechanical irritation, caused by dental elements. Conclusion: It is apparent, through the patients studied, that there is a relationship between certain forms of arches and the development of lesions of traumatic origin on the border of the tongue.
Introduction
The tooth constitutes the unit of the dental system and the chewing apparatus. Teeth are made up of similar elements, which, varying in shape, volume and position, give rise to different groups. Aligning with the teeth of the maxilla itself, they come into contact on their proximal faces, follow a curvature of posterior concavity and form, with their support structures, an anatomical- physiological unit called the dental arch.
The different shapes of the dental arch are obtained from the conjunction of the supporting bone, the position of the teeth, parafunctional habits, diet, respiratory disorders, systemic diseases and basically from the balance between the intra and extraoral muscular forces. The centrifuges forces generated by the tongue and the centripetal ones coming from the perioral musculature.
The shape and size of the dental arches also has an undoubted influence on the location of the tongue on the floor of the mouth when it is at rest.
It is currently known that the contact of the tongue with the dental arches can generate injuries in the pressure areas. Trauma is a cofactor that affects the appearance of injuries in the tongue and surrounding tissues (Figure 1).
The Dental Arch: the following forms of dental arches are currently accepted in the literature, and can be summarized as follows:
- Ovoid: relative anterior curvature and posterior convergence. It is recorded in 85% of cases. The anterior and posterior sectors follow a segment of very regular circumference, with distal ends toward the midline. Attributed to individuals with a strong and voluminous bone constitution.
- Parabolic: Similar to a parabola. It has anterior curvature and slight divergence in the posterior sectors.
- Elliptical or round: similar to the ovoid but with exaggeration of the anterior curvature and slightly convergent posterior sectors.
- Hyperbolic: shaped like a hyperbola, with a flattened anterior curve and marked divergence in the posterior sectors.
- In V: more exaggerated. Angled anterior sector and divergent posterior segments
- U-shaped or square: anterior portion almost straight and posterior sectors parallel to each other. Attributed to individuals such as the Saxons.
![Figure 1: Different proposed forms of dental arches [1].](/fulltextimages/8928/fig_1.png)
The tongue is a mobile muscular eminence that occupies the floor of the oral cavity, and has an irregularly oval shape with a thick posterior extremity, and its tips is inclines forward.
The assessment of the size of the tongue is based on subjective criteria by observing the clinical discrepancy between its size and the size of the oral cavity [2]. The tongue reaches approximately its final size at the age of 18 years [3]. The average volume of the tongue in adults is larger in men than in women, 25.3 cm3 and 22.6 cm3, respectively [4]. There is a high correlation between the tongue and the lower arch and it is higher in the posterior part of the dental arch [5].
Relationship between the tongue and the dental arches: the lingual volume has a close relationship with both dental arches. That relationship is natural and is accentuated in the posterior third or lingual trunk, when the tongue is at rest [5]. The adaptive role that the tongue has, within the dental arches, is undeniable [6, 7]. The dimensions of the dental arches have an important role in determining the alignment of the teeth, stability of the arch shape and relief of crowding, and an irrefutable incidence in the location of the tongue.
In a situation of biomechanical balance, each dental arch is in a position to accept, dissipate and exert pressures that occur in the chewing act, without injuring neighboring structures. Chronic trauma of the oral mucosa (CTOM) is the result of the irritative and repeated mechanical action of an intraoral aggressor agent, in this case the teeth, acting individually or together, causing mechanical irritation [8].
CTOM can generate lesions in healthy mucosa or intensify previous oral pathologies, for example, indentations on the edge of the tongue. Epidemiological and laboratory studies describe a possible causal relationship betwen CTOM and oral cancer [9].
Carcinogenesis: the risk factors that stimulate carcinogenesis, classically described in the literature, are tobacco and alcohol, nowadays it is known that there are other emerging risks such as chronic mechanical irritation (CMI) caused by dental elements [10]. CMI of the squamous epithelium of the oral mucosa can promote dysplasia and carcinogenesis, independent of other factors. This effect can occur on the oral mucosa more easily, if it is previously initiated by some other carcinogen, as observed in patients with potentially malignant disorders [11].
The hardness of the traumatizing agent and the time of exposure to CMI have a direct influence on an increased risk of developing oral cancer [12].
Carcinogenesis induced by CMI of the edges of the tongue shows an increase in frequency, a higher degree of malignancy and a decrease in the latency period, this suggests that CTOM may play a role as a promoter and progressor of oral neoplasms [13]. It can also act as a facilitator of epithelial invasion by HPV, whose relationship with carcinogenesis is known [7, 14].
Oxidative and nitrative damage to DNA is carried out through chronic inflammation, which is related to trauma and carcinogenesis [15].
During the last 100 years it has been recognized that most tumors are associated with inflammatory cells. The association was established by Virchow in 1863, who generated the hypothesis that cancer arises in places of inflammation, and proposed the theory of chronic irritation to explain the origin of some malignant neoplasms [16].
Recognizing the CMI of the teeth, in the areas of intimate contact with the oral mucosa as a potential carcinogen, has a high impact on the design of prevention and treatment strategies [17].
Patients and Methods
This descriptive, prospective study was approved by the Research and Ethics Committee of the Dental Department of National University of Cuyo (UN CUYO) Mendoza, Argentina, in accordance with the declarations of Nüremberg, Helsinki, and Tokyo of the World Medical Association. This study was carried out with 28 patients, who attended the Clinic of the Dental Department of the National University of Cuyo (UN CUYO) Mendoza, Argentina. The sample included individuals over 18 years old of both genders, with complete permanent dentition up to the first molar in the upper and lower arches, who have not had orthodontic treatment, and presented some alteration of traumatic origin on the edge of the tongue (for example: indentations, erythema, erosion, atrophy, ulceration, keratosis, hyperplasia, petechiae, phlyctena, slough, scar, hair loss, perforation, verrucosity, keratosis, plaque, macula, vegetation, cracks, fissures etc.).
All of the patients signed a written consent and had been completely analyzed (Clinical history, clínical review, impressions models, photography of the lesions and the dental arches), the scanning of the models was carried out with Planmeca cone beam computed tomography equipment available at the Dental Department, of the UN CUYO, in order to obtain a scan of the model and an image of the 3D model, with computerized tracing available in the tomograph software, of the shape of both dental arches.
The variables to observe were:
- Dental arches: shape, size
- Shape of the dental arch: photographic record, clinical analysis, impressions, study models, scan of the models.
- Tongue: size, pathology type and description, time of evolution of the pathology.
- Pathological history: habits, tobacco, alcohol, tics, allergies, rhinitis, piercing (perforation)
- Family history: Head and neck cancer.
- Parafunctional habits: diurnal and nocturnal bruxism, onychophagia, buccal mucosa suction, phagedenic activity.
- Dental trauma on the mucous membranes
- Dental elements: wear facets, overflowing reconstructions, dental fractures, poorly polished amalgams, sharp cusps.
Statistical Model
Quantitative data were described using media values, and qualitative data were expressed as percentages. Data were processed using, Chi-Square test. All statistical analyses were performed with Infostat (v. 2015, http://www.infostat. com.ar).
Results
Of the 28 patients studied, 15 were men and 13 were women, with an average age of 31.8 years old.
Dental Trauma
Upon clinical observation of the dental elements, it was identified that some pieces can generate trauma on the mucous membranes. It is noteworthy that the most frequent dental pathology observed were: attrition facets in 13 patients, followed by sharp cusps in 11 patients, overflowing reconstructions were found in 2 patients, poorly polished amalgams in 2 patients, and dental fractures in 2 patients. Dental Arches When we observed clinically, corroborated with the plaster models, confirmed the diagnosis, and the model was scanned in the tomograph, we were able to trace the shape of the dental arches.
Upper Arch
We found 4 patients with a round upper arch equivalent to 14% of the total, 1 patient with a square upper arch meaning 4% of the total, 4 patients with a V-shaped upper arch equivalent to 14% of the total, 14 patients with hyperbolic shaped upper arch signifying 50% of the total, 1 patient with ovoid upper arch representing 4% of the total, 4 patients with parabolic upper arch encompassing to 14% of the total (Table 1).
| Upper arch form | Number of patients |
| Round | 4 |
| Square | 1 |
| V-arch | 4 |
| Hyperbolic | 14 |
| Ovoid | 1 |
| Parabolic | 4 |
Table 2: Upper arch number of patients distribution according to shape.
Lower Arch
We didn’t find a patient with a round-shaped arch, but we found 3 patients with a square- shaped lower arch, which represents 10% of the total, 3 patients with a V-shaped lower arch, equivalent to 10% of the total, 18 patients with hyperbolic lower arch meaning 65% of the total, 1 patient with ovoid lower arch signifying 5% of the total, 3 patients with parabolic lower arch including 10% of the total (Table 2).
| Lower arch form | Number of patients |
|---|---|
| Round | 0 |
| Square | 3 |
| V-arch | 3 |
| Hyperbolic | 18 |
| Ovoid | 1 |
| Parabolic | 3 |
Table 1: Lower arch number of patients distribution according to shape.
Pathologies of the Tongue in Relation To the Size of the Jaws
In the relationship between the most frequent pathologies of the tongue and the size of the maxillary, it was observed that the greatest number of pathologies developed in patients with a upper and lower jaw of normal size on clinical observation.
When we observed the size of the jaws clinically and in the images of the scanned models, we found:
- Atretic palate 3 patients
- Normal palate 25 patients
- Atretic jaw 9 patients
- Normal jaw 19 patients
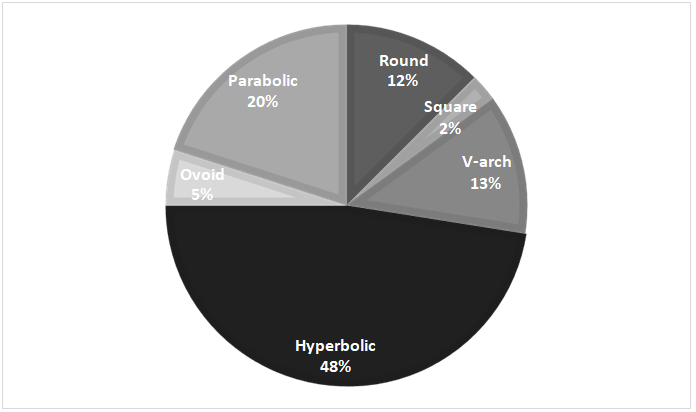
Relationship form of upper dental arch / type of lesion on the edge of the tongue Upper arch
The patients with the highest number of lesions were those with hyperbolic upper arch. This included 48% of all diagnosed lesions, 20% of all lesions were detected in patients with parabolic upper dental arch, 13% in dental arch in V, 12% of the lesions diagnosed occurred in patients with a round dental arch shape, 5% in ovoid arch, and 2% of the lesions appeared in patients with a square upper dental arch (Figure 2).
The variables analyzed, shape of the upper arch and number of lesions, in order to verify whether or not there is a statistically significant relationship between them. It is stated as null hypothesis that the shape of the upper arch is not related to the number of lesions.
It is observed that the chi-square significance value is 10.588 and it is not significant since its value p= 0 .390 is greater than 0.05. Therefore, the null hypothesis is not rejected: both variables are not related. This means that the shape of the upper arch of the patients is not related to the number of lesions.
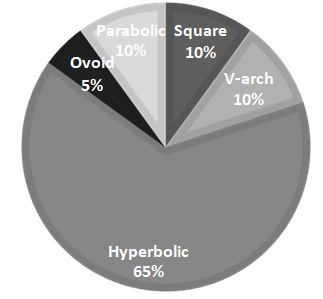
Relation between form of lower dental arch/ type of lesion on the borders of the tongue Lower Arch
65% of all diagnosed lesions occurred in patients with hyperbolic lower arches, 10% in patients with square, V-shaped and parabolic arches, respectively, and 5% in patients with ovoid lower arches (Figure 3).
The variables analyzed, shape of the lower arch and number of lesions, in order to verify whether or not there is a statistically significant relationship between them. It is stated as null hypothesis that the shape of the lower arch is not related to the number of lesions.
It is observed that the chi-square significance value is 14.259 and it is not significant since its p=0.941 value is greater than 0.05. Therefore, the null hypothesis is not rejected: both variables are not related.
Tongue Pathologies Observed
40 lingual pathologies were clinically diagnosed in the 28 patients included in this study (Figure 4).
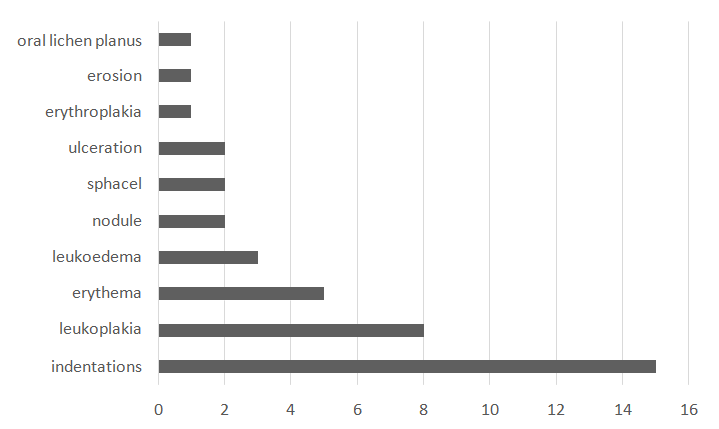
It is noteworthy that among the pathologies described, there were leukoplakias, oral lichen planus, both of them considered potentially malignant disorders (OPMD). There is scientific evidence of a combination of high risk for the development of cancer, when the OPMD are on the edge of the tongue, and it represents an urgent need to carry out the correct follow-up of the patient and eliminate the causes of the traumatic impact [7].
Discussion
To correctly understand the findings of this study, is convenient to consider some characteristics of the population under study. When detecting lesions on the edge of the tongue, in a high percentage of patients we do not find complete dental arches (exclusion criteria), which makes the work difficult and significantly reduces the study population. Evaluating clinical signs, which lead us to detect primary or secondary elementary lesions to arrive at a diagnosis, it is evident that most of the lesions (ulcerations, leukoplakia, indentations) are generated by trauma of the tongue against the dental elements [18]. In most of the patients, more than one pathology has been found in each edge of the tongue observed. A scalloped tongue is the most frequently pathology found in our patients (n=15), usually it isn’t a reason to worry, but its potential causes can lead to further complications, if not treated. The presence of a scalloped tongue may also help diagnose certain medical conditions and identify bad oral habits [19].
When performing the clinical observation of the dental arches and comparing them with the images obtained from the scan of the study models in the computed tomography, it was possible to verify that the clinical diagnoses coincided with the forms recorded in the tomography in all cases.
The generic proportion of lesions we detected has been evaluated. We observed 40 lesions in 28 arches analyzed for each maxilla, which results in a media 1.43 lesions for each dental upper arch described (Table 3).
| Number of patients | Number of lesions | Proportion | |
|---|---|---|---|
| round | 4 | 5 | 1,25 |
| square | 1 | 1 | 1,00 |
| V arch | 4 | 5 | 1,25 |
| hiperbolic | 14 | 19 | 1,36 |
| ovoid | 1 | 2 | 2,00 |
| parabolic | 4 | 8 | 2,00 |
| Total | 28 | 40 | 1,43 |
Table 3: Comparison of data, number of lesions for each upper arch.
In the upper arch, the hyperbolic form, the most frequently observed, is close to the average 1.36, the ovoid and parabolic arches have apparently a greater propensity to generate lesions 2.00 (Table 4).
| Number of patients | Number of lesions | Proportion | |
|---|---|---|---|
| round | 0 | 0 | |
| square | 3 | 4 | 1,33 |
| V arch | 3 | 4 | 1,33 |
| hiperbolic | 18 | 26 | 1,44 |
| ovoid | 1 | 2 | 2,00 |
| parabolic | 3 | 4 | 1,33 |
| Total | 28 | 40 | 1,43 |
Table 4: Comparison of data, number of lesions per lower arch.
In the lower arch, the hyperbolic form is close to the average 1.44, and the ovoid arch has probably a greater propensity to generate lesions 2.00.
Another recorded data was the presence of a lingual frenulum. In our patients we observed, 75% (n= 21) of the patients presented a classic frenulum insertion, 14% (n=4) of patients no frenulum observed, 11% (n= 3) of patients present short and ischemic frenulum when tightened. The impact that the lingual frenulum has on the mobility and lingual tension of the tongue is evident [20]. There is a consensus among the authors concerning the negative effects of lingual frenulum’s in anatomic and functional alterations over craniofacial growth and development [21, 22].
An additional data that was revealed in our patients is the parafunctional habits, we found patients with onychophagia (n=8), patients with nocturnal bruxism (n= 17), patients with daytime bruxism (n=6), patients with mucosal suction (n= 4), some of them present more than one parafunctional habit (n=9), no duration time was recorded. Consequently when this practice is present for months or even years, the tongue is exposed to a continuous mechanical irritation, this emphasizes the need for identifying dysfunctions and parafunctions in order to properly detect oral CMI [23, 24].
CMI should be properly recorded, observing dental morfologie, and its potential interactions with functional factors as well. Recognizing mucosal irritation, in areas of intimate contact with teeth, as a potential risk factor for developing cancer, has a high impact on the design of prevention and treatment strategies [25]. Chronic oral mucosa irritation has a significant association with oral squamous cell carcinoma, for some authors [26, 27]. Elimination of CMI could decrease the risk of oral squamous cell carcinoma [28, 29].
We have not found similar studies in the literature that compare the variables (shape of dental arch and lesions on the edge of the tongue) analyzed in the present work. Defective teeth and ill- fitting dentures have been mentioned in relation to oral cancer. This association is also supported by experimental studies of chemically induced carcinogenesis with CMI that showed an increase in cancer occurrence, higher malignancy grade, and a shorter latency period [30].
We consider that is very important and remains to be evaluated, data on specific measurements such as the degree of lingualization of some teeth, measurements in mm of dental arch length, intercanine and intermolar measurements (first molars) that will enrich the data obtained so far.
Conclusion
- The most frequent dental arch form recorded in our patients was hyperbolic for the upper jaw in 50% of cases, and also hyperbolic for the lower jaw in 63% of cases.
- The most severe pathologies, leukoplakia 8 cases, erythroplasia 1, traumatic ulcerations 2 cases, were recorded in female patients with ovoid and hyperbolic arches, non-smokers who occasionally consume alcohol, with lingualized lower molar, sharp cusps and important attrition facets
- The small dental arches (atretic palate 3 cases, and atretic jaw 9 cases), do not had the highest number of lesions (11 lesions out of a total of 40 lesions found in the sample).
- Each of the forms of dental arch described, present a different way of relating to the tongue.
- The contribution that this work hopes to make, is to systematize, through observation and diagnostic confirmation through study models and images, the relationship within the different structures that confirms the oral cavity.
Detect which the traumatic factors are, and correct them and thus avoid injuries that can trigger potentially malignant disorders.
The link between the hard structures (dental arches) and the tongue contained between the arches, lead us to suspect that each of the forms found, may develop a lesion of relative importance and it should be properly recorded and a follow-up is necessary.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.
Acknowledgment
Diagnostic imaging service of the Faculty of Dentistry of the National University of Cuyo.
References
-
Figun M, Garino R (1986) Anatomía funcionaly aplicada. Editorial El Ateneo, segunda edición pp: 276.
-
Frohlich K, Ingervall B, Schumaker R (1993) Influence of surgical tongue reduction on pressure from the tongue on the teeth. Angle Orthod 63(3): 191-198.
-
Lowe A, Gionhaku N, Takeuchi K, Fleetham J (1986) Three-dimensional CT reconstructions of tongue and airway in adults with obstructive sleep apnea. Am J Orthod Dentofacial Orthop 90(5): 364- 374.
-
Tamari K, Murakami T, Takahama Y (1991) The dimensions of the tongue in relation to its motility. Am J Orthod Dentofacial Orthop 99(2): 140-146.
-
Tamari K, Shimizu K, Ichinose M, Nakata S (1991) Relationship between tongue volume and lower dental arch sizes. Am J Orthod Dentofacial Orthop 100(5): 453- 458.
-
Fröhlich K, Ingervall B, Thüer U (1992) Further studies of the pressure from the tongue on the teeth in young adults. Eur J Orthod 14(3): 229-239.
-
Piemonte ED, Lazos J, Brunotto M (2010) Relationship between chronic trauma of the oral mucosa, oral potentially malignant disorders and oral cancer. J Oral Pathol Med 39(7): 513-517.
-
Lorini L, Bescós Atín C, Thavaraj S, Richter M, Ferranti MA (2021) Overview of oral potentially malignant disorders: from risk factors to specific therapies. Cancers 13(15): 3696.
-
Thumfart W, Weidenbecher M, Waller G, Pesch HJ (1978) Chronic mechanical trauma in the aetiology of oropha- ryngeal carcinoma. J Maxillofac Surg 6(3): 217-221.
-
Warnakulasuriya S (2009) Causes of oral cancer-an appraisal of controversies. Br Dent J 207(10): 471-475.
-
Dayal, Reddy R, Anuradha BK (2000) Malignant potential of oral submucous fibrosis due to intraoral trauma. Indian J Med Sci 54(5): 182-187.
-
Radoï L, Paget Bailly S, Cyr D, Papadopoulos A, Guida F, et al. (2013) Body mass index, body mass change, and risk of oral cavity cancer: results of a large population based case-control study, the ICARE study. Cancer Causes Control 24(7): 1437-1448.
-
Münger K, Baldwin A, Edwards KM, Hayakawa H, Nguyen CL, et al. (2004) Mechanisms of human papillomavirus- induced oncogenesis. J Virol 78(21): 11451-11460.
-
Kreimer AR, Clifford GM, Boyle P, Franceschi S (2005) Human papillomavirus types in head and neck squamous cell carcinomas worldwide: a systematic review. Cancer Epidemiol Biomark Prev 14(2): 467-475.
-
Balkwill F, Mantovani A (2001) Inflammation and cancer: back to Virchow? Lancet 357(9255): 539-545.
-
Virgone A, Badreh S (2021) The 4P: Preventing Preneoplasia through Patients Partnership. Cancers 13(17): 4408.
-
Farah CS, Woo SB, Zain RB, Sklavounou A, Lingen M, et al. (2014) Oral cancer and oral potentially malignant disorders. International journal of dentistry 2014: 853479.
-
Meirelles L, Garcia RCMR (2016) Influence of bruxism and splint therapy on tongue pressure against teeth. Cranio 34(2): 100-104.
-
Klockars T (2013) Short lingual frenulum. Duodecim 129(9): 947-949.
-
Pompéia LE, Ilinsky RS, Ortolani CLF, Faltin K (2017) Ankyloglossia and its influence on growth and development of the stomatognathic system. Rev Paul Pediatr 35(2): 216-221.
-
Jang SJ, Cha BK, Ngan P, Choi DS, Lee SK, et al. (2011) Relationship between the lingual frenulum and craniofacial morphology in adults. Am J Orthod Dentofacial Orthop 139(4): e361-367.
-
Lazos JP, Piemonte ED, Lanfranchi HE, Brunotto MN (2017) Characterization of Chronic Mechanical Irritation in Oral Cancer. Int J Dent 2017: 6784526.
-
Perry BJ, Zammit AP, Lewandowski AW, Bashford JJ, Dragovic AS, et al. (2015) Sites of origin of oral cavity cancer in nonsmokers vs smokers: possible evidence of dental trauma carcinogenesis and its importance compared with human papillomavirus. JAMA Otolaryngol Head Neck Surg 141(1): 5-11.
-
Gupta AA, Kheur S, Varadarajan S, Parveen S, Dewan H, et al. (2021) Chronic mechanical irritation and oral squamous cell carcinoma: A systematic review and meta-analysis. Bosn J Basic Med Sci 21(6): 647-658.
-
Pentenero M, Azzi L, Lodi G, Manfredi M, Varoni E (2021) Chronic mechanical trauma/irritation and oral carcinoma: A systematic review showing low evidence to support an association. Oral Dis.
-
Piemonte ED, Lazos JP, Gilligan GM, Panico RL, Werner LC, et al. (2022) Chronic mechanical irritation enhances the effect of tobacco and alcohol on the risk of oral squamous cell carcinoma: a case-control study in Argentina. Clin Oral Investig.
-
Lockhart PB, Norris CM, Pulliam C (1998) Dental factors in the genesis of squamous cell carcinoma of the oral cavity, Oral Oncol 34(2): 133-139.
-
Velly M, Franco EL, Schlecht N, Pintos J, Kowalski LP, et al. (1998) Relationship between dental factors and risk of upper aerodigestive tract cancer. Oral Oncol 34(4): 284- 291.
-
Rosenquist K, Wennerberg J, Schildt EB, Bladström A, Hansson B G, et al. (2005) Oral status, oral infections and some lifestyle factors as risk factors for oral and oropharyngeal squamous cell carcinoma. A population- based case-control study in southern Sweden. Acta Oto- Laryngologica 125(12): 1327-1336.
-
Pérez MA, Raimondi AR, Itoiz ME (2005) An experimental model to demonstrate the carcinogenic action of oral chronic traumatic ulcer. J Oral Pathol Med 34(1): 17-22.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells