Dental Arch Parameters and Goslon Scores in Mixed Dentition of Egyptian Children with Surgically Repaired Unilateral Cleft Lip and Palate
Introduction: Various forms of malocclusion are usually encountered in non-syndromic cleft lip and palate, mostly affecting maxillary dental arch. Objective: To assess the dental arch parameters in surgically treated unilateral cleft lip and palate Egyptian children with mixed dentition and compare them with those of comparable healthy non-cleft children. Material and Methods: Comparative cross-sectional study design was used. Twenty-six non-syndromic children with repaired unilateral cleft lip and palate (UCLP), aged 6-9 years, were compared to twenty-six healthy non-cleft children (control group) recruited from Faculty of Dentistry, Alexandria University. Both groups were divided into two age groups; 6-7 years and 8-9 years. For each subject, dental arch parameters were measured using dental study models. Results: Mean maxillary arch depth and inter-canine arch width were significantly smaller in UCLP children than in non-cleft children in the age groups 6-7 and 8-9 years. Mean inter-molar arch width was not significantly narrower in UCLP children than in non-cleft children. Mean mandibular arch dimensions of UCLP children did not differ significantly from those of non-cleft children. The mean Goslon Yardstick score was 3. Conclusion: Children with UCLP, aged 6-9 year old, had significant reduction in mean maxillary arch dimensions compared to healthy matching non-cleft children except for inter-molar arch width which showed no significant reduction. The average dental arch relationship in surgically-repaired UCLP children was fair according to Goslon Yardstick index.
Introduction
Cleft lip and palate is a common cranio-facial congenital defect resulting from incomplete fusion of maxillary and intermaxillary processes during development of the fetus [1]. It is multifactorial and is caused by interaction of genetic and environmental factors. Thus, it can occur as an isolated condition or as one component of an inherited disease or syndrome [2, 3, 4]. According to WHO [5], its prevalence worldwide is about one per 500–700 of all births and it differs with cleft type, gender and ethnic origin.
Dental arch parameters are generally altered in patients with clefts. The maxillary arch dimensions are diminished due to either the cleft itself that affect the developing dental arch or the primary surgical repairs [6, 7, 8, 9, 10, 11].
There is no general agreement on the optimal surgical protocol intended for unilateral cleft lip and palate (UCLP) correction [12]. Some centers use a multistage approach, in which more than one operation is done to close the UCLP and others use one-stage repair approach [13]. The Oslo protocol is an example of multistage approach in which lip closure is accomplished by Millard technique [14] at 3 months of age. Then the posterior palate is closed at 18 months using a modified von Langenbeck technique [15]. Finally, alveolar bone grafting is done during the mixed dentition. Secondary surgery can be performed on an individual basis to repair any residual defect [12, 13].
In order to assess the treatment outcome regarding dental arch relationships of various surgical protocols, the Great Ormond Street London, Oslo Norway (Goslon) yardstick ranking system was developed by Mars, et al. [16] and is considered the most commonly used and oldest index to measure treatment outcomes of surgical repair with mixed dentition. It uses an ordinal scale of five categories, excellent, good, fair, poor, very poor, to identify an individual’s occlusal status with a consequent general prediction about the relative complexity of future correction of malocclusion.
The ultimate aim of UCLP treatment is to achieve a normalization of functions such as speech, growth of the naso-maxillary complex, arch dimensions and occlusion as well as facial appearance using a multidisciplinary approach [17]. Pediatric dentists have a responsibility towards the overall dental care of these children. They are involved in the presurgical and postsurgical phase of maxillary orthopedics. Both active and passive appliances can be used to bring the cleft segments to better alignment and thereby promote better initial surgical outcome [18].
In order to implement the highest possible standards of care for UCLP children by the pediatric dentist, it is important to assess early treatment outcome regarding arch dimensions after primary surgical repair of lip and palate. The dental arch dimensions of these children have been evaluated in previous studies [10, 11], few investigators in Egypt tackled this issue [19]. Due to racial differences in development of dental arch and growth patterns, as stated by Lavelle [20], the scarcity of data in Egypt addressing this unfortunate group of children presents a gap that impedes the delivery of proper dental care to them. The present study aims at filling this gap by highlighting the main characteristics of dental arch parameters in surgically repaired UCLP children by the Oslo surgical protocol and compares them with those of healthy, matching, non-cleft.
Material and Methods
The study had a comparative cross sectional design. Five hundred cleft children registered in the period January 2006 till December 2009 in Orthodontics as well as Maxillo- facial and Plastic Surgery departments, Faculty of Dentistry, Alexandria University were examined during period from September 2014 to April 2015. They were all surgically repaired in the Maxillo-facial and Plastic Surgery department of Alexandria University which serves as a central hospital for Alexandria Governorate and other nearby governorates (Kafr El Sheikh, El Beheira and Marsa Matrouh) and other rural areas. The inclusion criteria were non-syndromic complete UCLP children of both genders, with mixed dentition and surgically repaired according to the Oslo surgical protocol [13]. Four hundred and sixteen children had other types of clefts (incomplete UCLP, isolated cleft palate, bilateral cleft lip and palate and unilateral cleft lip) so they were excluded from our study. We also excluded nineteen UCLP children with systemic diseases, intellectual disabilities or syndromes and other congenital anomalies. Furthermore thirty five children were excluded because they had previous naso-alveolar moulding, orthodontic treatment, bone graft or prematurely extracted multiple teeth due to caries. Four UCLP children with more than one year (±) difference between chronological and dental ages (assessment of dental age was based on the Schour and Massler tables) were also excluded [21]. Only twenty-six UCLP children, (20 boys and 6 girls) with a mean age of 7.83 years, fulfilled the inclusion criteria and were included in our study.
Twenty-six healthy, gender and age matched non-cleft children were also recruited for comparisons. They were free from oral habits and with limited or no crowding of teeth and no premature loss of teeth. They were selected from neighbors or school-mates (companions) of UCLP children.
Ethical approval for the study was obtained from Dental Research Ethics Committee, Faculty of Dentistry, Alexandria University. The children’s parents or guardians were asked to sign an informed consent. Participants were assured of the confidentiality of the collected data and that it was used only for research purposes.
Measurements were carried out by the researcher who was trained and calibrated to an acceptable level of intra- examiner consistency in assessing dental arch dimensions based on non-significant differences between duplicate measurements using paired t test.
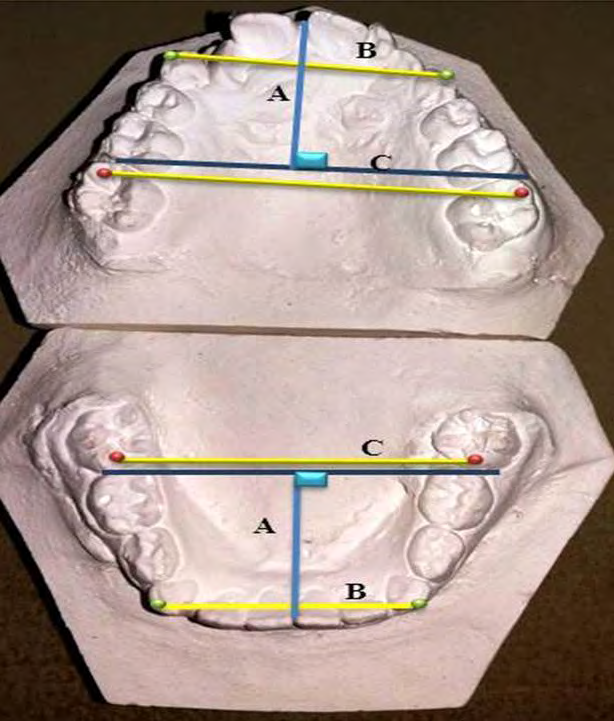
For each subject, demographic data were recorded and intra-oral examination was done to determine cleft side. Upper and lower alginate impressions were taken and dental arch dimensions were measured using digital boley gauge (ProDent USA digital Caliper 4”, from the study casts (Figure 1).
a) Maxillary and mandibular arch depths (A in Figure 1): measured in millimeters from the median point between the central incisors (or the mesio-incisal corner of the central incisor in case of missing central incisor) until the tangent line to the mesial surface of the first permanent molars [22]. b) Maxillary and mandibular inter-canine arch widths (B in Figure 1): measured in millimeters between cusp tips of the right and left primary or permanent canines in maxillary and mandibular arches respectively. In case of missing or un-erupted canines, this measurement was substituted by the inter-first primary molar arch width, which is the distance between buccal cusp tips of the right and left first primary molar in both arches [22]. c) Maxillary and mandibular inter-molar arch widths (C in Figure 1): measured in millimeters between mesio- buccal cusp tips of the right and left permanent first molars in maxillary and mandibular arches respectively [22]. In cases of cusp tip flattening by wear, the reference point (estimated cusp tip) was marked as the central point in the middle of the wear facet, according to Bishara, et al. [23]. d) Incisor relationship: over-jet, over bite and open bite were measured on the dental study casts. Over-jet and open bite were both measured in millimeters and over bite was measured as the percentage of vertical overlap of maxillary incisors to mandibular incisors [22]. e) Midline deviation was determined clinically and from the dental casts of the patients by determining the reference line and maxillary and mandibular dental midlines. The reference line is the line between Glabella and Subnasale and it is determined clinically. The Glabella is the midpoint between the eyebrows and the Subnasale is the base of the nose. The dental midline is the mid-sagittal line of maxillary and mandibular dental arches possessing teeth of ideal size, shape, and position, when situated in maximum intercuspation. It passes between the mesial surfaces of the two central incisors. If one of the central incisors is missing then the dental midline is determined through the line tangent to the mesial contact area of the present central incisor. If the dental midline coincided with the reference line then there is no midline deviation. The dental midline was also related to the labial frenum and the incisive papilla as guiding points from dental casts. If the dental midline was coinciding with the guiding point then the dental midline was centered. If the dental midline was located to the right or the left of the guiding point then the midline was deviated and the side of deviation was determined [22].
Dental arch relationships: the casts were ranked using GOSLON Yardstick by one calibrated researcher. The features assessed in the GOSLON Yardstick and the descriptions of each grade are shown in Table 1 adapted from Alam, et al. [24].
| Goslon Yardstick Rank | General Features |
| 1 (Excellent) | Favorable Advantageous skeletal form Positive overjet and overbite Exhibit Angle Class II division 1 |
| 2 (Good) | Favorable relationship Class I dental relationship |
| 3 (Fair) | Edge to edge dental relationship (Class III malocclusion) In case of borderline case between 3 and 4: Deep overbite - group 3 |
| 4 (Poor) | Unfavorable facial growth Reverse overjet of 3 to 5 mm case belong to group 4 In case of borderline case between 3 and 4: anterior openbite – group 4 |
| 5 (Very Poor) | Significant Class III Reverse overjet of 3 to 5 mm but marked proclination of upper incisors and retroclination of lower incisor |
Table 1: General features of the models in the Goslon yardstick.
Statistical Analysis
Data were entered into an Excel file and imported to IBM SPSS software version 20.0 for analysis. Descriptive statistics (frequencies and percentages as well as means and standard deviations) were calculated. Dental arch dimensions and incisor relationship were compared using Independent samples t-test. Midline deviation was compared using Fisher exact test. P< 0.05 was considered statistically significant.
Results
In the UCLP group, males represented 76.9 % of the group and in the non-cleft group, 69.2 % were males, P=0.652. The mean ±SD age was 7.83 ± 1.52 years in UCLP children and 7.63 ± 1.52 in non-cleft children, P=0.973.
As shown in Table 2, the mean maxillary arch depth was significantly smaller in UCLP children than in non-cleft children in both 6-7 years old group (P=0.004) and 8-9 years (P=0.026). There was no significant difference between both groups regarding mean mandibular arch depth (P=0.410 and 0.670 in 6-7 years and 8-9 years respectively).
| 6-7 year old children | 8-9 year old children | ||||||
|---|---|---|---|---|---|---|---|
| UCLP | Non-cleft | P value | UCLP | Non-cleft | P value | ||
| Arch Depth | Maxillary | 22.38±3.70 | 25.62±1.94 | t =3.2 0.004* | 21.44±4.39 | 25.26±2.19 | t = 2.4 0.026* |
| Mandibular | 24.15±2.86 | 21.44±2.08 | t =0.8 0.410 | 22.53±2.33 | 22.08±3.09 | t =0.4 0.670 | |
| Inter- canine width | Maxillary | 26.84±2.57 | 31.71±2.70 | t =3.2 0.004* | 26.02±5.24 | 33.98±2.52 | t =4.7 0.001* |
| Mandibular | 25.98±2.14 | 24.75±2.97 | t =0.8 0.425 | 26.92±4.37 | 26.22±2.11 | t =0.3 0.770 | |
| Inter- molar width | Maxillary | 45.15±4.82 | 46.15±3.92 | t =0.1 0.884 | 45.26±4.99 | 49.75±3.84 | t =1.1 0.285 |
| Mandibular | 45.24±3.23 | 45.26±4.88 | t =1.6 0.134 | 45.37±3.25 | 45.44±3.97 | t =1.0 0.305 | |
| Over-jet in mm | -3.10±5.40 | 2.20±1.50 | t =3.2 0.004* | 1.40±5.00 | 2.90±1.80 | t =1.0 0.328 | |
| Open bite in mm | 6.00±1.50 | - | - | 3.90±2.60 | - | - | |
| Overbite % | 17.40±17.60 | 23.80±26.90 | t =0.62 0.543 | 23.00±26.90 | 24.30±21.10 | t =0.14 0.889 |
Table 2: Comparison between UCLP and non-cleft children with respect to Maxillary and Mandibular arch depths, Inter-canine arch w
The mean maxillary inter-canine width was significantly narrower in the UCLP group than in non-cleft group in both 6-7 years old group (P=0.004) and 8-9 years (P= 0.001). There was no significant difference between groups regarding mandibular inter-canine arch width in the age groups 6-7 years and 8-9 years (P=0.425 and 0.770 respectively).
There was no significant difference between both groups in the mean maxillary and mandibular inter-molar width in the age groups examined (P= 0.884 and 0.134 for 6-7 years old children and 0.285 and 0.305 for 8-9 years old children).
There were no significant differences between UCLP
and non-cleft children with respect to over-bite in both age groups (P=0.543 and 0.889). As for over-jet, there was significant difference between UCLP and non-cleft children in the age group 6-7 years (P=0.004) but not in the 8-9 years old group (P= 0.328). No open bite was seen in the non-cleft children.
As presented in Table 3, midline deviation was more frequent in UCLP than in non-cleft groups in both age groups (P=0.001 in 6-7 years group and P=0.016 in 8-9 years group). In addition, predilection of midline deviation, if exists, in UCLP group was towards non-cleft side.
| 6-7 year old children | 8-9 year old children | |||||
|---|---|---|---|---|---|---|
| UCLP | Non-cleft | P value | UCLP | Non-cleft | P value | |
| No midline deviation | 1 (6.25) | 17 (94.4) | 0.001* | 2 (20) | 7 (87.5) | 0.016* |
| Midline Deviation | 15 (93.75) | 1 (5.56) | 8 (80) | 1 (12.5) |
Table 3: ** Comparison between UCLP and non-cleft children regarding midline deviation. Table 4 shows the percentage distribution
*: statistically significant at P< 0.05 Table 3: Comparison between UCLP and non-cleft children regarding midline deviation. Table 4 shows the percentage distribution of UCLP children across the Goslon Yardstick Ranks in both age groups. The mean Goslon Yardstick score is 2.9±1.3 in 6-7 year old children and 3.1±1.0 in 8-9 year old children.
| Goslon Yardstick Rank | UCLP (n=26) | |
|---|---|---|
| 6-7 year old children | 8-9 year old children | |
| (n=16) | (n=10) | |
| Group 1: Excellent | 3(18.75%) | 0(0%) |
| Group 2: Good | 3(18.75%) | 3(30%) |
| Group 3: Fair | 5(31.25%) | 4(40%) |
| Group 4: Poor | 3(18.75%) | 2(20%) |
| Group 5: Very Poor | 2(12.5%) | 1(10%) |
| Total | 16(100%) | 10 (100%) |
| Mean | 2.9±1.3 | 3.1±1.0 |
| Median | 3 | 3 |
Table 4: Percentage distribution of UCLP children across the Goslon Yardstick Ranks.
Discussion
Children with unilateral cleft lip and palate (UCLP) usually exhibit deficient naso-maxillary complex due to tissue deficiency, scar tissue formation after early reconstructive surgery and inherent growth retardation. Consequently, maxillary dental arch development is also retarded [6].
The great variations in the early surgical repair outcome of UCLP can be attributed to several factors [25]. This fact, in addition to scarcity of data available in Egypt regarding early outcome assessment initiated this descriptive study to establish baseline information for the pediatric dentists to improve the standards of care available to this vulnerable group of children.
In the present study, UCLP children were divided into two critical age periods of mixed dentition (6-7 years) and (8-9 years). Among these age groups, different preventive and interceptive orthodontic interventions have been reported to improve the dental arch dimensions and occlusion for UCLP children [25].
In the present study, digital calipers were used to measure the dental arch dimensions from dental casts directly. This method was used rather than the visual 3D
dental cast analysis on account of the assumption of Ooster Kamp, et al. [26], who reported that the reliability of visual 3D dental cast analysis is uncertain and time-consuming.
Goslon Yardstick index was used to assess the dental arch relationship in this study as Modified Huddart Bodenham (MHB) system was used in another part of our study Baraka, et al. [27]. In addition to the fact that Goslon Yardstick index is the most common scoring system to compare surgical outcomes across different cleft centers, it is possible that the overall MHB score does not accurately represent the severity of the malocclusion: mild generalized irregularity may yield a higher score than a more severe but localized anomaly as stated by Mars, et al. [16].
The mean maxillary dental arch depth was significantly deficient in the age groups 6-7 years and 8-9 years compared to healthy children. This is in agreement with the study of Athanasiou, et al. [28] which stated that early palatoplasty lead to maxilla growth inhibition in all dimensions. Deficiency could be also related to the palate-version of the maxillary central incisors, the mesial drifting of the first permanent molars due to congenitally missing teeth as well as ectopically erupting first permanent molars.
The mean maxillary inter-canine width was significantly narrower in UCLP group in the age groups 6-7 years and 8-9 years, which support the findings of the studies performed by Athanasiou, et al. [28] and Stein, et al. [29].
Mean maxillary inter-molar width values were not significantly different from that of non-cleft group in both age groups. This coincides with the study performed by Garrahy, et al. [10]. The reason behind this finding might be due to larger maxillary inter-molar arch width in UCLP children at birth compared to non-cleft children as reported by Kramer, et al. [30]. Consequently, after surgical palatal closure and scar tissue formation, the inter-molar arch width values of UCLP children start to approach those of non-cleft children during mixed dentition stage.
The present study showed that there were no significant differences in the mean mandibular arch dimensions among both age groups between UCLP and non-cleft children. The results suggest that the effect of maxillary arch surgery does not influence remarkably on the mandibular arch dimensions. This finding agrees with other studies such as that of Derijcke, et al. [31] and Garrahy, et al. [10].
Regarding incisor relationship, UCLP children showed a statistically significant negative mean over-jet in the age group 6-7 years. As for the age group 8-9 years, over-jet mean value was not significant between both groups. This might be due to the presence of few cases who were developing class II with maxillary protrusion. Anterior open bite also existed in many of UCLP children owing to severe maxillary retrusion in many cases.
As regards midline deviation, significant maxillary midline deviation existed in most of UCLP group. Predilection of midline deviation, if exists, in UCLP group was towards non-cleft side. This finding agrees with what was mentioned in the study performed by Prahl, et al. [32] that midline deviation in UCLP cases is towards the non-cleft side.
With respect to Goslon Yardstick scoring, it was shown that the mean score for surgically repaired UCLP children in Alexandria University is approximately three which is fair. This mean score is comparable with other cleft centers in other countries such as U.K, Oslo, Eurocleft centers and Tokyo (with mean scores 3.14, 2.29, 2.47 and 3.64 respectively) as reported in studies conducted by Mars, et al. [23], [33, 34, 35], Molsted, et al. [36], Nollet, et al. [37] and Susami, et al. [38].
The main limitation revealed in our study that should be taken into consideration is the small number of children recruited. The study included attendants of the Maxillo- Facial and Plastic Surgery Department as well as Orthodontic Department, Faculty of Dentistry, Alexandria University during the period from September 2014 throughout April 2015. In spite of the several significant differences between UCLP and matching healthy children, these results should be interpreted cautiously before they are regarded as representative of UCLP children in the Egyptian population [39, 40].
Further research should be initiated to assess arch dimensions and dental arch relationship following different interceptive orthodontic measures and alveolar bone grafting in attempt to improve surgical outcomes. In addition, characteristics of arch parameters in children with different types of cleft lip and palate in Egyptian children should be also investigated.
Conclusion
Based on the results of present study:
- Children with UCLP repaired with Oslo protocol revealed significant reduction in mean maxillary arch measurements (arch depth and inter-canine arch width) when compared to healthy children while mean maxillary inter-molar arch width did not differ significantly among UCLP and non-cleft groups.
- Mean mandibular arch parameters (arch depth, inter- canine arch width, inter-molar arch width) were not influenced by the deficient maxillary arch and were comparable to those of non-cleft healthy children.
- The main treatment outcome based on dental arch relationships among Egyptian children born with non- syndromic complete UCLP seems to be fair as the mean score of Goslon Yardstick is 3.0.
Conflict of interest
The authors declare that they have no conflicts of interest.
References
-
Marazita ML, Mooney MP (2004) Current concepts in the embryology and genetics of cleft lip and cleft palate. Clin Plast Surg 31(2): 125-140.
-
Cobourne MT (2004) The complex genetics of cleft lip and palate. Eur J Orthod 26(1): 7-16.
-
Rice DP (2005) Craniofacial anomalies: from development to molecular pathogenesis. Curr Mol Med 5(7): 699-722.
-
Mossey PA, Little J, Munger RG, Dixon MJ, Shaw WC (2009) Cleft lip and palate. Lancet 374: 1773-1785.
-
World Health Organization (WHO) (2012) Oral Health.
-
Athanasiou AE, Mazaheri M, Zarrinnia K (1987) Longitudinal study of the dental arch dimensions in bilateral cleft lip and palate patients. J Pedod 11(3): 253- 268.
-
Nystrom M, Ranta R (1989) Sizes of dental arches and interdental space in 3-year-old children with and without cleft lip/palate. Eur J Orthod 11(1): 82-88.
-
da Silva Filho O, Ramos A, Abdo R (1992) The influence of unilateral cleft lip and palate on maxillary dental arch morphology. Angle Orthod 62(4): 283-290.
-
McCance A, Roberts Harry D, Sherriff M, Mars M, Houston WJ (1993) Sri Lankan cleft lip and palate study model analysis: clefts of the secondary palate. Cleft Palate Craniofac J 30(2): 227-230.
-
Garrahy A, Millett DT, Ayoub AF (2005) Early assessment of dental arch development in repaired unilateral cleft lip and unilateral cleft lip and palate versus controls. Cleft Palate Craniofac J 42(4): 385-391.
-
Lewis BR, Stern MR, Willmot DR (2008) Maxillary anterior tooth size and arch dimensions in unilateral cleft lip and palate. Cleft Palate Craniofac J 45(6): 639- 646.
-
Costello B, Ruiz R (2004) Cleft lip and palate: Comprehensive treatment planning and primary repair. In: Miloro M, et al. (Eds.), Peterson’s principles of oral and maxillofacial surgery, 2nd (Edn.), Hamilton: BC Decker inc; pp: 839-858.
-
Fudalej P, Hortis Dzierzbicka M, Dudkiewicz Z, Semb G (2009) Dental arch relationship in children with complete unilateral cleft lip and palate following Warsaw (one-stage repair) and Oslo protocols. Cleft Palate Craniofac J 46(6): 648-653.
-
Millard RD (1968) Extensions of the rotation- advancement principle for wide unilateral cleft lips. Plast Reconstr Surg 42(6): 535-544.
-
Stewart TL, Fisher DM, Olson JL (2009) Modified Von Langenbeck Cleft palate repair using an anterior triangular flap: decreased incidence of anterior oronasal fistulas. Cleft Palate Craniofac J 46(3): 299-304.
-
Mars M, Plint DA, Houston WJB, Bergland O, Semb G (1987) The Goslon Yardstick: a new system of assessing dental arch relationships in children with unilateral clefts of the lip and palate. Cleft Palate J 24(4): 314-322.
-
Long RE, Hathaway R, Daskalogiannakis J, Mercado A, Russell K, et al. (2011) The americleft study: an inter- center study of treatment outcomes for patients with unilateral cleft lip and palate part 1. Principles and study design. Cleft Palate Craniofac J 48(3): 239-243.
-
Jones J, Sadove AM, Dean JA, Huebener DV (2011) Multidisciplinary team approach to cleft lip and palate management. In: McDonald R, et al. (Eds.), Dentistry for the Child and Adolescent, 9th (Edn.), Missouri: Mosby; pp: 550-60.
-
El Koutby MM, Hafez SA (1993) Prevalence of malocclusion in the primary and early mixed dentition in a group of Egyptian children with complete unilateral cleft lip and palate. Egypt Dent J 39(3): 479-484.
-
Lavelle CL (1975) The shape of dental arch. Am J ORthod 67(2): 176-184.
-
Graber TM (1974) Orthodontics, principles and practice. Philadelphia: WB Saunders pp: 90-101.
-
Burdi AR, Moyers RE (1988) Development of the dentition and the occlusion. In: Moyers RE (Eds.), Handbook of Orthodontics, 4th (Edn.), Chicago: Year Book Medical Publisher Inc; pp: 99-146.
-
Bishara SE, Bayati P, Zaher AR, Jakobsen JR (1994) Comparisons of the dental arch changes in patients with Class II, division 1 malocclusions: extraction vs nonextraction treatments. Angle Orthod 64(5): 351-358.
-
Alam MK, Kajii TS, Koshikawa Matsuno M, Sugawara Kato Y, Sato Y, et al. (2008) Multivariate analysis of factors affecting dental arch relationships in Japanese unilateral cleft lip and palate patients at Hokkaido University Hospital. Orthodontic Waves 67(2): 45-53.
-
Reiser E (2011) Cleft Size and Maxillary Arch Dimensions in Unilateral Cleft Lip and Palate and Cleft Palate. PhD Thesis, Faculty of Medicine, Uppsala University.
-
Oosterkamp BC, van der Meer WJ, Rutenfrans M, Dijkstra PU (2006) Reliability of linear measurements on a virtual bilateral cleft lip and palate model. Cleft Palate Craniofac J 43(5): 519-523.
-
Baraka M, Hanno A, Bakry NS, Medra A, Moussa H (2017) Transverse Dental Arch Relationship and Occlusion in Surgically Repaired Unilateral Cleft Lip and Palate Egyptian Children. Med Clin Res & Rev 1(2): 1-7.
-
Athanasiou AE, Mazaheri M, Zarrinnia K (1988) Dental arch dimensions in patients with unilateral cleft lip and palate. Cleft Palate J 25(2): 139-145.
-
Stein S, Dunsche A, Gellrich NC, Härle F, Jonas I (2007) One-or-Two- stage palate closure in patients with unilateral cleft lip and palate: Comparing cephalometric and occlusal outcomes. Cleft Palate Craniofac J 44(1): 13- 22.
-
Kramer GJ, Hoeksma JB, Prahl Andersen B (1996) Early palatal changes after initial palatal surgery in children with cleft lip and palate. Cleft Palate Craniofac J 33(2): 104-111.
-
Derijcke A, Kuijpers Jagtman AM, Lekkas C, Hardjowasito W, Latief B (1994) Dental arch dimensions in unoperated adult cleft palate-palate patients: an analysis of 37 cases. J Craniofac Genet Dev Biol; 14(1): 69-74.
-
Prahl C, Andersen PB, Bongaarts C, Bronakhorst E, Ongkosuwito E, et al. (2009) The effects of infant orthopedics in patients with cleft lip and palate until six years of age. CLEFT Palate Craniofac J 46(6): 654-663.
-
Mars M, Houston WJ (1990) A preliminary study of facial growth and morphology in unoperated male unilateral cleft lip and palate subjects over 13 years of age. Cleft Palate Craniofac J 27(1): 7-10.
-
Mars M, Asher McDade C, Brattstrom V, Dahl E, McWilliam J, et al. (1992) The RPS. A six-center international study of treatment outcome in patients with clefts of the lip and palate. Part 3. Dental arch relationships. Cleft Palate Craniofac J 29(5): 405-408.
-
Mars M, Batra P (2006) Complete Unilateral Cleft Lip and Palate: Validity of the Five-Year Index and the Goslon Yardstick in Predicting Long-Term Dental Arch Relationships. Cleft Palate Craniofac J 43(5): 557-562.
-
Molsted K, Asher McDade C, Brattstrom V, Dahl E, Mars M, et al. (1993) Timing of hard palate closure and dental arch relationships in unilateral cleft lip and palate patients: a mixed-longitudinal study. Cleft Palate Craniofac J 30(4): 391-396.
-
Nollet PJPM, Katsaros C, Hof MAV, Kujpers Jagtman AM (2005) Treatment outcome in unilateral cleft lip and palate evaluated with the GOSLON Yardstick: A meta- analysis of 1236 patients. Plast Reconstr Surg 116(5): 1255-1262.
-
Susami T, Ogihara Y, Matsuzaki M, Sakiyama M, Takato T, et al. (2006) Assessment of Dental Arch Relationships in Japanese Patients With Unilateral Cleft Lip and Palate. Cleft Palate Craniofac J 43(1): 96-102.
-
Atack N, Hathorn I, Mars M, Sandy J (1997) Study models of 5 year old children as predictors of surgical outcome in unilateral cleft lip and palate. Eur J Orthod 19(2): 165- 170.
-
Atack N, Hathorn I, Semb G, Dowell T, Sandy JR (1997) A new index for assessing surgical outcome in unilateral cleft lip and palate subjects aged five: reproducibility and validity. Cleft Palate Craniofac J 34(3): 242-246.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells