Comparative Study for Fracture Resistance of Open Apex Teeth Filled with two Endodontic Filling Techniques
Objectives: To compare the fracture resistance of open apex endodontically treated teeth filled with two different filling techniques (fluid Gutta-percha and Biodentine®). Material and Methods: 30 human upper central incisors instrumented with a gates glidden n6 drill simulating an open apex were divided into four groups (positive control group, negative group, gutta-percha-filled group and Biodentine®-filled group) were subjected to compressive forces with the aid of a Shimadzu machine until the maximum fracture limit was reached. Results: Although there were descriptive differences between the untreated group (maximum strength) and the instrumented and unfilled tooth (lower strength), we found no significant statistical differences between the filling with Gutta-percha and Biodentine bioceramic cement. The statistical analysis of the data collected for this study was performed using SPSS 23 software with a confidence level of 95%. Chi-square tests and Student t-tests p<0.05 were used for the analysis of the results. Conclusion: Filling a tooth with an open apex always improves fracture resistance as opposed to not filling it, but there are no significant differences between using one specific material or another.
Introduction
A dental fracture is defined by the American Association of Endodontists as a break in enamel and/or dentin and/ or cement which is presumed to be deeper than a fissure of unknown depth or extent, visible or not clinically or radiographically visible and with or without separate tooth segments [1].
In the case of young permanent teeth, when the patient suffers any injury to the pulp tissue, whether due to caries, trauma, deep restorations, etc., irreversible pulpitis of the affected tooth may appear with the consequent paralysis of growth and apical closure. Premature loss of a vital pulp results in a fragile tooth with impaired crown/root ratio, thin dentin walls and a wide and often apically divergent root that poses significant endodontic and restorative challenges. Therefore, the dentist’s main aim is to protect the survival of the pulp until tooth development is complete [2]. If, finally, it is not possible to maintain this pulp vitality and the consequent apical closure, we will opt for apexification.
Apexification, or root-end closure, is the process by which an immature, non-vital permanent tooth that has lost the capacity for root development is induced to form a calcified barrier at the root end. Various sealant materials have been used for this treatment.
The first documented use of a sealer cement was undertaken by Krell and Wefel when they compared the efficacy of calcium phosphate and Grossman’s sealer on extracted teeth, finding no significant difference in adhesion, cohesion and morphological appearance. Subsequently, calcium phosphate cement has been successfully used in endodontic treatments, including pulp capping, periapical defects, apical surgeries, perforations, etc.
On the other hand, bioceramic cements are included in the group of bioactive ceramic materials that are biocompatible (biocompatibility being understood as the capacity of a material not to trigger an adverse reaction such as toxicity, irritation, inflammation, allergy or carcinogenicity) thanks to their physical and chemical properties.
To fully understand bioceramic materials we must differentiate between restorative materials (cements with a putty consistency, used in apexification, perforations, pulp capping, etc.) and sealant materials (cements with a more liquid consistency, mostly used as root filling cements in endodontics).
There are several reasons that may lead us to choose a bioceramic material when it comes to its use in dentistry, such as its excellent biocompatibility, avoiding that it is rejected by the surrounding tissue and above all its excellent physical and chemical capabilities because it contains calcium. This calcium phosphate improves the setting properties and results in a chemical, crystalline composition similar to tooth and bone apatite materials, thus improving the bonding of the sealant to the root dentin [3].
The main problems with these cements are the difficulty of removing them from the canal once they have set together with the tissue damage they can cause to the periapical tissue after extrusion of the cement to the periapex, thus delaying healing, although it has been observed in some studies that other extruded cements can also cause cytotoxicity [4].
There are a large number of bioceramic sealant and restorative materials on the market, since these materials are currently the subject of most dental studies on how to advance in the field of endodontics, their dentin bonding capacity, their biocompatibility in the periapical area and their resistance to fracture, among others, which is the main aim of this study. Among them we can name MTA, undertaken by Torabinejad and collaborators (Pro Root MTA, Dentsply, Tulsa, OK, USA), iRoot SP (Innovative Bioceramix Inc., Vancouver, Canada), Guttaflow (Coltene/Whaledent AG, Altstatten, Switzerland), Biodentine® (Septodont Ltd, Saint Maur des Fraussés, France, etc.
In this study we have focused on comparing the fracture resistance of open apex endodontically treated teeth with two different filling techniques; beta type fluid gutta-percha (B&L Biotech Inc., USA) and Biodentine ® bioceramic cement (Septodont Ltd, Saint Maur des Fraussés, France), using a Shimadzu type machine to simulate tooth fracture until reaching the maximum fracture limit, in this way comparing the resistance of open apex endodontically treated teeth filled with two different filling techniques (fluid Gutta-percha and Biodentine®).
Materials and Methods
Thirty single-rooted upper incisor roots were selected and kept in 0.1% thymol solution (Scharlau, Scharlab S.L, Spain) until the start of the study. Pre-operative radiographs were taken in the mesiodistal and vestibulopalatine direction to ascertain the existence of a single root, as well as a single canal or relevant anatomical anomalies. Teeth with the presence of calcific metamorphosis of the canal, observable fractures or fissures, previous root canal treatments, severe curvatures, root resorptions, dilacerated roots or teeth with root caries were also discarded.
The crown of the tooth was removed with the aid of a diamond disc under profuse irrigation until 12 mm long roots were obtained. A digital caliper was used to measure the vestibulopalatine and mesiodistal diameter of the coronal plane for standardization.
After the removal of the crown and standardization, the teeth were randomly divided into four groups: a positive control group, a negative control group, a group filled with fluid gutta-percha and a group filled with Biodentine® restorative cement.
The initial working length was taken with a size 15 K file (“Dentsply Maillefer, Ballaigues, Switzerland”) inserting until the tip appeared in the apical foramen, then reducing 1 mm of its length. All root canals were instrumented with a Gates Glidden bur until reaching No. 6 with profuse water irrigation. Intra-duct irrigation was performed with 3 ml sodium hypochlorite (NaOCl 5.25%) between each bur in a 27 gauge monoject needle (Biodent CO., LTD, Gyoenggi- do, Korea). The smear layer was removed with 3ml 17% EDTA, the canal was rinsed with 10ml distilled water before drying with protaper gold F5 paper tips (“Dentsply Maillefer, Ballaigues, Switzerland). Irrigants were activated using the Endoactivator instrument in 30-second sessions. (Dentsply
Tulsa Dental Specialities, Tulsa, OK, USA) (Table 1).
| N=5 | Positive Control/Healthy Tooth | |
| Group I | N=5 | Negative Control/Instrumented but Unfilled Tooth |
| Group II | N=5 | Root Canals Filled with Gutta-Percha and AH Plus® Sealer Cement |
| Group III | N=10 | Root Canals Filled with Gutta-Percha and AH Plus® Sealer Cement |
| Group IV | N=10 | Root Canals Filled with Root Repair Biodentine® Material |
Table 1: Positive control group, Negative Group, Gutta-Percha-Filled Group and Biodentine®-Filled Group.
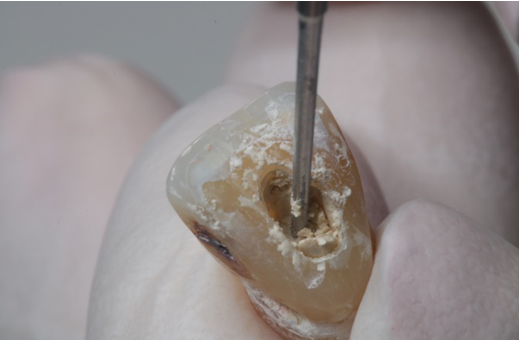
Biodentine® bioceramic restorative material was introduced by injecting the material through the canal entrance with a MAP system material type conveyor, Dentsply Maillefer and compacted with a Buchanan type No. 1 and No. 2 hand-held striker, Sybronendo, Orange, CA, USA (Figure 1).
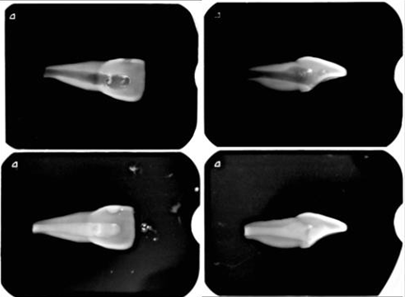
Finally, periapical radiographs were taken mesiodistally and vestibulolingually to ensure their complete filling. Finally, the sealing of the crown was performed with temporary filling material “Cavit TM, 3MTM, ESPE TM, MN, U. S”. In order for the sealants to fully set, all samples were stored at 100% humidity and 37°C for 14 days Figure 2.
After preparation of the teeth and clarifying the mechanical and material conditions with the engineer in charge from the Polytechnic University of Valencia, a thickness of 0.2-0.3 mm orthodontic wax was used to cover 5 mm of all roots apically to mimic a periodontal ligament.
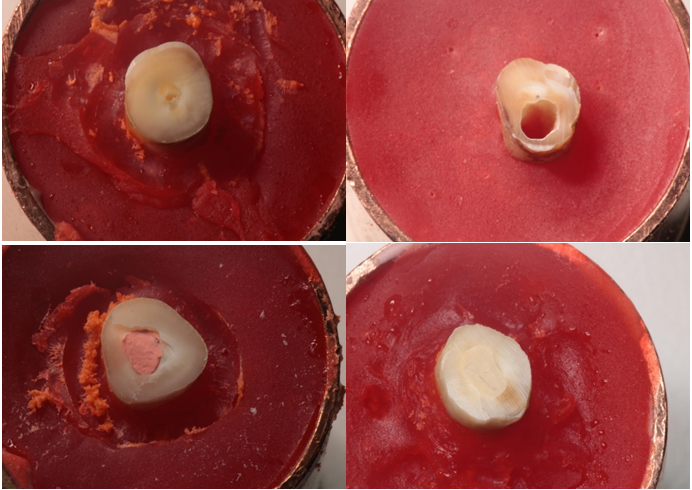
A digital calliper was used to measure the uniform wax thickness. The samples were placed in copper cylinders (50 mm in height and 24 mm in diameter) in a vertical position, embedding 5 mm of the root length in Duralay® (Reliance, Dental MFG.CO.) inside the copper cylinder Figure 3.
Fracture toughness was tested using a universal testing machine “Shimadzu AG-X Plus, Japan”. The acrylic blocks were placed on the bottom plate of the instrument. The upper plate has a diameter of 2.8 mm diameter and spherical steel tip. The tip compressed the centre of the canal and exerted vertical load (1 mm/min) until fracture occurred. The maximum force applied to fracture each root was recorded in Newton (N) (Figures 4-6).
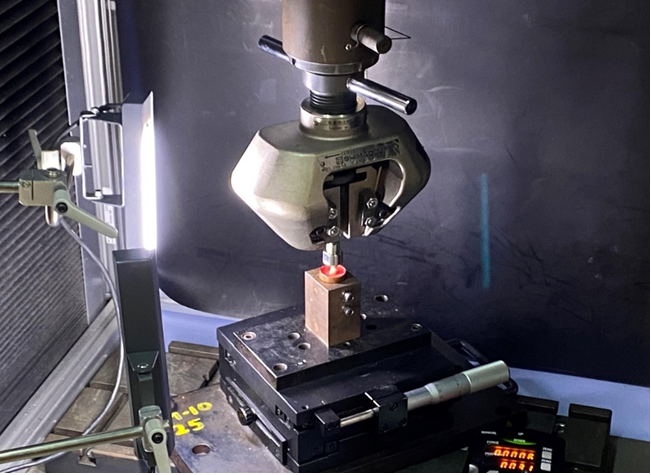
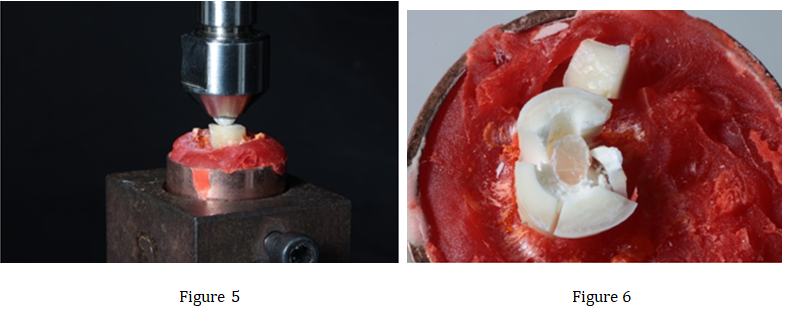
Figures 5 & 6: Tooth prepared for fracture resistance test and tooth finally fractured.
Our main variable or study variable (dependent variables) was the pressure supported by the tooth until fracture (quantitative variable).
The statistical analysis of the data collected for this study was performed using SPSS 23 software with a confidence level of 95%. (p<0.05) Chi-square tests and Student t-tests p<0.05 were used for the analysis of the results.
Results
The average pressure supported until breakage by the teeth treated with Biodentine® was 1208.03 N, those treated with Gutta-percha 1211.26 N, untreated teeth 1503.74 N and teeth with root flaring 711.33 N.
| N | Average Maximum Supported Force | |
|---|---|---|
| Positive control | 5 | 1503.74 |
| Negative control | 5 | 711.33 |
| Gutta-percha + AH plus | 10 | 1208.03 |
| Biodentine | 10 | 1211.26 |
Table 2: Average Maximum Supported Force.
We observed that the maximum force supported by the untreated teeth was higher than that of the flared teeth and that the maximum force supported by the teeth with root flaring was less than that of the rest of the teeth. We assessed whether these differences were statistically significant.
As the sample size was small, we performed a normality test to observe whether the samples came from populations with normal distribution or not and thus choose the type of statistical analysis to perform.
The p-value of the contrast statistic of the Anova test was 0.209 > 0.05, so we found no statistical evidence to say that the maximum force supported by the four groups is significantly different.
The p-values of the four groups were greater than 0.05, so we can assume that the four samples are from normal populations and we will use parametric methods of comparison.
To see which parametric test we should use, we performed a Levene’s test for homogeneity of variances.
The p-value of the contrast statistic of Levene’s test was 0.154 (p<0.05), so we could assume that the variances of the four groups were equal and therefore we used the parametric Anova test to compare the results of the four groups.
The p-value of the contrast statistic of the Anova test was 0.209 > (p<0.05), so we found no statistical evidence to say that the maximum force supported by the four groups is significantly different Tables 3-5.
| Treatment | Shapiro-Wilk | ||
|---|---|---|---|
| Statistic | gl | p-value | |
| Biodentine | 0,941 | 10 | 0,559 |
| Gutta-percha | 0,873 | 10 | 0,108 |
| Positive control | 0,972 | 5 | 0,890 |
| Negative control | 0,928 | 5 | 0,583 |
| Levene’s test | GL1 | GL2 | p-value |
| 1,903 | 3 | 26 | 0,154 |
Table 3: Normality tests maximum force supported.
Test for homogeneity of variances Maximum force supported
| Sum of squares | GL | RMS | FF | p-value | |
|---|---|---|---|---|---|
| Intergroup | 1639336434 | 3 | 546445,478 | 1,618 | 0,209 |
| Intragroup | 8778997,796 | 26 | 337653,761 | ||
| Total | 1,042E7 | 29 |
Table 4: ANOVA.
Discussion
Fully developed teeth have a sufficiently thick dentin wall to give the tooth adequate fracture resistance. In contrast, immature teeth lack this wall quality which makes them prone to fracture. Therefore, the viability of the tooth depends to a great extent on the type of treatment we perform.
The problems associated with the use of apexification with calcium hydroxide have promoted the apex-formation technique with bioceramic cements in a single visit to avoid future complications.
As a large number of researchers have shown, MTA is an excellent option for apical capping but it has some drawbacks such as the difficulty in handling, the long setting time of the material (about 72 hours) that leads the clinician to have to perform the treatment in two sessions, the colour change caused by this material on the tooth, the low resistance to compression, etc. [5].
For this reason, as an alternative, a calcium silicate-based restorative cement such as Biodentine® has recently been introduced as a filling material for these types of pathology.
In literature we have found a considerable number of authors who have investigated open apex dental fracture, but so far and due to the large number of new bioceramic cements, literature is scarce in the fact of comparing teeth with open apex where these materials have been used. Most studies compare Gutta-percha (gold standard) and resin cements, glass ionomer-based cements or MTA, the latter adding a very considerable increase in working time and the impossibility of performing the treatment in a single session [6].
Regarding the method used to undertake this study, we have found in literature that there are coincidences with our results in the fact that there is a significant difficulty in correctly obturating a high calibre canal with Biodentine in its entirety, which we have empirically observed when filling the widened canal without observing spaces or gaps in the postoperative radiographs [7, 8].
The vast majority of studies agree with us when it comes to the use of materials, such as the study by Soares et al, in which orthodontic wax was also used to simulate the periodontal ligament [9]. We have found numerous studies that employ our same irrigation protocol, 5.25% hypochlorite, and 17% EDTA, [10] embedding the teeth in copper cylinders embedded in Duralay and using Instrom or Shimadzu type machines to perform the compressive fracture resistance test [11, 12, 13].
Regarding the results, we have found some studies that, thanks to finite element analysis, manage to find results similar to ours without the need for such practical material and methods as ours, taking advantage of excellent in vitro digital tools available today. In the study by Eram, et al. [14] they found significantly lower fracture resistance in open apex teeth with a 4mm MTA apical cap as opposed to the same size Biodentine ® apical cap, which makes this an excellent choice for the production of our apical stop.
With regard to the improvement in resistance to fracture between teeth in the control group (healthy untreated tooth) and those filled with Gutta-percha, most of the studies we have found agree that the control group always withstands the pressure of the compressive force better than the tooth that is filled with Gutta-percha [15].
We have found some studies, such as that of Kazandag, et al. which found no significant differences between the control group and the group filled with Gutta-percha (these studies thus giving more importance to the sealant material than to the amount of dentin remaining), [16] but in general the large number of studies agree that it is the amount of dentin that improves resistance to fracture [17, 18].
On the other hand, a significant number of studies show that Biodentine® does improve fracture resistance in vertical compression tests when filling teeth with open apices and teeth with normal canal caliber [19, 20].
The vast majority of studies do coincide in the fact that the fracture resistance always improves in a tooth that is filled rather than unfilled, i.e., with regard to our study, in most of the literature it is the negative control group (treated tooth, but not filled) that presents lower values in terms of fracture resistance [21, 22, 23].
Most studies that have compared fracture resistance
with bioceramic cements add a fiberglass post to improve the ability to resist this compressive forces [24].
Conclusion
Filling a tooth with an open apex always improves fracture resistance as opposed to not filling it, but there are no significant differences between using one specific material or another.
References
-
American association of endodontics (2020) Glossary of Endodontic Terms. 10th (Edn.), Chicago.
-
Hargreaves K, Berman L, Rotstein I (2016) Cohen, Vías de la pulpa. Barcelona: Elsevier.
-
Cherng AM, Chow LC, Takagi S (2001) _In vitro_ evaluation of a calcium phosphate cement root canal filler/sealer. J Endod 27(10): 613-615.
-
Viapiana R, Baluci CA, Tanomaru Filho M, Camilleri J (2014) Investigation of chemical changes in sealers during application of the warm vertical compaction technique. Int Endod J 48(1): 16-27.
-
Bachoo IK, Seymour D, Brunton P (2013) Clinical case reports using a novel calci- um-based cement. Br Dent J 214(2): 61-64.
-
Topçuoglu HS, Tuncay O, Karatas E, Arslan H, Yeter K (2013) _In Vitro_ Fracture Resistance of Roots Obturated with Epoxy Resin–based, Mineral Trioxide Aggregate– based, and Bioceramic Root Canal Sealers. J Endod 39(12): 1630-1633.
-
Elnaghy A, Elsaka SE (2016) Fracture resistance of simulated immature teeth filled with Biodentine and white mineral trioxide aggregate-an _in vitro_ study. Dent Traumatol 32(2): 116-120.
-
Osiri S, Banomyong D, Sattabanasuk V, Yanpiset K (2018) Root Reinforcement after Obturation with Calcium Silicate–based Sealer and Modified Gutta-percha Cone. J Endod 44(12): 1843-1848.
-
Soares CJ, Pizi ECG, Fonseca RB, Martins LRM (2005) Influence of root embedment material and periodontal ligament simulation onfracture resistance tests. Braz Oral Res 19(1): 11-16.
-
Plotino G, Maria Grande N, Isufi A, Ioppolo P, Pedullà E, et al. (2017) Fracture strength of endodontically treated teeth with different access cavity. J Endod 43(6): 995- 1000.
-
Elnaghy A, Elsaka S (2019) Fracture resistance of simulated immature roots using Biodentine and fiber post compared with different canal-filling materials under aging conditions. Clin Oral Investig 24(3): 1333- 1338.
-
Almohaimede A, Almaine D, Alaathy S (2020) Fracture resistance of roots filled with bio-ceramic and epoxy resin-based sealer: _In vitro_ study. Eur Endod J 5(2): 134- 137.
-
Evren OK, Altunsoy M, Tanriver M, Capar ID, Kalkan A, et al. (2016) Fracture resistance of simulated immature teeth after apexification with calcium silicate-based materials. Eur J Dent 10(2): 188-192.
-
Eram A, Zuber M, Keni LG, Kalburgi S, Naik R, et al. (2020) Finite element analysis of immature teeth filled with MTA, Biodentine and Bioaggregate. Comput Methods Programs Biomed 190: 105356.
-
Marchi V, Scheire J, Simon S (2020) Retreatment of Root Canals Filled with BioRoot RCS: An _In Vitro_ Experimental Study. J Endod 46(6): 858-862.
-
Kazandag K, Sunay H, Tanalp J, Bayirli G (2009) Fracture resistance of roots using different canal filling systems. Int Endod J 42(8): 705-710.
-
Elnaghy A, Elsaka SE (2016) Fracture resistance of simulated immature teeth filled with Biodentine and white mineral trioxide aggregate-an _in vitro_ study. Dent Traumatol 32(2): 116-120.
-
Almohaimede A, Almaine D, Alaathy S (2020) Fracture resistance of roots filled with bio-ceramic and epoxy resin-based sealer: _In vitro_ study. Eur Endod J 5(2): 134- 137.
-
Guneser MB, Akbulut MB, Eldeniz AU (2013) Effect of Various Endodontic Irrigants on the Push-out Bond Strength of Biodentine and Conventional Root Perforation Repair Materials. J Endod 39(3): 380-384.
-
Sarraf P, Nekoofar MH, Sheykhrezae MS, Dummer PH (2019) Fracture resistance of immature incisors using various endodontic biomaterials. Dental investigations society 13: 156-160.
-
Ulusoy OI, Paltun YN (2016) Fracture resistance of roots with simulated internal resorption defects and obturated using different hybrid techniques. J Dent Sci 12(2): 121-125.
-
Topçuoglu HS, Tuncay O, Karatas E, Arslan H, Yeter K (2013) _In Vitro_ Fracture Resistance of Roots Obturated with Epoxy Resin–based, Mineral Trioxide Aggregate– based, and Bioceramic Root Canal Sealers J Endod 39(12): 1630-1633.
-
Ulusoy OI, Paltun YN (2016) Fracture resistance of roots with simulated internal resorption defects and obturated using different hybrid techniques. J Dent Sci 12(2): 121-125.
-
Bayram E, Bayram HM (2016) Fracture resistance of immature teeth filled with mineral trioxide aggregate, bioaggregate, and biodentine. Eur J Dent 10(2): 220-224.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells