A Pilot Study: The Effectiveness of Augmenting Alveolar Bone Defects with Bone Marrow Aspirate Impregnated Allogeneic Graft
Purpose: The purpose of this pilot study was to evaluate the effectiveness of bone marrow aspirate impregnated allogeneic graft as compared with autogenous bone grafting in inducing adequate bone for endosseous dental implants. Materials and Methods: Sixteen patients with alveolar bone defects secondary to trauma, pathology or infection were augmented with bone marrow aspirate impregnated allogeneic bone. Bone induction was assessed by alveolar ridge height and width using cone beam CT obtained before and 4 months after treatment as compared to published controls using autogenous harvesting sites. Results: Mean increases in alveolar ridge height at 4 months after treatment were similar to established controls using traditional autogenous harvesting sites: 3.9 mm and 3.8 respectively. Mean increases in alveolar ridge width (buccal to lingual) at the crest of the ridge were similar between both autogenous, allogeneic and bone marrow aspirate groups: 4.33, 4.56 and 3.97 respectively. Seven of the 10 patients have received dental implants which have remained osseointegrated at least 1 year post-implantation. In addition, subject undergoing BMA harvest had VAS scores of one 1 week after harvest as compared to a VAS of 5.5 in published controls using traditional anterior iliac bone harvest. Also only 9% of subjects reported any pain 1 week after BMA harvest versus 15% and 70% in published controls using the proximal tibia as a harvest site. Conclusion: This study is the first pilot study using BMA impregnated allogeneic bone to augment alveolar bone defects as an adequate source of bone for functional loading of endosseous dental implants as compared to more traditional forms of grafting.
Introduction
Alveolar bone deficiency due to tooth loss, trauma, or maxillofacial neoplasms can compromise the ability to restore form and function of the patient’s dentition. Historically, bone loss is primarily treated by bone grafting techniques. Autogenous bone has always been considered the “gold standard” of all bone grafting techniques, despite the need for a donor site with its potential complications, increased cost and possible hospital stay. To avoid donor site morbidity, other grafting materials have also been used such as allograft, xenograft and alloplasts, serving only as a scaffold requiring osteoblasts and soluble factors to regenerate bone. Recently, soluble factors such as bone morphogenetic proteins (BMP’s) have been studied with success in limited conditions, but cost and some concerning adverse effects are the major factors in providing this option [1, 2]. A viable alternative to these procedures is the use of autogenous stem cells to develop a safer, less costly system for bone regeneration. Bone marrow aspirate (BMA) is a rich source for mesenchymal stems cells that can differentiate into osteoblasts and produce bone.
Use of this technique has been reported in the orthopedic literature to treat non-union of tibia fractures, simple bone cysts in long bones, spinal arthrodesis and thoracolumbar fractures. Bone-marrow injection is as effective in regenerating bone as open autologous grafting with fewer disadvantages [3]. When BMA is added to an osteoconductive matrix to treat simple bone cysts, it was shown to be safe and effective in healing the bony defect [4, 5]. There have also been a few case reports using BMA in continuity defects in mandibles. In one case, a patient originally treated with rhBMP-2 failed to heal and therefore opted for retreatment with the addition of BMA, which resulted in complete healing of the defect [6]. In animal studies, the use of mesenchymal stem cells has shown some promise. One study created standardized bone defects in minipigs and randomly grafted with autogenous mandibular bone, an alloplastic scaffold, platelet rich plasma (PRP) + scaffold or mesenchymal stem cells (MSC) + PRP + scaffold. Their results showed a significantly higher percentage of bony contact to graft particles as compared to the PRP-scaffold and scaffold alone, which suggest that the addition of mesenchymal stem cells enhance bone formation [7].
In recent dental literature, mesenchymal stem cells were used to augment maxillary sinus floors in patients with atrophic posterior maxillae [8]. One report had 6 consecutively treated patients using cultured MSCs in combination with biphasic hydroxyl apatite/β-tricalcium phosphate (HA/TCP) to augment the sinus floor. At time of implant placement, histologic evaluation of core biopsies revealed a mean bone regeneration of 41.34% and all implants were considered clinically osseointegrated after 4 months. Another study used split-mouth design augmenting sinus floors with BioOss and bone marrow concentrate and examining implant survival 3 months after placement and after functional loading. Their results show a 3 month survival rate of 91% in the treated side as compared to 100% in BioOss controls. Also no implants were loss after 1 year of functional loading. Both of these papers demonstrate that mesenchymal cells whether cultured or via bone marrow aspirate are a viable option in augmenting posterior maxillary atrophy [9]. In addition, the BioOss study also shows that BioOss alone is just as effective when used in the maxillary sinus augmentation. In contrast, there have not been any prospective studies using mesenchymal stem cells in any form to augment lateral alveolar defects. Our study is the first to examine the use of autologous BMA to induce adequate bone in lateral defects for the placement of endosseous dental implants as compared to gold standard autogenous bone graft.
Patients and Methods
The data for this institutional review board–approved, pilot were collected from patients enrolled from 2011 through 2013 at a single academic clinical center, Harbor- UCLA Medical Center Oral and Maxillofacial Surgery Division. Subjects were recruited by advertisements in the several county of Los Angeles outpatient dental clinics and informally by word of mouth. Inclusion Criteria for the pilot study were subjects at least 18y.o. with inadequate bone for implant restoration (less than 6mm bone height and width), if subject has more than one deficient site only one site will be used in the study, bone loss due to trauma, pathology or localized, periodontal defects (due to malposed/partially impacted teeth) and patients who need bone and will be restored with overdentures. Exclusion criteria included patients with continuity defect, defects requiring both an alveolar and sinus graft, previous failed augmentation procedures, current pathology in the region, significant/ untreated: periodontal disease, caries infection or chronic inflammation of the oral cavity within 2 adjacent tooth of the study treatment area, uncontrolled diabetes, pregnancy/ lactation, medications/diseases and treatments known to affect bone turnover and history of documented allergy to any of the study components. At baseline evaluation informed consent, medical and dental history, pregnancy test, dental exam, periapical and panoramic radiograph, dental impressions and cone-beam CT was obtained.
Surgical Technique
Onlay Bone Graft Procedure: A Modified Lip-Switch technique was to place the graft. An alveolar crestal incision, maxillary or mandibular vestibular incision was made and a mucoperiosteal flap was raised. The recipient site was delineated and decorticated using a rotary instrument. The study treatment (bone marrow aspirate impregnated allogeneic bone) was placed onto the recipient site and stabilized using titanium bone screws.
Bone Marrow Aspiration Procedure: The border of the anterior iliac was palpated orienting the planned puncture site. The skin was stretched between 2 fingers over the crest in order to identify the thickness. The anatomy and planned puncture site outlined. The site was prepared and draped in a sterile fashion. After local anesthesia was injected under the skin and periostoeum, a “J” needle (Jamshidi Bone Marrow Biopsy and Aspiration Tray; Cardinal Health, McGaw Park, IL) was inserted by hand through the skin into the anterior iliac crest. The needle was rotated gently into 1 cm of the marrow cavity. The stylet was removed from the needle and a 5-cc syringe attached. Bone marrow was aspirated by retraction of the plunger of the syringe. After 2-3 mL of marrow was collected, the needle may be repositioned if more marrow is needed. The syringe was removed from the marrow space with an upward twisting motion. Pressure was placed over the aspiration site for 5 minutes, and a bandage was placed. The aspirated marrow was used to “soak” or impregnate the allogeneic bone [10].
At 1 week post-graft patient was evaluated for any signs of infection and wound dehiscence of recipient site, infection, pain (using 10 point visual analog scale), difficulty in ambulation and numbness of donor site and post-operative panoramic radiograph. At one month post-graft subject was evaluated for infection and wound dehiscence of recipient site as well as infection and numbness of donor site. Panoramic radiograph was also obtained to confirm retention of the bone graft. At 4 months the subjects were again evaluated for signs of infection and wound dehiscence of recipient site and infection and numbness of donor site. A 4month pre-implant cone-beam CT was taken with surgical stent in place.
Cone-Beam CT Height and Width Measurements
An average bone height was be measured along a vertical line drawn from the alveolar crest to the appropriate anatomic barrier (maxillary sinus floor, inferior border of the mandible or the inferior alveolar nerve), parallel to the plane of each planned endosseous dental implant site. To measure bone width, a horizontal line was drawn perpendicular to each vertical line at the presurgical height of the alveolar crest to the appropriate anatomic barrier along the vertical axis of the height measurement line [11].
Results
Measurement of Bone Induction
In Figure 1 shows subjects 1 show the placement of BMA impregnated freeze dried corticocancellous. Figure 1B and 1C shows the use of the Modified Lip-Switch technique in order to obtain primary closure over the BMA impregnated graft. In Figure 1D is an occlusal view of deficient anterior alveolar ridge preop of subject 1. In Figure 1E shows subjects 1 the occlusal view of anterior alveolar ridge 4 months after placement of BMA impregnated freeze dried corticocancellous. Figure F and G facial view of deficient anterior alveolar ridge preop and 4 months postop.
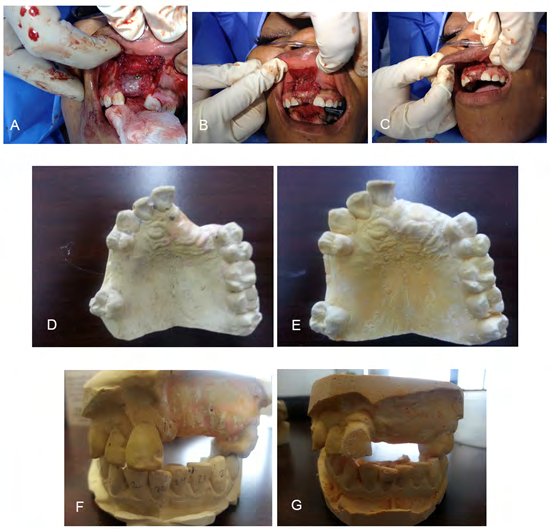
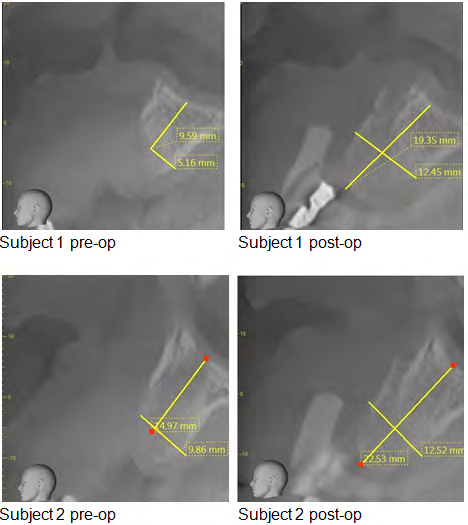
Figure 1: A. Placement of BMA impregnated freeze dried corticocancellous. B and C. Modified Lip-Switch technique to obtain primary closure over the BMA impregnated graft. D. Occlusal view of deficient anterior alveolar ridge preop. E. Occlusal view of anterior alveolar ridge 4 months after placement of BMA impregnated freeze dried corticocancellous. F. Facial view of deficient anterior alveolar ridge preop. G. Facial view of anterior alveolar ridge 4 months after placement of BMA impregnated freeze dried corticocancellous Figure 2 shows preop and postop conebeam CT measurements for subjects 1 and 2. The mean increase in alveolar ridge height of each of the subjects were measured at 4 months after treatment and were similar to established controls using traditional autogenous harvesting sites: 3.9 mm and 3.8 respectively. The mean increase in alveolar ridge width of each of the subjects were measured at the crest of the ridge were similar between both established autogenous, allogeneic as compared to our bone marrow aspirate groups: 4.33, 4.56 and 3.97 respectively. Seven of the 10 patients have received dental implants which have remained osseointegrated at least 1-year post-implantation.
Patient Outcome
We also measured, pain using Visual Analog Scale (VAS) and compared with established harvesting the anterior iliac bone (AIC) and the Tibia. Subject undergoing BMA harvest had VAS scores of one 1 week after harvest as compared to a VAS of 5.5 in published controls using traditional AIC harvest. Also only 9% of subjects reported any pain 1 week after BMA harvest versus 15% and 70% in published controls using the proximal tibia as a harvest site Tables 1 & 2.
| VAS mean @1wk | |
| Barone, et al. | 5.5 |
| Becker, et al. | 5 |
| BMA Pilot Study | 1 |
Table 2: Comparisons of VAS for AIC and BMA harvest sites for maxillofacial grafting.
| % of Postop Pain Report | |
| Kirmeier, et al. | 15% |
| Mardhena, et al. | 70% |
| BMA Pilot Study | 9% |
Table 1: Comparisons of patient reported pain for Tibia and BMA harvest sites for maxillofacial grafting.
Discussion & Conclusion
The use of BMA has been reported in the orthopedic literature to treat non-union of tibia fractures, simple bone cysts in long bones, spinal arthrodesis and thoracolumbar fractures. Bone-marrow injection is as effective in regenerating bone as open autologous grafting with fewer disadvantages [3]. When BMA is added to an osteoconductive matrix to treat simple bone cysts, it was shown to be safe and effective in healing the bony defect [4, 5]. There have also been a few case reports using BMA in continuity defects in mandibles. In one case, a patient originally treated with rhBMP-2 failed to heal and therefore opted for retreatment with the addition of BMA, which resulted in complete healing of the defect [6]. Although there have not been any prospective human studies examining the effectiveness BMA in maxillofacial defects, there has been a few animal studies that have shown some promise. One study created standardized bone defects in minipigs and randomly grafted with autogenous mandibular bone, an alloplastic scaffold, platelet rich plasma (PRP) + scaffold or mesenchymal stem cells (MSC) + PRP + scaffold. Their results showed a significantly higher percentage of bony contact to graft particles as compared to the PRP- scaffold and scaffold alone, which suggest that the addition of mesenchymal stem cells enhance bone formation [7].
More recently, augmentation of other grating materials with BMA has been described in extraction sockets and maxillofacial cystic bone defects. On study evaluated the level of mineralized tissue and expression of RUNX-2 and osteocalcin from anterior extraction site of 15 patients that were randomized into control, platelet-rich fibrin group (PRFG), and BMA concentrate with PRFG (BM/PG) [12, 13]. The histomorphometric analysis of these three groups showed more pronounced mineralization tissue in the PRFG and the BM/PG as compared to the control. Also there was increase of osteocalcin mainly in the BM/PG indicating that the addition of BMAC increased mineralization. Unfortunately, this technique required BM concentrate which requires the provider to have a centrifuge as well as for the PRFG. For our study, we show that the use of BMA as an inexpensive and effective alternative to augment even larger defects as compared to extraction sockets.
In a prospective randomized study of 30 patients with maxillofacial bone cyst of greater than 2 cm, 15 patients were treated with hydroxyapatite (HA) collagen scaffold as the control group and the other 15 received BMA and HA collagen scaffold. The bone defects with BMA and HA collagen scaffold had a statistically significant reduction of the bony defect at 3 and 6 months, as well as less swelling and no tooth mobility at month 3. These results are impressive, but it still requires the use of alloplasts rather that allograft.
Our group believes that our results with the use of BMA and freeze-dried bone give the best results without the use of alloplasts and concentrating the bone marrow cells.
References
-
Baqain ZH, Anabtawi M, Karaky AA, Malkawi Z (2009) Morbidity from anterior iliac crest bone harvesting for secondary alveolar bone grafting: an outcome assessment study. J Oral Maxillofac Surg 67(3): 570-575.
-
Mazock JB, Schow SR, Triplett RG (2003) Posterior iliac crest bone harvest: review of technique, complications, and use of an epidural catheter for postoperative pain control. J Oral Maxillofac Surg 61(12): 1497-1503.
-
Connolly J, Guse R, Lippiello L, Dehne R (1989) Development of an osteogenic bone-marrow preparation. J Bone Joint Surg Am 71(5): 684-691.
-
Kanellopoulos AD, Yiannakopoulos CK, Soucacos PN (2005) Percutaneous reaming of simple bone cysts in children followed by injection of demineralized bone matrix and autologous bone marrow. J Pediatr Orthop 25(5): 671-675.
-
Kanellopoulos AD, Mavrogenis AF, Papagelopoulos PJ, Soucacos PN (2007) Elastic intramedullary nailing and DBM-bone marrow injection for the treatment of simple bone cysts. World J Surg Oncol 5: 111.
-
Carter TG, Brar PS, Tolas A, Beirne OR (2008) Off- label use of recombinant human bone morphogenetic protein-2 (rhBMP-2) for reconstruction of mandibular bone defects in humans. J Oral Maxillofac Surg 66(7): 1417-1425.
-
Pieri F, Lucarelli E, Corinaldesi G, Fini M, Aldini NN, et al. (2009) Effect of mesenchymal stem cells and platelet- rich plasma on the healing of standardized bone defects in the alveolar ridge: a comparative histomorphometric study in minipigs. J Oral Maxillofac Surg 67(2): 265-272.
-
Shayesteh YS, Khojasteh A, Soleimani M, Alikhasi M, Khoshzaban A, et al. (2008) Sinus augmentation using human mesenchymal stem cells loaded into a beta- tricalcium phosphate/hydroxyapatite scaffold. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106(2): 203- 209.
-
Rickert D, Vissink A, Slot WJ, Sauerbier S, Meijer HJ, et al. (2014) Maxillary sinus floor elevation surgery with BioOss® mixed with a bone marrow concentrate or autogenous bone: test of principle on implant survival and clinical performance. Int J Oral Maxillofac Surg 43(2): 243-247.
-
Smiler D, Soltan M (2006) Bone marrow aspiration: technique, grafts, and reports. Implant Dent 15(3): 229- 235.
-
Boyne PJ, Lilly LC, Marx RE, Moy PK, Nevins M, et al. (2005) De novo bone induction by recombinant human bone morphogenetic protein-2 (rhBMP-2) in maxillary sinus floor augmentation. J Oral Maxillofac Surg 63(12): 1693-1707.
-
Martins LCF, de Oliveira ALSC, Aloise AC, de Macedo LGS, Teixeira MLT, et al. (2021) Bone marrow aspirate concentrate and platelet-rich fibrin in fresh extraction sockets: A histomorphometric and immunohistochemical study in humans. J Craniomaxillofac Surg 49(2): 104-
-
Vignesh U, Mehrotra D, Howlader D, Kumar S, Anand V (2019) Bone Marrow Aspirate in Cystic Maxillofacial Bony Defects. J Craniofac Surg 30(3): 247-251.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells