Miniscrew Implant a Paragon of Anchorage in Contemporary Orthodontics-A Mini-Review
Temporary anchorage devices (TADs) are temporarily fixed to the bone to enhance orthodontic anchorage. Miniscrew implant is a temporary anchorage device (TAD) which provides better anchorage than conventional anchorage system. The miniimplants have allowed the management of wider discrepancies because force can be applied directly from the bone-borne anchor unit. Therefore, miniscrew implant enables the orthodontists to treat complex orthodontic cases which require higher anchorage control in three dimensions. The Present review discusses about the indications, contraindications, risk factors and placement protocol of miniscrew implant in routine orthodontic practice. Additionally, the biomechanical considerations and recent advancements are reviewed. Finally, a representative case showing absolute anchorage is also presented.
Introduction
Temporary anchorage devices (TADs) are temporarily fixed to the bone to enhance orthodontic anchorage and removed thereafter. TADs can be fixed to bone either mechanically (cortically stabilized) or biochemically (osseointegrated). Since its introduction, skeletal anchorage in orthodontics has gained increasing popularity in clinical applications and research Creekmore and Eklund [1]. Three types of TADs are commonly used in orthodontics: Mini plate, i.e. bone-anchored, length-reduced miniscrew implants i.e. Palatal implants and diameter-reduced mini- implants i.e, Miniscrew [2]. Orthodontic mini-implants or temporary intraoral skeletal anchorage devices (TISADs) are a compliance-free alternative to more traditional forms of anchorage [3]. TISADs are considered simple to place and have reported survival rates ranging from 80% to 94% [4]. Historically, Vitallium screws and stainless-steel wires were used in dog mandibles to retract the canine [5]. It worked on the concept of osseointegration [6]. The first reported patient treatment with osseointegrated implants was a blade implant placed to anchor rubber bands to retract teeth [7]. Another study reported using Vitallium bone-screw was used just below the anterior nasal spine to treat overbite [1]. Robert corroborated the use of implants in orthodontic anchorage [8]. First reported, the clinical use of miniscrew implant for orthodontic anchorage was the intrusion of mandibular incisors [9].
Indications of Miniscrew Implant
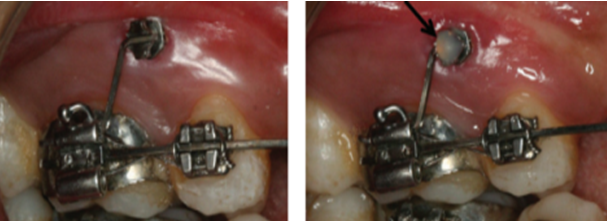
It is widely used for the closure of edentulous space, which avoid the need of a prosthesis. It helps in the intrusion and extrusion of the teeth, reduces complications and facilitates easier tooth movement. It is also used to reposition malposed teeth as it helps to control anchorage during orthodontic tooth movement (Figure 1). It reinforces anchorage during complex tooth movement; palatal implants improve patients’ compliance. Therefore, it is a good alternative for Class II elastics and headgear. It is used in partially edentulous cases, which serve as a future restorative abutment. It corrects undesirable occlusion and provides solid anchorage to retract the entire arch. It also facilitates localized bonding and reduces anchorage loss during orthodontic treatment. In the transverse direction, miniscrew implant can be used for correction of dental midline [10, 11], correction of dental and skeletal asymmetries. It is recently used during orthopedic movement, which also accelerates sutural distraction (palatal expansion) and bone movement (MARPE-miniscrew implant assisted palatal expansion) [12, 13]. In the vertical direction, it is used in the cases of deepbite and openbite correction [14].

Limitations of Miniscrew Implant use
Miniscrew implant is not indicated in patients having systematic diseases that affect bone metabolism. Patients younger than 12 years who have yet not completed skeletal growth, as shown by a hand-wrist radiograph, should have palatal miniscrew placed away from the midline suture in the paramedian region. Miniscrews are contraindicated in heavy smokers and patients with bone metabolic disorders. MSI should not be placed in the areas of bone remodeling, such as a healing socket or near a deciduous tooth. Thin cortical bone limits the use of miniscrew implants because miniscrew implants are mechanically retained and loosening of a screw can develop because of thin cortical bone. Lack of clinical skills limits its usage. Enthusiastic usage of invasive and costly procedures in all patients is not recommended [15].
Implant materials
The material must be non-toxic and biocompatible, possess excellent mechanical properties, and provide resistance to stress, strain, and corrosion. The commonly used materials can be divided into 3 categories [16]:
- biotolerant (stainless steel, chromium-cobalt alloy)
- bioinert (titanium, carbon)
- bioactive (hydroxylapatite, ceramic oxidized aluminum).
Titanium is an ideal material as it has no allergic and immunological reactions and no neoplasm formation [17]. The bone grows along the titanium oxide surface, which is formed after contact with air or tissue fluid. However, pure titanium has less fatigue strength than titanium alloys. A titanium alloy-titanium-6 aluminum-4 vanadium-is used to overcome this disadvantage.
Safe Zone for Miniscrew Implant
Miniscrew implants are available in varying lengths and diameters to accommodate placement at different sites in both jaws. Most miniscrew implants have a thread diameter ranging from 1.2 mm to 2.0 mm and a length ranging from 6.0 mm to 12.0 mm [18]. The safe zone for mini-implant placement in the posterior region is inter radicular bone of the maxilla and mandible in the molar and premolar area. In the anterior region, it is placed between the central and lateral incisor at 6mm above cementoenamel junction [19]. One screw each can be placed on either side of the central and lateral incisor. A single screw can also be placed in the maxilla in the midline. The other locations for the miniscrew implant placement are mandibular symphysis, retromolar, infra-zygomatic and maxillary tuberosity area [20].
Bone Quality and Quantity
The primary stability is dependent upon cortical bone thickness, which is an essential factor for miniscrew implant placement. The cortical bone thickness of less than 1mm has a higher chance of implant failure [21, 22]. Studies have shown that as the cortical thickness increases, deflection of miniscrew implant decreases [22]. The cortical bone thickness of less than 1mm is vulnerable to bone resorption due to stress caused during orthodontic tooth movement [23]. The important factor for primary stability of bone is bone quality and quantity, which affect the long-term success of miniscrew implant. Bone quality can be assessed clearly by cone-beam computed photography. It is advisable to perform CBCT imaging in patients who require miniscrew implant placement [24].
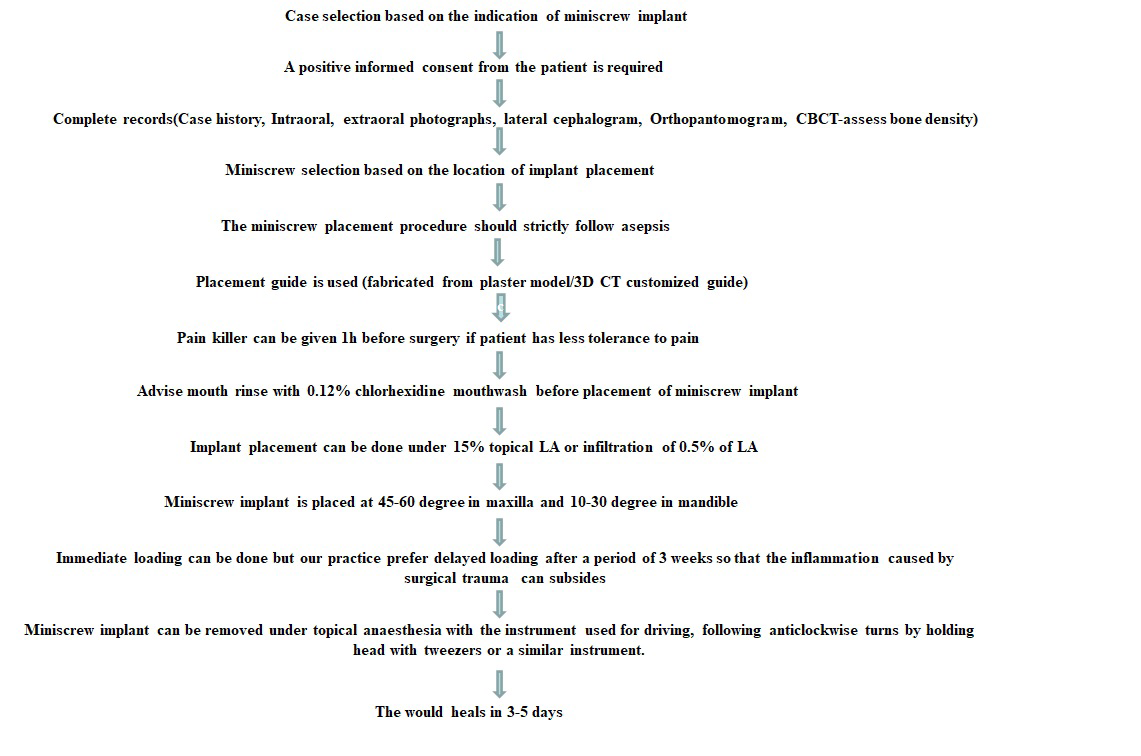
Protocol of Mini Screw Implant Placement
A thorough case history is to be taken. Positive informed consent is required before the start of the treatment. The patient should be motivated enough to maintain oral hygiene (Figure 2) [25, 26, 27]. Complete records including intraoral and extraoral photographs, upper and lower study models, x rays are required. CBCT is an additional diagnostic aid which is done for the assessment of bone density a) Miniscrew selection: The inter radicular bone and the buccolingual dimension of the alveolus are to be examined before miniscrew implant placement. The nasopalatal thickness should also be examined. The miniscrew implant are longer in length used in the retromolar area. The conventional miniscrew implant are used in the inter radicular bone of the maxilla and mandible. The implants larger in diameter used in the anterior palate. b) Surgical procedure: The implant placement procedure should strictly follow asepsis. The placement guide is fabricated in a recent plaster model, or 3D CT customized guide can be used. The patient is advised to start with 250mg amoxicillin or suitable antibiotic on the night before the surgery. The pain killer can be given 1h before surgery if the patient has less tolerance to pain. The patient is asked to rinse with 0.12% chlorhexidine mouthwash before starting the procedure. The implant placement is done under 15% topical LA or infiltration of 0.5% of LA. The miniscrew implant is placed at 45-60 deg in the maxilla and 10-30 deg in the posterior mandible. The postoperative phase requires strict maintenance of oral hygiene. c) Loading of implant: The immediate loading can be done but our practice prefers delayed loading after 3 weeks so that the inflammation caused by surgical trauma can subsides d) Miniscrew removal: MSI can be removed under topical anesthesia with the instrument used for driving, following anticlockwise turns by holding the head with tweezers or a similar device. The wound heals in 3-5 days.
Biomechanics Considerations of Miniscrew Implant Placement
The miniscrew implant is a temporary anchorage device. It utilizes direct and indirect anchorage during space closure. Direct anchorage refers to the movement of teeth using orthodontic miniscrew implant, whereas indirect anchorage refers to the stabilization of certain teeth in the dental arch and subsequent use of these stabilized anchors to move other teeth [28, 29] (Figures 3 & 4). The intrusion of anterior teeth is carried out in deep bite cases, while intrusion of posterior teeth is carried out in open bite case [30]. Uprightening of the molar is an important indication of a miniscrew implant. Mild, moderate, and severe tipping is approached differently. In case of mild mesial tipping, assembly of miniscrew placed mesially, and an open coil spring with distally directed force can be used. In the case of moderately tipped molars, Miniscrew is placed mesially, use of an open coil spring for unlocking the molar is recommended, followed by an uprighting spring. In severe tipping, it is difficult to bond the molar on the buccal aspect. A miniscrew distal to the tipped molar is used, the preferable sites are the retromolar pad area or the tuberosity area.

Risks and Complications with the use of Miniscrew
Papadopoulos’s meta-analysis reported that the failure rate of miniscrew implant is 0.123(87.7% success rate) [31]. The studies have shown that age, sex, insertion site, and insertion side (left/Right) does not affect the failure rate [21, 32, 33]. It has been reported that there is a difference in the rate of success and failure of MSI in maxilla and mandible [34]. The higher survival rate of 100% in the maxilla is seen and 76.33% in the mandible [35]. The higher failure rate in human mandibles is attributed to the greater bone density of the mandible, resulting in higher insertion torque values, bone overheating, and less cortical bone formation around the MSI, which is also limits cleaning of the area [33]. However, failure risks tend to be higher in younger (20 years old) patients [20, 36, 37], probably due to the active bone metabolism and low maturation of the maxillofacial bone in growing children [22]. The higher the insertion torque, the higher will be the failure rate. A study reported that insertion torque values higher than 10 Ncm are associated with a higher failure rate [21, 38]. The root contact to the teeth can be another contributing factor for implant failure but root injuries are usually treatable [39, 40]. Finite element analysis [24, 41] can do the stress simulation. The other complications during mini-implant placement can be trauma to periodontal ligament, miniscrew slippage, nerve injury, subcutaneous emphysema, nasal and maxillary sinus perforations. Miniscrew migration may also occur in rare cases as a complication of implant placement. Soft tissue complications include oral ulceration, soft tissue coverage of miniscrew head and auxiliary, peri-implantitis [42].
Implant Maintenance and Post-Operative Care
After surgery, the surrounding soft tissues must be maintained to ensure the longevity of the implant. Plaque accumulation near the gingival margin can cause perimucositis or peri-implantitis. Therefore, patients must be instructed to follow daily plaque control at home and have regular professional care.
Recent Advancement
With the advent of miniscrew implants, the orthopaedic correction have been possible in the three dimensions of the craniofacial structures. MARPE (miniscrew implant assisted rapid palatal expansion) is recently used for orthopaedic transverse maxillary expansion. Studies have reported that higher amount of orthopaedic expansion can be achieved with MARPE as compared to conventional expansion appliances [43]. A CAD CAM assisted customised miniscrew implant retained appliances are recently used in orthodontics. Direct 3-dimensional metal printing via laser melting is used for the construction of appliance such as miniscrew assisted hyrax for transverse expansion [44]. Recent studies also discuss about the role of biomarkers in the secondary stability of mini- implant. The change in the levels of biomarkers such as IL-1 [45], OPG/RANKL [46], TNF-α [47] and circulating cell free nucleic acids [48] in peri-miniscrew implant crevicular fluid have shown an association with the secondary stability of miniscrew implants. Studies have reported that higher level of biomarkers has an association with peri-implantitis which is a potential causative factor for miniscrew implant failure [49].
Future Perspectives
The miniscrew implants in various clinical situations need further clinical trials. The success rate of miniscrew implants is affected by mechanical as well as biological factors. Therefore, prospective randomised trials should be done to assess biological markers and their role in miniscrew implants stability. The clinical trials with 3D guided splints should be promoted during miniscrew implants placement. Using artificial intelligence, the diagnosis and treatment planning can be automated, and the inconsistencies can be reduced to improve the success rates for miniscrew implants.
Conclusion
The miniscrew implant as temporary anchorage device enables better anchorage preservation compared with traditional reinforcement system. It has enhanced the limit for Envelop of discrepancy for nonsurgical management. The miniscrew implant is not a magic wand, but rather a valuable tool to enhance the quality of orthodontic treatment.
References
-
Creekmore TD, Eklund MK (1983) The possibility of skeletal anchorage. J Clin Orthod 17(4): 266-269.
-
Cope JB (2005) Temporary Anchorage Devices in Orthodontics: A Paradigm Shift. Semin Orthod 11(1): 3-9.
-
Antoszewska Smith J, Sarul M, Łyczek J, Konopka T, Kawala B (2017) Effectiveness of orthodontic miniscrew implants in anchorage reinforcement during en-masse retraction: A systematic review and meta-analysis. Am J Orthod Dentofacial Orthop 151(3): 440-455.
-
Kuroda S, Sugawara Y, Deguchi T, Kyung HM, Takano Yamamoto T (2007) Clinical use of miniscrew implants as orthodontic anchorage: success rates and postoperative discomfort. Am J Orthod Dentofacial Orthop 131(1): 9-15.
-
Gainsforth BL, Higley LB (1945) A study of orthodontic anchorage possibilities in basal bone. Am J Orthod Oral Surg 31(8): 406-417.
-
Branemark PI, Breine U, Adell R (1969) Intraosseous anchorage of dental prostheses. I. Experimental studies. Scand J Plast Reconstr Surg 3(2): 81-100.
-
Linkow LI (1969) The endosseous blade implant and its use in orthodontics. Int J Orthod 7(4): 149-154.
-
Roberts WE, Smith RK, Zilberman Y, Mozsary PG, Smith RS (1984) Osseous adaptation to continuous loading of rigid endosseous implants. Am J Orthod 86(2): 95-111.
-
Kanomi R (1997) Mini-implant for orthodontic anchorage. J Clin Orthod 31(11): 763-767.
-
Jung MH (2021) Treatment of facial asymmetry and severe midline deviation with orthodontic mini- implants. Am J Orthod Dentofacial Orthop 160(2): 312- 324.
-
Chung KR, Kim SH, Choo H, Kook YA, Cope JB (2010) Distalization of the mandibular dentition with mini- implants to correct a Class III malocclusion with a midline deviation. Am J Orthod Dentofacial Orthop 137(1): 135-146.
-
Carlson C, Sung J, McComb RW, Machado AW, Moon W (2016) Microimplant-assisted rapid palatal l to orthopedically correct transverse maxillary deficiency in an adult. Am J Orthod Dentofacial Orthop 149(5): 716- 728.
-
Sugawara J (1999) Dr. Junji Sugawara on the skeletal anchorage system. J Clin Orthod 33(12): 689-696.
-
Chang J, Mehta S, Chen PJ, Upadhyay M, Yadav S (2019) Correction of open bite with temporary anchorage device- supported intrusion. APOS Trends in Orthodontics 9(4): 246-251.
-
Kharbanda OP (2013) Orthodontic treatment with contemporary fixed appliance. In: Kharbanda OP (Eds.), Orthodontics: Diagnosis and management of malocclusion and dentofacial deformities, 2nd (Edn.), Elsevier.
-
Misch CE (1999) Contemporary implant dentistry. 2nd (Edn.), Saint Louis: Mosby.
-
Özcan M, Hämmerle C (2012) Titanium as a Reconstruction and Implant Material in Dentistry: Advantages and Pitfalls. Materials (Basel) 5(9): 1528- 1545.
-
Odman J, Lekholm U, Jemt T, Thilander B (1994) Osseointegrated implants as orthodontic anchorage in the treatment of partially edentulous adult patients. Eur J Orthod 16(3): 187-201.
-
Fayed MMS, Pazera P, Christos K (2010) Optimal sites for orthodontic mini-implant placement assessed by cone- beam computed tomography. Angle Orthod 80(5): 939- 951.
-
Poggio PM, Incorvati C, Velo S, Carano A (2006) ‘Safe zones’: a guide for miniscrew positioning in the maxillary and mandibular arch. Angle Orthod 76(2): 191-197.
-
Motoyoshi M, Yoshida T, Ono A, Shimizu N (2007) Effect of cortical bone thickness and implant placement torque on stability of orthodontic mini-implants. Int J Oral Maxillofac Implants 22(5): 779-784.
-
Motoyoshi M, Inaba M, Ono A, Ueno S, Shimizu N (2009) The effect of cortical bone thickness on the stability of orthodontic mini-implants and on the stress distribution in surrounding bone. Int J Oral Maxillofac Surg 38(1): 13- 84.
-
Stahl E, Keilig L, Abdelgader I, Jager A, Bourauel C (2009) Numerical analyses of biomechanical behavior of various orthodontic anchorage implants. J Orofac Orthop 70(2): 115-127.
-
Motoyoshi M, Ueno S, Okazaki K, Shimizu N (2009) Bone stress for a mini-implant close to the roots of adjacent teethe3D finite element analysis. Int J Oral Maxillofac Surg 38(4): 363-368.
-
Roze J, Babu S, Saffazadeh A, Gayet Delacroix M, Hoomaert A, et al. (2009) Correlating implant stability to bone structure. Clin Oral Implants Res 20(10): 1140- 1145.
-
AlSamak S, Al Hafidh NN, Al Khatib AR (2022) Evaluation of potential mini-implant insertion sites for maxillary skeletal expander: A computerized tomography study. Clinical and Investigative Orthodontics 81(1): 34-42.
-
Wilmes B, Su YY, Drescher D (2008) Insertion angle impact on primary stability of orthodontic mini- implants. Angle Orthod 78(6): 1065-1070.
-
Ozkan S, Bayram M (2016) Comparison of direct and indirect skeletal anchorage systems combined with 2 canine retraction techniques. Am J Orthod Dentofacial Orthop 150(5): 763-770.
-
Ren Y (2009) Mini-implants for direct or indirect orthodontic anchorage. Evid Based Dent 10(4): 113.
-
Ozsoy PO, Ozcirpici AA, Veziroglu F (2009) Miniscrews for upper incisor intrusion. Eur J Orthod 31(4): 412-416.
-
Papadopoulos MA, Papageorgiou SN, Zogakis IP (2011) Clinical effectiveness of orthodontic miniscrew implants: a meta-analysis. J Dent Res 90(8): 969-976.
-
Serra G, Morais LS, Elias CN, Meyers MA, Andrade L, et al. (2010) Sequential bone healing of immediately loaded mini-implants: histomorphometric and fluorescence analysis. Am J Orthod Dentofacial Orthop 137(1): 80-90.
-
Miyawaki S, Koyama I, Inoue M, Mishima K, Sugahara T, et al. (2003) Factors associated with the stability of titanium screws placed in the posterior region for orthodontic anchorage. Am J Orthod Dentofacial Orthop 124(4): 373-378.
-
Lin YD, Wu YK (2015) Factors affecting the stability of mini-implants. Chin J Tissue Eng Res 19(8): 1295-1300.
-
Samrit V, Kharbanda OP, Duggal R, Seith A, Malhotra V (2012) Bone density and miniscrew stability in orthodontic patients. Aust Orthod J 28(2): 204-212.
-
Papageorgiou SN, Zogakis IP, Papadopoulos MA (2012) Failure rates and associated risk factors of orthodontic miniscrew implants: a meta-analysis. Am J Orthod Dentofac Orthop 142(5): 577-595.
-
Chen YJ, Chang HH, Huang CY, Hung HC, Lai EHH, et al. (2007) A retrospective analysis of the failure rate of three different orthodontic skeletal anchorage systems. Clin Oral Implants Res 18(6): 768-775.
-
Motoyoshi M, Hirabayashi M, Uemura M, Shimizu N (2006) Recommended placement torque when tightening an orthodontic mini-implant. Clin Oral Implants Res 17(1): 109-114.
-
Chen YH, Chang HH, Chen YJ, Lee D, Chiang HH, et al. (2008) Root contact during insertion of miniscrews for orthodontic anchorage increases the failure rate: an animal study. Clin Oral Implants Res 19(1): 99-106.
-
Briceno CE, Rossouw PE, Carrillo R, Spears R, Buschang PH (2009) Healing of the roots and surrounding structures after intentional damage with miniscrew implants. Am J Orthod Dentofacial Orthop 135(3): 292- 301.
-
Yu WJ, Kim MR, Park HS, Kyung HM, Kwon OW (2011) Finite element analysis of peri-implant bone stress- induced root contact of orthodontic micro implant. Korean J Orthod 41(1): 6-15.
-
Kuroda S, Tanaka E (2014) Risks and complications of miniscrew anchorage in clinical orthodontics. Japanese dental science review 50(4): 79-85.
-
Mehta S, Wang D, Kuo CL, Mu J, Vich ML, et al. (2021) Long-term effects of mini-screw-assisted rapid palatal expansion on airway. Angle Orthod 91(2): 195-205.
-
Graf S, Vasudavan S, Wilmes B (2018) CAD-CAM design and 3-dimensional printing of mini-implant retained orthodontic appliances. Am J Orthod Dentofacial Orthop 154(6): 877-882.
-
Sari E, Ugar C (2007) Interleukin 1beta levels around microscrew implants during orthodontic tooth movement. Angle Orthod 77(6): 1073-1078.
-
Enhos S, Veli I, Cakmak O, Ucar FI, Alkan A, et al. (2013) OPG and RANKL levels around miniscrew implants during orthodontic tooth movement. Am J Orthod Dentofac Orthop 144(2): 203-209.
-
Kaya FA, Hamamci N, Uysal E, Yokuş B (2011) Identification of tumor necrosis factor-alpha levels around miniscrews during canine distalization. Kor J Orthod 41(1): 36.
-
Qureshi T, Duggal R, Kharbanda OP, Rajeswari MR (2021) Expression of circulating cell-free nucleic acids around miniscrew implant during orthodontic tooth movement-a prospective study. Prog Orthod 22(1): 33.
-
Alassy H, Parachuru P, Wolff L (2019) Peri-Implantitis Diagnosis and Prognosis Using Biomarkers in Peri- Implant Crevicular Fluid: A Narrative Review. Diagnostics (Basel) 9(4): 214.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells