Can the Photobiomodulation Improve Osseointegration? A Literature Review
This study discussed the characteristics of photobiomodulation modalities using low-level laser and light-emitting diodes and their therapeutic effects on post-implant osseointegration, through an integrative literature review. The methodology consists of a guided search in Portuguese and English from 2001 to 2020 through texts in Google Scholar, PubMed and Scielo databases. Results: The technique of osseointegrated implants within implantology has made great advances possible by favoring the restoration of dental function and aesthetics in total and partial edentulous individuals. This type of implant is successful when the phenomenon of osseointegration occurs, a complex process that depends on several local and systemic circumstances for stability and durability of the implant. In this sense, the use of photobiomodulation in Implant Dentistry can promote speed in the osseointegration process and, consequently, establish better conditions in the postoperative period. Final Considerations: Although several authors present satisfactory results in both photobiomodulation modalities, mainly acceleration of the initial phases of osseointegration, more research in this area should be carried out so that this relationship is better clarified.
Introduction
Dentistry seeks to develop new possibilities to improve the process that drives rehabilitation through implants: The process of osseointegration. It is through the improvement of this dynamic and complex process that implants have been used with greater safety and predictability of success [1].
With the advent of osseointegrated implants, the possibilities for oral rehabilitation of both total edentulous patients and partial rehabilitation have increased. This stage is directly related to the osseointegration process. Generally, osseointegration can be described as the integration of the implant surface with the receiving peri-implant tissues [2, 3].
In the current scenario, osseointegrated implants present high success rates and, therefore, several therapeutic modalities have been studied to obtain a greater variety of biological effects on the tissues, such as biostimulation of tissue proliferation and bone cell metabolism that ensure implant survival [2, 4].
Although they have high predictability of success, there are a number of factors that can favor or impair the osseointegration process due to the dynamism of bone formation and the maintenance of periimplant bone. Therefore, knowledge about techniques that can positively influence osseointegration is still the object of study within the academic community [1].
In this sense, as therapeutic modalities that can favor osseointegration and ensure a better prognosis for osseointegrated implants, we can mention low-intensity laser therapy and light-emitting diodes mainly due to their analgesic, anti-inflammatory and granulation tissue and collagen formation effects [3].
The use of technology in tissue biostimulation and light- tissue integration is considered one of the greatest advances in medicine and dentistry, being used in a wide variety of dental processes [5].
Photobiomodulation with low intensity laser has therapeutic applicability by virtue of its monochromatic and coherence properties, and has been widely explored since the 1960s for treating trauma, since the photonic method - the transformation into biochemical energy - induces a cascade of cellular events favoring local microcirculation and protein synthesis or inhibiting cellular activities [6, 7, 8].
According to Garcia, et al. [9], the application of laser in alveolar wounds causes chronological acceleration in the process of bone tissue repair and this speed of wound closure is proportionally related to the number of applications. Furthermore, its effects are also correlated with the parameters used, such as wavelength, applied energy density, irradiated area, distance from the tissue and power [4].
The effects of phototherapy occur when the infrared wavelength interacts with the tissue generating stimuli such as biostimulation of bone tissue, osteoblastic activity, the reduction of inflammatory processes, minimization of pain, speed in the healing process, among others [5].
An alternative to lasers is the light-emitting diode (LED) or also called photo-emitting diode. It is a phototherapeutic modality used since the 1990s to minimize the inflammatory response due to tissue trauma in surgical procedures that undoubtedly establish an intrinsic relationship. The clinical applicability of this artifice is feasible because the light- emitting diode has a longer lifetime compared to other sources, however, may present different effects on tissues compared to LASER [10, 11].
Therefore, phototherapies present good results in the repair and biostimulation of both soft and hard tissues. Bone tissue repair is slower due to its complexity involving local systemic variables, however, photon therapy can considerably decrease post-surgical recovery time and recovery period [12].
Thus, this work conducts an integrative review of the literature to discuss and analyze the use of photobiomodulation and its possible mechanisms of functioning in osteoblasts, as well as to improve the indication of these modalities as a complement to implant dentistry.
Methodology
This work is an integrative literature review whose bibliographic material was obtained through consultation of review papers and/or research published in Portuguese and English from 2000 to 2020 available in the electronic databases Google Scholar, PubMed and Scielo.
To this end, searches were made of references containing the following keywords: bone repair, Photobiomodulation and Osseointegration.
As eligibility criterion articles were included that had an association between photobiomodulation and osseointegration, considering the mechanisms of action on the osteoblasts.
Results and Discussion
Photobiomodulation
A major innovation for implant dentistry that may come to enhance the bone healing process, as well as, improve stability is photobiomodulation, which produces effects at the cellular level [13].
The term photobiomodulation refers to the influence on cellular metabolism resulting from the application of photon energy with red and infrared light in the wavelength range between 600 and 700 nanometers (nm) and between 780 and 1100 nm. There is preference for the wavelength of red light due to its greater ability to penetrate tissues and absorption by chromophores [14].
The first LASER was developed by US physicist Theodore Harold Maiman in 1960 and the origin of the word is the English language acronym “Light Amplification by Stimulated Emission of Radiation,” which translates as “light amplification by stimulated emission of radiation” [15, 16].
Since its creation, low-intensity or non-surgical LASERs have been used for therapeutic purposes in different areas of health, especially in dental procedures. Its wide therapeutic use is linked to the fact that this device presents electromagnetic waves that have monochromaticity that propagate coherently in space and time. It is also possible to verify the wavelength measured between the consecutive peaks of its trajectory that range between 500 and 1200 nm, resulting in non-thermal and biostimulant effects [17, 18].
The monochromaticity characteristic of the LASER refers to the fact that it has photons of the same color and a single wavelength that carries, directionally, high concentrations of energy. Such specificity confers radiation to LASER resulting, therefore, in interactions with biological tissues and therapeutic utility [15, 18].
Coherence in space and time, on the other hand, indicates that its waves propagate in an ordered manner and with the same amplitude, causing the photons to travel to parallel to the tube that generates such energy with a minimum degree of divergence [19].
The main difference between a LASER and LED is the lack of spatial coherence of the LED because it presents light beams that travel divergently, resulting in lower penetration power. The wavelengths of LED vary between 390 and 904 nm, however, photobiomodulation uses only red and infrared lights [9].
Leite, et al. [20] compared the effects of low intensity photobiomodulation (LASER/LED) on the process of alveolar repair in rats. In their study, they used LASER and LED in a sample composed of 45 rats submitted to a protocol of induced injury, in which it was possible to verify a moderate inflammatory process and osteoblastic activity in both resources.
In a study proposed by Stein, et al. [21] to evaluate the effects of photobiomodulation on proliferation osteoblasts in humans, cultured osteoblasts were irradiated using laser irradiation and the effects were quantified by cell counting. A significant increase in the cell count was observed compared with non-irradiated cells.
Both phototherapies stimulate the general metabolism of cells, the generation of energy so that the cell can maintain its activities, protein synthesis, mobility, cell replication, maintenance of membrane potential, improvement in wound healing and nerve regeneration, and mainly, in the induction of bone formation [12].
Such evidence suggests the possibility of irradiation in bone tissue submitted to implants and probable acceleration in the osseointegration processes that must be better elucidated.
Osseointegration and Photobiomodulation
Table 1 systematizes the main results of the studies included in the analysis of the literature review. To table 1, the variables were used: author, type of study, object, methodology, results and conclusion. These variables are of fundamental importance for the study because through them it is possible to assess whether photobiomodulation can improve the process of osseointegration of implants.
| Author and Study | Objective | Methodology | Results | Conclusion |
|---|---|---|---|---|
| Leite, et al. [20] In vivo study | Evaluate the effectiveness of LASER/LED in bone repair in fracture- induced rats. | 45 male rats had induced fractures and were divided into three groups: The infrared LED treatment group with wavelength close to 858 +/- 20 nm, energy of 4 J/cm2 and 120 seconds of irradiation. The LASER treatment group with wavelength close to 830 nm, 4J/cm2 for 120 seconds. And the control group. | Both features (LASER/LED) accelerated the alveolar repair process. | Both resources accelerate the alveolar repair process, as well as a more satisfactory increase of osteoblasts and osteocytes in the injured areas and reduction of the inflammatory process. |
Twelve patients submitted to bimaxillary implant surgery with particulate bone graft. The intervention side was irradiated with LED for 20 minutes, each day and for 10 consecutive days after surgery. Measurements of the implant stability coefficient (ISQ) were taken immediately before surgery, one month and three months after surgery.
Evaluate the effects of photobiomodulation with LED on the stability of dental implants in bone graft Kashefimehr A, et al. [22] Clinical Trial Perform an integrative review of the literature to answer the following question: How does the use of laser aid the process of osseointegration in implantodontia?
Search for scientific articles in pubmed, lilacs and scopus databases indexed from 2016 to 2020.
Santos, et al. [5] Literature review Fifty-six rats were divided into four groups: The first in which the bone defect in the tibia was filled with deproteinized bovine bone graft, the second in which the bone defect was filled with biphasic hydroxyapatite ceramic and β-tricalcium phosphate and the third and fourth groups were filled with the same types of bone graft and submitted to low-intensity LASER therapy 808nm, 100mW of power, in 7 sessions with 48h between irradiations.
Evaluate the osseointegration of implants placed in graft areas with different types of osseoconducting bones submitted to low-intensity infrared LASER irradiation in rats.
De Oliveira GJPL, et al. [23] In vivo study
A randomized controlled clinical trial in twelve patients who were divided into two groups: A group that received implants of an end bone root shape and no LASER irradiation. Group that received low intensity LASER implant and irradiation. Each patient received fifteen sessions of LASER within two weeks of implant placement, and the others every two weeks until six months. Output power of 2 watts, 980 nm wavelengths, 300 hz frequency for 5 minutes was used.
Evaluate the bone changes of the crest around late dental implants submitted to low intensity LASER application compared to implants without LASER irradiation.
Bakry, et al. [24] Clinical Trial
The ISQ value was not modified with LED irradiation immediately after surgery. However, there was a favorable increase after one month.
The LED favors the increase of the ISQ over three months.
Low-power LASER assists in implantodontia about osseointegration of the implant, reducing the postoperative period, pain and inflammation. However, more studies are needed.
There are not enough case studies, especially in humans, to prove the efficacy of LASER in the osseointegration process, although the technique is promising.
The results obtained by biomechanical, microtomographic and histometric methods confirmed that low-intensity LASER therapy induces a higher degree of osseointegration.
Low-power laser therapy performed in areas grafted with osteoconductors before implant placement improves osseointegration.
Under the conditions evaluated, the low intensity LASER had no effect on the implant in terms of success rate.
The results showed no significant difference between the two groups.
A literature review that seeks to highlight the interaction between osteoblast and light in addition to discussing in vitro photobiomodulation therapy for alveolus preservation.
Amaroli, et al. [25] Literary review Searches the PubMed and Scholar database.
Discuss and analyze the therapeutic effects of low- intensity LASER on tissues in post- implanted areas and cover clinical usability protocols.
Searches were conducted from 2000 to 2019 in the Scielo, PubMed, Scholar Google, Medline and Lilacs databases.
Munhoz, et al. [15] Literature Review
The combined effect of LASER and LED was used to evaluate the stify ness of the implants during the healing period. The patients were divided into two groups: Patients who received LASER and LED 20min/day for 10 days, 830 nm laser (15mW/cm2), combined with 632 nm LED (10mW/cm2) in four points around the implant. And patients who did not receive phototherapy. Then measurements of the coefficient of stability of the implant were made.
The study seeks to answer the following question: Can LASER and LED improve the stability of dental implants?
Mohajerani, et al. [26] Clinical Study
Twenty-four patients (8 women and 16 men) underwent implant therapy (resulting in 40 implants) in the posterior region of the mandible. The patients were divided into two groups: Group that received LASER therapy with wavelength of 635 nm, power of 100 mW and average power density of 199.04 mW/cm2 (dose: 4J per point or 8J/cm2), for 40 seconds per point (one vestibular side point and one lingual point of the alveolo/ implant). Total energy per session: 8J. And control group that did not receive irradiation with LASER.
Evaluate bone stability in the peri-implant zone after using low- intensity LASER with wavelength of 635 nm.
Matys, et al. [13] Randomized clinical trial Wavelengths greater than 800 nm and irradiations greater than three applications improve bone repair. The study only suggests better experimental configurations.
Wavelengths greater than 800 nm and irradiations greater than three applications improve bone repair.
The efficacy of low-intensity laser therapy in osseointegration and bone repair are questionable. There are still no universal protocols and studies aimed at regeneration do not present favorable results.
Low-intensity LASER has good results only in the treatment of soft tissues and therapeutic procedures.
Simultaneous use of LASER and LED increases implant stability after 9 weeks.
The combined use of LASER and LED increases implant stability.
The use of LASER with 635 nm in periimplant soft tissue improves implant instability and increases the value of the bone density scale after 12 weeks at the mid and apical level of the implant.
Based on this study, there was an improvement in the stability of the secondary implant through the use of the 635 nm LASER.
Evaluate the influence of photobiomodulation using low-intensity LASER and LED on bone tissue and mucous cells grown in machined titanium discs.
Human cell lines of osteoblasts, fibroblasts and epithelial cells were used and submitted to 3 irradiations within 24 hours. The LASER with wavelength of 780 nm and power of 25 mW. And the LED with 810 nm wavelength and 20 mW of power.
Rech [4] In vitro study
Conduct a literature review on the use of photobiomodulation in the process of bone tissue repair.
Casalechi VL, et al. [12] Literature review Use of bibliographic material obtained through visits to Bireme databases.
Evaluate studies correlating photobiomodulation and regeneration to evaluate the parameters that produce positive results based on the dose and power used.
The Search bases PubMed, Springer, Google Scholar and Cochrane were used and 230 articles were evaluated, of which only 19 articles met the inclusion criteria.
Zein, et al. [14] Literature Review
Twenty rabbits received 40 implants in the medial part of the right and left tibias, one implant of each surface in each tibia. These animals were divided into two groups: Animals that received irradiation with low-intensity LASER and animals that did not. The infrared LASER was applied with a wavelength of 880 nm, a power of 100 mw, a dose of 8.7 J/ cm2 for 25 seconds for an area of 1 cm2.
Evaluate the effects of low-intensity LASER on the osseointegration process of implants with different surfaces.
Jesus [27] In vivo study
Epithelial cell adhering was significantly affected by photobiomodulation.
Photobiomodulation can improve cellular functions related to the periimplant repair process.
There are few studies on the effects of photobiomodulation on bone repair. But most studies suggest that photobiomodulation minimizes pain and bone repair time.
Photobiomodulation has shown good results in hard tissue repair.
Photobiomodulation with low-power LASER increases cell metabolism, DNA synthesis and RNA, leading to bone neoformation and absorption, increasing osseointegration. There is no fixed dose that produces such answers.
There is a relationship between dose and potency in the positive effects caused by low-intensity LASER therapy on osseointegration.
The low-intensity LASER accelerated the early stages of the osseointegration process allowing for higher removal torque values.
The low-intensity LASER showed positive effects in the process of osseointegration of rabbits.
Evaluate the systemic effects of low- intensity LASER in the bone repair process of critical defects created in the tibia of rabbits and filled with the lyophilized bone of bovine origin and covered with a collagen membrane.
Critical size defects were produced in the left tibia of twenty rabbits. These defects were filled with the sintered lyophilized bone of bovine origin and coated with a collagen membrane. The experimental group received low-intensity LASER therapy with an infrared diode, 830nm, at a dose of 10J/cm2, power of mW. Adding a total of 7 applications with an interval of 48 hours.
Bergamaschi IP [16] In vivo study
Twelve patients (6 men and 6 women) underwent implant therapy for bilateral reconstruction in the posterior region of the maxilla. After surgery, one side was randomly chosen to receive low-level LASER treatment and the other was a placebo. The LASER used with wavelength equal to 637 nm, power of 40 mW and continuous wave. The total irradiation dose per treatment was 6.26 J/cm2.
Investigate the influence of low- level LASER on osseointegration and early success of implants placed in low density bones.
Mandić B, et al. [17] Clinical study Eight dogs underwent therapy with implants in mandibular bone defects filled with nanoemulsion, liposome, blood clot and autogenous bone. In this study, infrared LED at wavelength equal to 830 nm, dose of 1.5J, power of 60 mW and irradiation time of 2 minutes and visible light with wavelength equal to 633 nm, dose of 3J, power equal to 58 mW for 3 minutes and 45 seconds of irradiation were used. Visible and infrared light was irradiated after 48/72 hours postoperatively in four dogs and 96/120 hours in four dogs.
To evaluate the effects of photosensitive drugs activated by LED on the osseointegration of implants through histometric and histological studies carried out in dogs.
Faria PEP, et al. [28] In vivo study
Contribute to better indication of the applicability of laser therapy in implantodontics Silva, et al. [3] Literature review Search for different studies that deal with the theme.
No systemic effects of LASER therapy were observed in the bone repair process.
Low-intensity LASER therapy did not effect the bone repair process.
Low-intensity laser therapy did not express significant influence on the osseointegration of self-screwimplants placed in low density bone of the posterior maxilla.
In the first week there was no significant influence of LASER on the osseointegration of implants.
Liposome and nanoemulsion with 72/96 hour LED application resulted in greater bone formation than the clot alone, but this process was not sustained in subsequent periods. Bone neoformation was higher with the photobiomodulation after 48/72 hours.
The use of photosensitive drugs activated by LED tended to bone formation, similar to the autogenous bone graft at the later time.
More research needs to be conducted to standardize protocols that support the relationship of laser therapy and osseointegration in Implantodontia.
There is no consensus on the protocol for the use of low- intensity Laser in the literature.
Fifteen partial edentulous patients were submitted to implant therapy and randomly divided into two groups: LED-treated group (8 patients, 10 implants) and the control group (7 patients, 12 implants). In the LED group, a wavelength of 626 nm was used, applied for 20 seconds, a total power of 185 mW, a total energy of 222J over the surgical area. The LED was applied 3 times a week for 3 weeks in the postoperative period.
Determine the effects of LED photobiomodulation on implant osseointegration.
Gokmenoglu C, et al. [29] Clinical trial Outline several studies in which photobiomodulation shows efficacy in the process of osseointegration of implants in animal models.
Search for different studies on photobiomodulation and implants with animal models in PubMed with dates until April 2013. A total of 71 accesses were obtained.
Tang E Gold [30] Literature Review
Twelve ewes were submitted to bilateral elevation of the maxillary sinus with spongy bone of iliac crest. The implant sites were irradiated intraoperatively and in the first postoperative week with 680 nm wavelength, 75 mW of total power a density of 3-4J/cm2.
Determine whether low-power LASER treatment improves bone regeneration and implant osseointegration.
Jakse, et. al. [31] In vivo study
Osteoblast cells were irradiated with LASER with a wavelength of 632 nm, it was applied on days 2 and 3 after seeding 3 seconds – up to a power density of 180 mW/cm2 - that corresponds to 0.14, 0.43, and 1.43 J/cm2 energy density. And the effects were measured by cell count compared with non-irradiated cells.
Investigate the effect of low-power LASER on the proliferation and differentiation of human osteoblast cells.
Stein, et al. [21] In vitro study
Two titanium implants were placed in thirty rabbits that were divided into 3 groups: two tests and one control. Of the test groups, one received laser irradiation emitted in the infrared band of 830 nm and the other in the range of 680nm, with an intensity of 4J/cm2.
The LED favors the stability of the implant during the evaluated period. The study suggests that LED has effects on the tissues around the implant.
Photobiomodulation with LED in the surgical area has beneficial effects on the osseointegration process and on implant stability.
Through this review it is possible to observe positive results of photobiomodulation to improve osseointegration and stability of implants in animal models.
The photobiomodulation improves osseointegration in animal models.
There was no confirmation of improvement in bone regeneration within a spongy sinus graft. However, there was a positive effect on the osseointegration of the implants.
The experiment confirms the results proposed by other authors that low- intensity LASER has a positive impact on implant osseointegration.
LASER increases the proliferation of human osteoblasts in vitro and thereby improves human bone repair.
Low-intensity LASER promotes the proliferation of and maturation of human osteoblasts in vitro.
There was a significant difference after the 6 weeks when compared to the control group.
Laser irradiation of wavelengths of 680 nm and 830 nm improved the degree of osseointegration.
Based on the data obtained, the authors reveal that osseointegrated implants have become a widely used technique with great possibility of success in clinical reality for treating partial and total edentulism [2, 33]. However, several factors influence the dental implant success which can be highlighted as bone quality, the techniques used, post-
| Blay A [32] In vivo study | Evaluate the effects of low-intensity LASER radiation on the mechanism of osseointegration of implants. | Two titanium implants were placed in thirty rabbits that were divided into 3 groups: two tests and one control. Of the test groups, one received laser irradiation emitted in the infrared band of 830 nm and the other in the range of 680nm, with an intensity of 4J/cm2. | There was a significant difference after the 6 weeks when compared to the control group. | Laser irradiation of wavelengths of 680 nm and 830 nm improved the degree of osseointegration. |
Table 2: Selected articles on the influence of photobiomodulation on osseointegration.
surgical care, material used, implant design, osseointegration, surface treatment and occlusal load [32].
A fundamental issue among these factors is osseointegration, that is, the functional adaptation between the living bone and the implant surface. This connection is essential because of the stability provided to the implant and is therefore the main factor influencing the load support and longevity of the procedure [34].
The integration between the alveolar bone and the implant surface, as well as the biological fixation and the implant-directed remodeling, are highly complex processes. And low-intensity laser therapy shows improvement in the quality and speed of this complex interaction between biomaterials and biocompatibility [33].
Importantly, photobiomodulation can be performed at the time of implant placement, as well as, during patient rehabilitation follow-up appointments to promote treatment success [30].
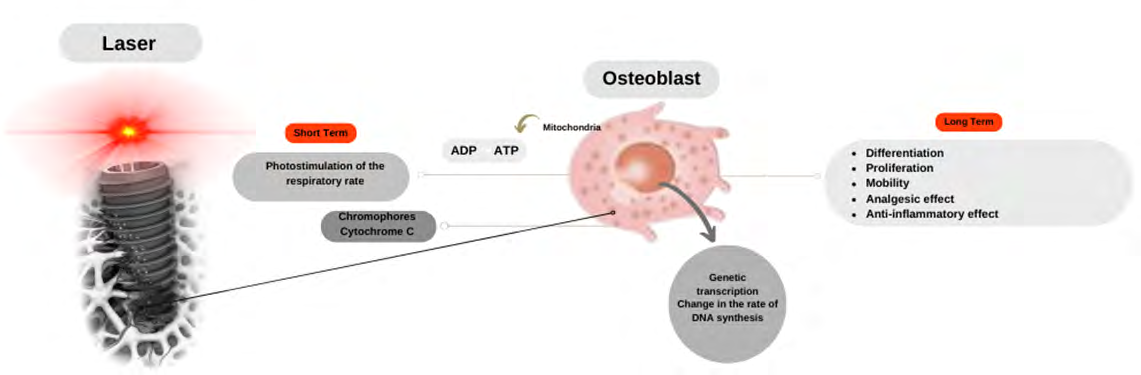
In LASER photobiomodulation, light is absorbed by chromophores, in particular cytochrome C, a photosensitive structure present in mitochondria and part of cellular respiration. By absorbing the light, it is transformed into energy. With the stimulation of mitochondrial photoreceptors for ATP synthesis, a biostimulatory effect occurs in bone tissue causing increase and proliferation of osteoblasts [12, 13] (Figure 1).
When it comes to the therapeutic effects obtained by applying LED in surgical areas, it is also possible to verify positive manifestations in the osseointegration process that ensure implant stability, greater contact between surfaces, proliferation and maturation of osteoblasts [29].
It is assumed that the vascular response to laser therapy is one of the reasons for obtaining the favorable cases of osseointegration present in the literature, since local blood flow and neovascularization are determining factors for osteogenesis [35].
In a study by Faria, et al. [28] to evaluate the effects of the photodynamic process on implant osseointegration in dogs, the animals underwent implant therapy. Bone defects were filled with nanoemulsion, liposome, blood clot and autogenous bone, and postoperatively were irradiated with LED in visible infrared light. It was observed that a significant bone formation occurred, similar to autogenous bone grafting.
In a study in which sheep underwent a bilateral maxillary sinus floor elevation procedure with cancellous bone from the iliac crest, Jakse, et al. [31] evaluated the influence of low-power laser treatment on bone regeneration and osseointegration of dental implants after sinus augmentation. Although laser therapy did not show effects on bone regeneration within the cancellous sinus graft, it was confirmed that there were positive effects on implant osseointegration after sinus augmentation.
Gokmenoglu, et al. [29] conducted a study to determine the effect of LED photobiomodulation in implant osseointegration by measuring implant stability by resonance frequency analysis, interleukin-1b, transforming growth factor-b, prostaglandin-E2 and nitric oxide levels in the periimplant crevicular fluid in 15 patients (8 from the control group and 7 from the LED group). The LED used had a wavelength equal to 626 nm. It was concluded that the application of LED in the surgical area brought beneficial effects in the osseointegration process and the implant stability was maintained.
In studies with rabbits, Jesus [27] evaluated the effects of low-intensity laser on the osseointegration process of implants with different surfaces in each tibia, randomly distributed. In view of the results, it was found that LASER accelerated the initial phases of osseointegration compared with non-irradiated implants.
Rech [4], in a study, evaluated the influence of the application of photobiomodulation using low-intensity LASER and LED on human cell lines of osteoblasts, fibroblasts and epithelial cells cultured on machined titanium disc. For the LASER, a wavelength of 780 nm was used, while for the LED light, a wavelength of 810 nm was applied. It was found that there was a positive influence of LASER and LED on viability, total protein synthesis and collagen in different ways in each cell type.
Subsequently, to evaluate implant stability (primary and secondary) and bone density in the peri-implant zone after protocol with low-intensity laser in 24 patients (8 women and 16 men), Matys, et al. [13] used 635 nm laser with irradiation on the buccal and lingual side of the alveolus/ implant. The conclusion obtained through this study was that there was improvement in secondary implant stability and bone density.
A little further on, to evaluate the effects of low-intensity laser therapy on the osseointegration of implants placed in grafted areas in rats, De Oliveira, et al. [23] filled bone defects made in the tibia with deproteinized bovine bone graft, biphasic hydroxyapatite ceramic and β-tricalcium phosphate. The aforementioned areas were treated with low-intensity laser irradiation. It was verified that the areas grafted with osteoconductive bone substitutes, before implant placement, reacted positively to osseointegration.
In the same year, Sampaio [36] evaluated the stability of osseointegrated implants in alveoli with and without the application of photobiomodulation therapy. For this, 20 patients requiring extraction in bilateral lower molars were selected and one group received photobiomodulation therapy immediately after surgery. After 45 days of exodontia, implants were installed and primary stability was evaluated using a device called Osstell ISQ. However, it was concluded that there were no statistically significant effects in the ISQ stability evaluation.
Although studies on photobiomodulation are advancing over time, it is possible to verify that its applications, in both LASER and LED modalities - and in a large majority - result in improvement of cellular functions of peri-implant tissues, although their responses are distinct depending on the type of light applied, wavelength and the cell type considered [4].
Clinical Applications
The parameters used in photobiomodulation applications are of fundamental importance in obtaining the expected results. Amaroli, et al. [25] analyzes the effects of LASER photobiomodulation on bone repair. This study concluded that the use of appropriate parameters favors osteoproliferation and osteoinduction in animals and humans. It was established that wavelengths greater than 800 nm and irradiations greater than three applications improve bone repair. In this study, it was also possible to verify that, in healthy rats, the wavelength of 980 nm 0.01 W, 13.95 J/cm2 (60s) and 904/910 nm, 0.2 W, 43.8 J/cm2 (60s) positively affected osteoblastic differentiation markers, as well as bone mineralization. In diabetic rats, using a wavelength of 980 nm and the same parameters described previously, there was also improvement in alveolar bone healing and calcification.
This proposition is confirmed in the subsequent study propose by De Oliveira, et al. [22] that evaluated the osseointegration of implants placed in graft areas with different types of osseoconducting bones submitted to low- intensity in healthy rats. In this study, they used wavelength of 808 nm, 100mW, during 7 sessions with 48 hours of interval between irradiations. Osseointegration and bone repair were evaluated by biomechanical, microtomographic, histometric and immunohistochemistry analyses. It was found that the low-level laser induced a higher degree of osseointegration.
Due to the absence of the Havers System in rats and the accelerated cure rate of rabbits – although they have Havers System – the protocols used in these experimental models offer broad parameters, but should not be used in clinical situations in humans. The model with dogs has human dentoalveolar similarities and may present a more realistic analysis for clinical context [25]. The parameters used by Faria, et al. [27] in the use of LED to evaluate the effects of the photodynamic process on implant osseointegration in dogs were infrared LED of 830 nm, dose of 1.5J, power of 60mW for 2 minutes within 48/72 hours. And visible LED, 633 nm, 3J dose, power of 58mW and time of 3 minutes and 45 seconds. In the interval of 96/120 hours after surgery, infrared LED, power 1.5W, was used for 2 minutes. And 120 hours later visible LED with power of 58mW and 3 minutes and 45 seconds. Thus, it was observed the new bone formation was greater when it used photobiostimulation after 48/72 hours.
The stability of the dental implant is correlated with the success of the osseointegration process. Therefore, many recent studies in human models have focused on evaluating implant stability and marginal bone changes around implants to relate the effectiveness of low-level LASER and LED with these events. Certainly, understanding the effects of photobiomodulation on bone remodeling is a crucial factor in whether LASER therapy can improve bone-implant interaction [24, 26, 37].
Mohajerani, et al. [26], for example, to evaluate the effects of the combined use of low-intensity LASER and LED on the stability of dental implants, LASER and LED irradiations were performed for ten days and then compared with patients in the control group who did not receive light therapy. The parameters used for the LASER was 830 nm wavelength (15mW/cm2), 10mW of power. Combined with 632 nm LED (10mW/cm2) at four points around the implant for 20 minutes a day for 10 days. The results show that the simultaneous use of the two photobiomodulation modalities increases the stability of the implants.
Matys, et al. [13], to evaluate the stability of laser- irradiated implants using wavelength of 635 nm, power of 100 mW and average power density of 199.04 mW/cm2 (dose: 4J per point or 8J/cm2) in soft tissue, for 40 seconds per point. It was possible to verify improvement in implant ability and increase the value of bone density scale after 12 weeks at the middle and apical level of the implant.
In order to verify the efficacy of laser therapy in the osseointegration of dental implants, Bilge, et al. [37] submitted symmetrical edentulous patients in the mandible and maxilla to implant therapy. The implants were divided into laser group and control. The parameters used in this study were wavelength of 940 nm (total power of 200 mW, average power intensity of 250 mW/cm2, total energy of 40 J, mean energy intensity of 50 J/cm2). Six sessions were performed with LASER during two months. Subsequently, the stability of the implants was measured at baseline at 14, 30 and 90 days. It was concluded that laser therapy was effective and successful in the process of osseointegration of the implant. There was an increase in implant stability after six sessions of low-level LASER.
In a similar study, proposed by Torkzaban, et al. [38] to evaluate the efficacy of low-level LASER in dental implant stability, 19 patients were randomly divided into laser and control groups. The parameters used were wavelength of 940 nm, 100 mW output power, spot area 0.2826 cm2 and average power density (irradiance) of 354.6 mW/cm2 in continuous wave mode. LASER was irradiated by tissue in contact with mucosa for 40 seconds (14.18J/cm2). Energy was 4J at each side and total 8J per session. LASER irradiation was repeated at 2, 4, 6, 8, 10 and 12 days (56 J total). However, it was observed that within 2 weeks after implant placement, laser with a wavelength of 940 nm had no significant effects on implant stability. It is important to note that they made use of irradiance of 354.6mW/cm2, however the recommended values for stimulation and cure range from 5 to 50mW/cm2 [39].
Therefore, based on the positive results with animals observed in this study, it can be considered that there is a relationship between the acceleration of osseointegration and bone repair aided by low-level laser. Due to the wide variety of parameters studied over time (power, fluency, exposure time, exposure frequency and wavelength) it is verified that there are numerous possibilities of successes that must be studied continuously.
In the studies presented with partial edentulous patients, we know that there are several factors that can affect the dosimetry of low-level laser and LED, one of which is the depth of the target tissue and the wavelength. In that case, appropriate wavelength and intensity will influence the success of osseointegration. Theoretically, wavelengths close to 800 nm will have better tissue penetration of about 1 cm, while wavelengths close to 600 nm penetrate about 0.5 cm. Wavelengths in the range of 800-980 nm have higher penetration capacity. In fact, in studies with in vivo animals, it was verified that wavelength close to 800nm is more effective, although the parameters vary widely [25, 35, 40, 41, 42].
Unfortunately, as carefully detailed by Tunér and Jenkins [41], the parameters used in many studies are flawed because they do not present accuracy, detail and, on several occasions, it does not replicate knowledge from previous studies. Among the major problems, the lack of energy parameters (J) and dose (J/cm²) is found, which are often not even mentioned.
Jenkins and Carroll [43] proposed a complete report of technical and treatment parameters in tabular format as a way to standardize the informative content of published studies on photobiomodulation. The authors highlight the need to provide the specifications of the equipment, as well as its tolerances, the complete description of the equipment, calibration conditions and the methodology of the tests, the justification for the dosages chosen, the general conditions of the patient, target tissue, pathology and etiology presented.
It is evident that the use of photobiomodulation to optimize osseointegration as an applicable clinical therapy depends on the detailing of the parameters used by the authors. With greater accuracy in the description of the parameters, it would be possible to apply the benefits of photobiomodulation therapy, rather than just proving its promising evidence without definitive conclusions.
Conclusion
This study allows several authors to positively evaluate the use of photobiomodulation, especially low-level LASER. Therefore, there be evidence of acceleration of osteoblast proliferation and, consequently, of the osseointegration process in animal models. These studies also provide evidence that photobiomodulation may improve implant healing and long-term stability. However, it is essential that further research be conducted with humans for this relationship to be better clarified, given that the human biological structure is more complex and differentiated compared with animals.
It is also necessary to standardize protocols to ensure the efficacy and safety of the clinical use of photobiomodulation for improving osseointegrated implants. The inefficacy of photobiomodulation reported in some studies may be related to the protocols and experimental models used. Possibly, the use of this powerful artifice in implant dentistry will show promising results in the future.
References
-
Lucas RRS (2013) Fatores que afetam a osseointegração dos implantes–uma revisão. Revista Fluminense de Odontologia pp: 39.
-
Sartori I (2015) Oral rehabilitations with osseointegrated implants in cases of greater complexity. Nova Odessa: Napoleão.
-
Furtado SD, Barbosa CV, De Albuquerque, Lira AC (2014) Application of Laser Therapy in Implant Dentistry. Revista Saúde Ciência 3(2): 58-68.
-
Alberto RC (2018) Effects of photobiomodulation on adhesion and metabolism of osteoblasts, fibroblasts and epithelial cells on titanium surfaces in vitro.
-
Leão SAL, Novaes RCC, Silva EGA, Melo EL, Gerbi MEM (2021) Laser in implant dentistry: integrative review. Research Society and Development 10(3): e31310313322-e31310313322.
-
Vieira CA (2005) Comparative photobiomodulation between laser and low intensity LED in the angiogenesis of cutaneous wounds in rats. Tese de Doutorado. Master’s Dissertation, Engineering School of São Carlos.
-
Smith KC (1991) The photobiological basis of low-level laser radiation therapy. Laser Therapy 3(1): 19-24.
-
Frare JC, Nicolau RA (2008) Análise clínica do efeito da fotobiomodulação laser (GaAs-904 nm) sobre a disfunção temporomandibular. Brazilian Journal of Physical Therapy 12(1): 37-42.
-
Garcia GV (2000) Influence of the number of applications of biostimulation laser beam on the repair of dental extraction wounds. Histological study in rats. Rev Fac Odontol Lins 12(1): 29-37.
-
Comunian CR (2013) Fotobiomodulação com led e laser no reparo de alvéolo mandibular de coelhos (Oryctolagus cuniculus).
-
Rodrigues F (2014) Histological Analysis of Alveolar Bone Repair in Wistar Rats Subjected to Photodynamic Therapy.
-
Casalechi VL (2018) The use of photobiomodulation in bone repair (literature review). XI Latin American Initiation Meeting.
-
Matys J, Świder K, Grzech Leśniak K, Dominiak M, Romeo U (2019) Photobiomodulation by a 635nm diode laser on peri-implant bone: primary and secondary stability and bone density analysis-a randomized clinical trial. BioMed Res Int.
-
Randa Z, Wayne S, Stefano B (2017) Effect of low- level laser therapy on bone regeneration during osseointegration and bone graft. Photomed Laser Surg 35(12): 649-658.
-
Munhoz STFC, De Sirqueira, Vergeth GLC, De Macedo, Cavalcanti LF (2019) Effect of low power infrared laser on post-implant osseointegration: a literature review. Acervo Saúde Electronic Journal 28: e1036-e1036.
-
Bergamaschi IP (2016) Evaluation of the systemic effect of low intensity laser on the bone repair process with biomaterials: study in rabbits.
-
Mandic B, Lazic Z, Markovic A, Mandic B, Mandic M, et al. (2015) Influence of postoperative low-level laser therapy on the osseointegration of self-tapping implants in the posterior maxilla: a 6-week split-mouth clinical study. Vojnosanit Pregl 72(3): 233-240.
-
Thyrso CF, Marcelo VN, Denise ZM (2003) Evaluation of the action of low intensity laser radiation in the osseointegration process of titanium implants inserted in rabbit tibia. Implantnews magazine.
-
Becher RC (2014) Effect of laser or led photobiomodulation on bone formation after disjunction of the median palatal suture.
-
Leite MKM, Silva AC, Costa EKO, Silva FTA, Lopes AMA, et al. (2022) Comparação dos efeitos da fototerapia de baixa intensidade (laser/led) no processo de reparo ósseo experimentalmente induzido em ratos. Revista Eletrônica Acervo Saúde 15(4): e9665-e9665.
-
Stein A, Benayahu D, Maltz L, Oron U (2005) Low- level laser irradiation promotes proliferation and differentiation of human osteoblasts in vitro. Photomed Laser Surg 23(2): 161-166.
-
Kashefimehr A, Rahbar M, Faramarzi M, Babaloo A, Sadighi M, et al. (2021) Effect of Light Emitting Diode Photobiomodulation on the Stability of Dental Implants in Bone Grafted Cases: a Split-Mouth Randomized Clinical Trial. Maedica 16(2): 223-229.
-
De Oliveira GJPL, Aroni MAT, Pinotti FE, Marcantonio E, Marcantonio RAC (2020) Low-level laser therapy (LLLT) in sites grafted with osteoconductive bone substitutes improves osseointegration. Lasers in Medical Science 35(7): 1519-1529.
-
Bakry SA, Kamel HM, Awad S (2020) Evaluation of crestal bone changes around delayed implant in response to diode laser thearapy: a randomized controlled clinical trial. Egyptian Dental Journal, (Oral Surgery) 66(2): 841- 851.
-
Amaroli A, Colombo E, Zekiy A, Aicardi S, Benedicenti S (2020) Interaction between laser light and osteoblasts: photobiomodulation as a trend in the management of socket bone preservation-a review. Biology 9(11): 409.
-
Mohajerani H, Salehi AM, Tabeie F, Shafiei S, Tabrizi R (2020) Can low-level laser and light-emitting diode enhance the stability of dental implants?. J Maxillofac Oral Surg 19(2): 302-306.
-
Jesus LK (2017) Evaluation of the effects of low intensity laser on osseointegration of implants with different surfaces: analysis by resonance frequency and biomechanics.
-
Faria PEP, Felipucci DNB, Simioni AR, Primo FL, Tedesco AC, et al. (2015) Effects of photodynamic process (PDP) in implant osseointegration: a histologic and histometric study in dogs. Clinical implant dentistry and related research 17(5): 879-890.
-
Gokmenoglu C, Ozmeric N, Erguder I, Elgun S (2014) The effect of light-emitting diode photobiomodulation on implant stability and biochemical markers in peri- implant crevicular fluid. Photomed Laser Surg 32(3): 138-145.
-
Tang E, Arany P (2013) Photobiomodulation and implants: implications for dentistry. J Periodontal Implant Sci 43(6): 262-268.
-
Jakse N, Payer M, Tangl S, Berghold A, Kirmeier R, et al. (2007) Influence of low-level laser treatment on boné regeneration and osseointegration of dental implants following sinus augmentation: an experimental study on sheep. Clin Oral Implants Res 18(4): 517-524.
-
Blay A (2001) Effects of low intensity laser radiation on the mechanism of implant osseointegration: an _in_ _vivo study_, 135 f. Course Conclusion Paper (Master’s Dissertation). Instituto de Pesquisas Energéticas Nucleares, Autarquia Associada à Universidade de São Paulo, São Paulo.
-
De Oliveira, Afonso F (2019) Biomechanical analysis of osseointegration of implants with hydrophilic surface compared to implants with hydrophobic surface. Study in rats. Revista de Odontologia da UNESP, Especial, pp: 47.
-
Parithimarkalaignan S, Padmanabhan TV (2013) Osseointegration: an update. J Indian Prosthodont Soc 13(1): 2-6.
-
Freitas PM, Simoes A (2015) Lasers in dentistry: guide for clinical practice. John Wiley & Sons.
-
Freire SRM (2021) Avaliação da estabilidade de implantes osseointegrados em alvéolos, com e sem a aplicação da Terapia de Fotobiomodulação, por meio de Osstell® ISQ: ensaio clínico, duplo cego e randomizado Tese de Doutorado. Universidade de São Paulo.
-
Bilge S, Bayindir S, Demirbas A, Soylu E (2021) Efficacy of diode laser therapy on osseointegration of dental implants: A split-mouth clinical study.
-
Torkzaban P, Kasraei S, Torabi S, Farhadian M (2018) Low-level laser therapy with 940 nm diode laser on stability of dental implants: a randomized controlled clinical trial. Lasers Med Sci 33(2): 287-293.
-
Zayed SM, Hakim AAA (2020) Clinical efficacy of photobiomodulation on dental implant osseointegration: A systematic review. Saudi J Med Med Sci 8(2): 80-86.
-
Allison RR, Sibata CH (2010) Oncologic photodynamic therapy photosensitizers: a clinical review. Photodiagnosis Photodyn Ther 7(2): 61-75.
-
Tuner J, Jenkins PA (2016) Parameter reproducibility in photobiomodulation. Photomed Laser Surg 34(3): 91-
-
Uzunov TZ, Uzunova P, Angelov I, Gisbrecht A (2008) Comparative investigation of the penetration of different wavelength visible LED radiation into dental tissue. In: 15th International School on Quantum Electronics: Laser Physics and Applications. SPIE pp: 415-420.
-
Jenkins PA, Carroll JD (2011) How to report low-level laser therapy (LLLT)/photomedicine dose and beam parameters in clinical and laboratory studies. Photomed Laser Surg 29(12): 785-787.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells