Evaluation of Onset and Duration Period of Pulpal Anesthesia on Articaine, Buffered Articaine, Lignocaine and Buffered Lignocaine in Inferior Alveolar Nerve Block
Context: Pain is one of the most commonly experienced symptoms in dentistry, and managing pain is of greater importance during dental treatment. Local anesthetics are chemicals that block nerve conduction in a specific, temporary and reversible manner, without affecting the patient’s consciousness. Aims: The aim of this study is to evaluate the anesthetic efficacy of buffered lignocaine, buffered articaine, unbuffered lignocaine and unbuffered articaine in terms of latency (onset of anesthetic effect), duration of anesthetic effect during extraction of mandibular teeth following standard inferior alveolar nerve block. Settings and Design: This study was conducted at Department of Oral and Maxillofacial Surgery, Saveetha University, Chennai from November 2013 to November 2015. Methods and Materials: This study compares the anesthetic efficacy of 4% articaine, 2% lignocaine, 4% buffered articaine and 2% buffered articaine with epinephrine. Onset, duration of anesthetic effect was compared. Statistical analysis used: ANOVA Results: Total number of patients were 272. These patients were equally divided into 4 groups, each group containing 68 patients.THE anova test shows that significant difference between the groups, the mean value shows the group 4 is better than the other 3 groups. Conclusion: We conclude that 4% articaine has faster onset when compared to the other three group. Buffered lignocaine had significantly longer duration when compared to the other groups. This can be explained based on its different chemical structure, liposolubility, increased protein binding ability, diffusion in soft tissue and increased pulpal anesthesia.
Introduction
Pain is one of the most commonly experienced symptoms in dentistry, and managing pain is of greater importance during dental treatment [1, 2]. Local anesthetics are chemicals that block nerve conduction in a specific, temporary and reversible manner, without affecting the patient’s consciousness [3]. Carl Koller, a junior ophthalmologist is considered “Father of Local Anesthesia” [4]. William Halstad was the first person to use cocaine for conduction anesthesia [3]. Alfred Einhorn discovered Procaine, which marked the beginning of modern era regional anesthesia [5].
Although the patient may be told that the injection will feel “like a mosquito bite”, it is often much worse. To minimize the patient’s discomfort during a procedure has obvious benefits for both the patient and the surgeon. Although it is short-lived, the perceived pain of the injection of local anesthetic is bad enough for some patients to decline further interventions under local anesthesia. To give additional analgesics, or sedatives, or both, can be impractical and time consuming; it is even at times contraindicated [6].
The challenge is that while local anesthetic is the primary tool for pain management, its acidity may contribute to lengthy anesthetic waiting periods and cause the bee-sting effect or burning and stinging during the injection many of us are surprised to learn that the most widely used dental anesthetic solution are formulated at the pH of lemon juice [5].
Dental anesthetic was first studied by GRDS and then written by Laewen in 1910. Since the introduction of lidocaine in 1948, there have been dozens of studies evaluating whether alkalainisation would improve onset time or reduce injection pain. Occasionally alkalanisation has been studied in combination with warming or injection speed [7, 8].
The present study compares the anesthetic efficacy on onset and duration of buffered lignocaine, unbuffered lignocaine, buffered articaine and unbuffered articaine, in application to truncal block of the inferior alveolar nerve during the extraction.
Subjects and Methods
Study Design
This prospective study was approved by the human studies review board of Saveetha Dental College, after which 272 healthy patients aged 15-80 years gave their written consent to participate. They were among patients who were to have procedure under local anaesthesia in the mandibular region.
Surgical Procedure
All 272 patients were given standard nerve blocks anaesthetising inferior alveolar, lingual and long buccal. This 272 patients were given all these nerve blocks. All patients were randomly divided into 4 groups. Each one picked a slip and had the LA according to the group allotted randomly.
One group was given lignocaine hydrocholoride with adrenaline 1:80,000 solution as LA .Second group was given 4% articaine in 1:1,00,000 solution as LA . Third group was given buffered articaine that is a total of 1 ml of 7.5% sodium bicarbonate was added to 30 ml of vial containing 4 % of articaine as LA. Fourth group was given buffered lignocaine that is a total of 7.5% sodium bicarbonate. 3ml was added to 30ml vial containing 2% lignocaine hydrochloride with 1:80,000 adrenaline solution which yields one tenth dilution.
All the patients had the procedure explained to them. Both the operators and patients were unaware of which anaesthetic the patient had given. All LA in 4 groups were given using non pyrogenic, non-toxic sterile, single use injection. A maximum of 2.5 ml solution was used for all these blocks.
The time of onset of anaesthesia is defined as the first sensation of numbness or tingling in the anaesthetised region. It was calculated from the point of retrieval of the needle after the injection. A straight probe was used to assess the onset of anaesthesia by inserting it in the gingival sulcus of the teeth in the area of anaesthesia.
Duration of anaesthetic effect was recorded via telephonic interview.
Results
Following completion of the clinical study on the patients the data taken from the patients were tabulated for statistical studies after decoding drugs used.
Total number of patients were 272. These patients were equally divided into 4 groups, each group containing 68 patients (Table 1).
| Group I (%) | Group II (%) | Group III (%) | Group IV (%) | Overall | |
|---|---|---|---|---|---|
| Male | 28(42.4) | 32(45.1) | 22(32.8) | 36(52.9) | 118 |
| Female | 38(57.6) | 39(54.9) | 45(67.2) | 32(47.1) | 154 |
| Overall | 68 | 68 | 68 | 68 | 272 |
Table 1: Basic Demographical Variables Descriptive Statistics.
Among the total participants 118 (43.4%) were male and 154 (56.6 %) were female (Table 2).
| Age | Group I (%) | Group II (%) | Group III (%) | Group IV (%) | No. of Partici- pants | Percentage | Mean | SD |
|---|---|---|---|---|---|---|---|---|
| 10-20yrs | 6(9.1) | 10(14.1) | 6(9) | 9(13.2) | 31 | 11.4 | 3.03 | 1.46 |
| 20-30yrs | 20(30.3) | 21(29.6) | 25(37.3) | 21(30.9) | 87 | 32 | ||
| 30-40yrs | 14(21.2) | 17(23.9) | 18(26.9) | 20(29.4) | 69 | 25.4 | ||
| 40-50yrs | 11(16.7) | 10(14.1) | 9(13.4) | 8(11.8) | 38 | 14 | ||
| 50-60yrs | 8(12.1) | 9(12.7) | 2(3) | 6(8.8) | 25 | 9.2 | ||
| 60-70yrs | 7(10.6) | 3(4.2) | 5(7.5) | 2(2.9) | 22 | 7.3 | ||
| 70-80yrs | 0(0) | 1(1.4) | 2(3) | 2(2.9) | ||||
| Total | 66 (24.3) | 71(26.1) | 67(24.6) | 68(25) |
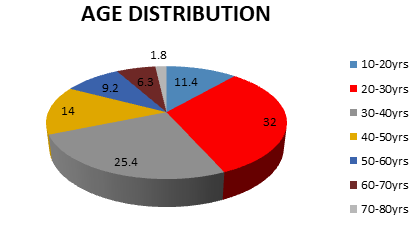
Table 2: Age Distribution of 4 Groups.
Table 2 and Figure 1 shows the more of the participants were participated at the age group of 30-40 years, the mean age and sd is 3.03±1.46.
| Sum of squares | Df | Mean Square | F | Sig. | |
|---|---|---|---|---|---|
| Between Groups | 1670.99 | 3 | 556.99 | 278 | 0.000* |
| Within Groups | 536.95 | 268 | 2 |
Table 3: ANOVA Test for Comparison of 4 Groups.
| Group | N | Mean (sec) | SD | Standard Error | 95% CI | |
|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | |||||
| 1 | 68 | 332.12 | 63.9 | 7.87 | 316.4 | 347.83 |
| 2 | 68 | 185.92 | 63.4 | 7.53 | 170.9 | 200.94 |
| 3 | 68 | 339.52 | 73.2 | 8.94 | 321.7 | 357.39 |
| 4 | 68 | 239.66 | 27.86 | 3.37 | 100.9 | 114.39 |
Table 4: ANOVA Test for Comparison of 4 Groups.
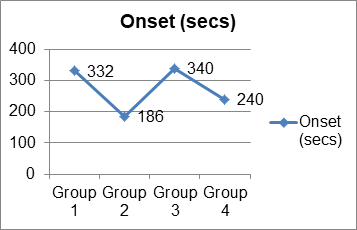
The anova test (Figure 2) shows that significant difference between the groups, the mean value shows the group 3 is better than the other 3 groups. The mean plot diagram also shows that group 3 is better than the other group treated with onset.
| Group | Mean Difference | SD Error | Sig. | 95% CI | ||
|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | |||||
| 1 | 2 | 146..20 | 10.19 | 0 | 119.8 | 172.57 |
| 3 | 7.4 | 10.34 | 0.891 | 34.14 | 19.34 | |
| 4 | 224.47 | 10.3 | 0 | 197.8 | 251.12 | |
| 2 | 1 | 146.2 | 10.19 | 0 | 172.6 | 119.84 |
| 3 | 153.6 | 10.16 | 0 | 179.9 | 127.34 | |
| 4 | 78.26 | 10.12 | 0 | 52.1 | 104.43 | |
| 3 | 1 | 7.4 | 10.34 | 0.891 | 19.34 | 34.14 |
| 2 | 153.6 | 10.16 | 0 | 127.3 | 179.87 | |
| 4 | 231.87 | 10.26 | 0 | 205.3 | 258.42 | |
| 4 | 1 | 224.47 | 10.3 | 0 | 251.1 | 197.83 |
| 2 | 78.26 | 10.12 | 0 | 104.4 | 52.1 | |
| 3 | 231.87 | 10.26 | 0 | 258.4 | 205.33 |
Table 5: Multiple Comparison.
There was statistically significant difference between groups as determined by anova (3,268) = 278, p=0.000. A turkey post hoc test revealed that the time to complete the problem was statistically significant higher in group 3. There was a no statistical difference between the other groups (Table 5).
| Sum of squares | Df | Mean Square | F | SIG | |
|---|---|---|---|---|---|
| Between Groups | 541.4 | 3 | 180.46 | 182.9 | 0.000* |
| Within Groups | 264.41 | 268 | 0.987 |
Table 6: Anova test for duration.
| Group | N | Mean (min) | SD | Standard Error | 95% CI | |
|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | |||||
| 1 | 66 | 159 | 63.911 | 3.22 | 152.2 | 165.07 |
| 2 | 71 | 215 | 63.46 | 3.42 | 208.7 | 222.32 |
| 3 | 67 | 196 | 73.25 | 5.39 | 185.2 | 206.72 |
| 4 | 68 | 276 | 27.86 | 4.36 | 267 | 284.45 |
Table 7: Anova test for duration.
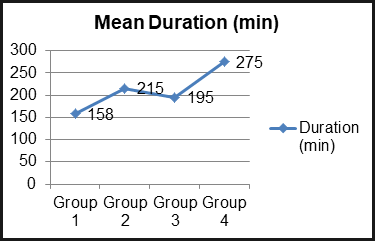
The anova test (Figure 3) shows that significant difference between the groups, the mean value shows the group 4 is better than the other 3 groups. The mean plot diagram also shows that group 4 is better than the other group when tested with duration.
There was statistically significant difference between groups as determined by anova f (3,268)=182.97, p=0.000. A tukey post hoc test revealed that the time to complete the study was statistically significant higher in group 4 (Table 6). There was no statistical difference between the other groups.
| Group | Mean Difference | Sd error | Sig. | 95% CI | ||
|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | |||||
| 1 | 2 | 58.85 | 5.89 | 0 | 72.1 | 41.62 |
| 3 | 37.04 | 5.97 | 0 | 52.76 | 21.85 | |
| 4 | 117.1 | 5.95 | 0 | 132.5 | 101.7 | |
| 2 | 1 | 58.57 | 5.89 | 0 | 41.62 | 72.1 |
| 3 | 19.55 | 5.87 | 0.005 | 4.37 | 34.73 | |
| 4 | 60.24 | 5.85 | 0 | 75.36 | 45.12 | |
| 3 | 1 | 37.3 | 5.97 | 0 | 21.85 | 52.76 |
| 2 | 19.55 | 5.87 | 0 | 34.73 | 4.37 | |
| 4 | 79.79 | 5.85 | 0.005 | 95.14 | 64.45 | |
| 4 | 1 | 117.1 | 5.95 | 0 | 101.7 | 132.5 |
| 2 | 60.24 | 5.85 | 0 | 45.12 | 75.36 | |
| 3 | 79.79 | 5.93 | 0 | 64.45 | 95.14 |
Table 8: Multiple Comparison.
Discussion
Local anaesthtics form the backbone of pain control techniques in dentistry [9, 10]. LA’s are the safest and the most effective drugs in medicine for the prevention and management of pain. LA ‘s are the only drugs that prevent the nociceptive impulse from reaching the patients brain [11] with the introduction of the first amide LA lidocaine HCL in 1948 providing profound anaesthesia of long duation became almost a certainity [12, 13] other amides introduced since 1948 include mepivacaine HCL, prilocaine HCL, bupivacaine HCL, etidocaine HCL and articaine HCL. Onset of pulpal anaesthesia commonly occurs within 5-10 minutes, persisting for approximately 60 minutes for articaine HCL, lidocaine HCL and mepicaine HCl formulations containing vasopressor [14, 15]. Local anaesthetics work, if deposited in close proximity to the nerve, they will block the nerve conduction.
However LA suffer a number of drawbacks [16, 17, 18];
- containing a vasopressor - sting on injection
- they are associated with a degree of post injection tissue injury
- LA have relatively slow onset
- La do not work as reliably in the presence of infection and inflammation All these drawbacks can be addressed by anaesthetic buffering which;
- Eliminates the sting
- Reduces tissue injury
- Reduces latency
- Introduces the independent anaesthetic effect of carbon di oxide Introduces the catalytic effect of carbon di oxide Chemistry and anaesthetic latency: To achieve pulpal anaesthesia two things must happen:
- The practitioner must deposit LA in close proximity to the nerve
- LA must cross the nerve membrane to block the sodium channels at present the first requirement is met through the injection technique. However without modification the anaesthetic ability to cross the nerve membrane is dependant on biochemical processes that are out of practitioners control. Thus with alkalinisation there is an alteration of biochemical process, thereby enhances the anaesthetic efficacy [19, 20, 21].
Sodium bicarbonate is a systemic alkalinising agent. It increases the plasma bicarbonate concentration, buffers excess hydrogen ions, and raises the pH of the blood, thereby reversing clinical signs of acidosis [4]. We used sodium bicarbonate to increase the pH of the local anaesthetic solution to a more physiological pH [22].
Importance of pH of the Local Anaesthetic Solution
Commercially available 2% lignocaine with 1:80,000 adrenaline solutions have a low pH (3.3). Although reducing the pH extends the shelf life of the solution to around 36 months, and prevents the early oxidation of adrenaline, the solution is more likely to produce a burning sensation on injection and a slower onset of anaesthesia [5].
Increasing the pH of the local anaesthetic solution speeds the onset of its action [5], increases its effectiveness, and makes the injection more comfortable. Alkalinising or increasing the pH of the solution can be achieved by adding sodium bicarbonate.
This increases the free base form of the lignocaine molecule and alkalinises the solution, thereby reducing the pain during injection.
We added 7.5 % sodium bicarbonate to local anaesthetic solution in a dilution of 1/10 [6]. This reduced the pH from 3.05 to 7.38,7.4 to 7.8 which caused the availability of the lipophilic uncharged lidocaine molecules (RN), also called the base, to be more available for diffusion into the membrane of the nerve as the solution was close to the physiological tissue pH of 7.4. When sodium bicarbonate is added it is also available in the tissues as bicarbonate ion, which alkalinises the extracellular pH [23, 24, 25, 26]. When extracellular pH is increased by the addition of bicarbonate, the decreased intracellular pH (through diffusion of carbon dioxide produced from the reaction of hydrogen and hydrogen carbonate in extracellular fluid) It also play a part in increasing the effect of the local anaesthetic block through protonation of intracellular free-base local anaesthetic (“ion trapping”) and increasing the concentration gradient for the free-base local anaesthetic across the plasma membrane [8, 27].
Onset of Anaesthesia
The mean time of onset of anaesthetic effect for lignocaine is 332.12 seconds articaine 185.92 sec, buffered articaine 339.52 sec, buffered lignocaine 239.66 sec. The latency, duration of anaesthetic effect of an anaesthetic solution depends on a number of factors such as intrinsic properties of the drug substance used and anesthetic technique employed [28, 29, 30]. In this study all the patients were administered inferior alveolar nerve block with the classical technique using landmark based technique described by Malamed [31].
Other factors also affect the onset and duration of LA including the affinity of local anaesthetic to the lipid and protein components within the nerve membrane, the intrinsic vasodilating activity of local anaesthetic, the presence or absence of a vasoconstrictor in the solution and the vascularity of the injection site [32, 33, 34, 35]. With alkalinisation the free base form of the local anaesthetic agent is more lipid-soluble, and so diffuses quickly into the membrane of the nerve [36]. The cytoplasm was acidified by the membrane-permeating carbon dioxide leading to the intracellular “trapping” of the cationic form of the local anaesthetic agent. Increasing the extracellular pH with a constant extracellular concentration of local anaesthetic results in a greater intracellular concentration of local anaesthetic and more complete inhibition of sodium currents, whether or not the intracellular carbon dioxide concentration or pH changes [37]. When extracellular pH is increased by the addition of bicarbonate, decreased intracellular pH through diffusion of carbon dioxide may also have a role in increasing the local anaesthetic block. Sodium bicarbonate ions also nonspecifically reduce the margin of safety for nerve conduction, and may have a direct action on the binding of the local anaesthetic to the sodium channel [26, 27, 38].
Duration of Anaesthesia
The mean time of duration of anaesthetic effect for lignocaine is 158.64 seconds articaine 215.49 sec, buffered articaine 195.94 sec, buffered lignocaine 275.74 sec according to anova test.
Duration of anesthetic effect of an anesthetic solution is proportional to its degree of protein binding [39, 40]. Articaine presents one of the greatest protein binding percentages of all amide local anesthetics, comparable only to ultra-long action substances such as bupivacaine, ropivacaine and ethidocaine. Mean duration of anesthetic effect for 4%articaine was 215.49 minutes and mean duration of anesthetic effect for 2% lignocaine was 158.64 minutes, the buffered 4% articaine is 195.94 and for buffered 2% lignocaine was 275.74. Increased duration of anesthetic effect gives comfort to the patient postoperatively. Latency and duration of anesthetic effect for buffered lignocaine was both clinically and statistically significant when compare to the other three groups using tukey post hoc test.
Conclusion
This study compares the anesthetic efficacy of 4% articaine, 2% lignocaine, 4% buffered articaine and 2% buffered articaine with epinephrine. Onset, duration of anesthetic effect were compared. We conclude that 4% articaine has faster onset when compared to the other three groups. Buffered lignocaine had significantly longer duration when compared to the other groups. This can be explained based on its different chemical structure, liposolubility, increased protein binding ability, diffusion in soft tissue and increased pulpal anesthesia.
References
-
Leonard M (1998) Carl Koller: Mankind’s Greatest Benefactor? The Story of Local Anesthesia. Journal of Dental Research 77(4): 535-538.
-
Liljestrand G (1967) Carl Koller and the Development of Local Anesthesia. Acta Physiologica Scandinavica. Supplementum 71(299): 1-30.
-
Schabes GA (1978) Monheim’s Local Anesthesia and Pain Control in Dental Practice. Anesth Prog 25(4): 132.
-
Goerig M, Bacon D, van Zundert A (2012) Carl Koller, cocaine, and local anesthesia: some less known and forgotten facts. Reg Anesth Pain Med 37(3): 318-324.
-
Hadda SE (1962) Procaine: Alfred Einhorn’s ideal substitute for cocaine. The Journal of the American Dental Association 64(6): 841-845.
-
Kashyap VM, Desai R, Reddy PB, Menon S (2011) Effect of alkalinisation of lignocaine for intraoral nerve block on pain during injection, and speed of onset of anaesthesia. Br J Oral Maxillofac Surg 49(8): 72-75.
-
Wang YH, Wang DR, Liu JY, Pan J (2021) Local anesthesia in oral and maxillofacial surgery: a review of current opinion. J Dent Sc 16(4): 1055-1065.
-
Elicherla SR, Sahithi V, Saikiran KV, Nunna M, Challa RR, et al. (2021) Local Anesthesia in Pediatric Dentistry: A Literature Review on Current Alternative Techniques and Approaches. Dent 4(2): 148-154.
-
Adewumi A, Hall M, Guelmann M, Riley J (2008) The incidence of adverse reactions following 4% septocaine (articaine) in children. Pediatr Dent 30(5): 424-428.
-
Becker DE, Reed KL (2012) Local Anesthetics: Review of Pharmacological Considerations. Anesth Prog 59(2): 90-101.
-
Brunetto PC, Ranali J, Bovi Ambrosano GM, de Oliveira PC, Groppo FC, et al. (2008) Anesthetic Efficacy of 3 Volumes of Lidocaine with Epinephrine in Maxillary Infiltration Anesthesia. Anesth Prog 55(2): 29-34.
-
Jack (2004) Handbook of local anesthesia malamed 5th (Edn.), mosby pdf.
-
Dunsky JL (1997) Alfred Einhorn: the discoverer of procaine. J Mass Dent Soc 46(3): 25-26.
-
Costa CG, Tortamano IP, Rocha RG, Francischone CE, Tortamano N (2005) Onset and duration periods of articaine and lidocaine on maxillary infiltration. Quintessence Int 36(3): 197-201.
-
Doğan N, Uçok C, Korkmaz C, Uçok O, Karasu HA (2003) The effects of articaine hydrochloride on wound healing: an experimental study. J Oral Maxillofac Surg 61(12): 1467-1470.
-
Haas DA, Harper DG, Saso MA, Young ER (1990) Comparison of articaine and prilocaine anesthesia by infiltration in maxillary and mandibular arches. Anesth Prog 37(5): 230-237.
-
Hersh EV, Giannakopoulos H, Levin LM, Secreto S, Moore PA, et al. (2006) The pharmacokinetics and cardiovascular effects of high-dose articaine with 1:100,000 and 1:200,000 epinephrine. J Am Dent Assoc 137(11): 1562-1571.
-
Jakobs W, Ladwig B, Cichon P, Ortel R, Kirch W (1995) Serum levels of articaine 2% and 4% in children. Anesth Prog 42(3-4): 113-115.
-
Potočnik I, Tomšič M, Bajrović F (2001) Sensitivity of sensory axons to lidocaine nerve block in rats. Pflugers Archiv 442(1): 193-194.
-
Robertson D, Nusstein J, Reader A, Beck M, McCartney M (2007) The anesthetic efficacy of articaine in buccal infiltration of mandibular posterior teeth. J Am Dent Assoc 138(8): 1104-1112.
-
Srinivasan N, Kavitha M, Loganathan CS, Padmini G (2009) Comparison of anesthetic efficacy of 4% articaine and 2% lidocaine for maxillary buccal infiltration in patients with irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 107(1): 133-136.
-
Gregorio LVL, Giglio FPM, Sakai VT, Modena KCS, Colombini BL, et al. (2008) A comparison of the clinical anesthetic efficacy of 4% articaine and 0.5% bupivacaine (both with 1:200,000 epinephrine) for lower third molar removal. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106(1): 19-28.
-
Mikesell P, Nusstein J, Reader A, Beck M, Weaver J (2005) A Comparison of Articaine and Lidocaine for Inferior Alveolar Nerve Blocks. J Endod 31(4): 265-270.
-
Moore PA, Doll B, Delie RA, Hersh EV, Korostoff J, et al. (2007) Hemostatic and anesthetic efficacy of 4% articaine HCl with 1:200,000 epinephrine and 4% articaine HCl with 1:100,000 epinephrine when administered intraorally for periodontal surgery. J Periodontol 78(2): 247-253.
-
Oertel R, Rahn R, Kirch W (1997) Clinical pharmacokinetics of articaine. Clin Pharmacokinet 33(6): 417-425.
-
Arif A, Riaz B, Bhatti AM, Sherwani NZ, Khan R, et al. (2021) Effect of Buffered Local Anesthesia on Perioperative Pain During Arteriovenous Fistula Surgery: A Randomized Control Trial. Cureus 13(5): e15202.
-
Aulestia Viera PV, Braga MM, Borsatti MA (2018) The effect of adjusting the pH of local anaesthetics in dentistry: a systematic review and meta‐analysis. Int Endod J 51(8): 862-876.
-
Oliveira PC, Volpato MC, Ramacciato JC, Ranali J (2004) Articaine and lignocaine efficiency in infiltration anaesthesia: a pilot study. Br Dent J 197(1): 45-46.
-
Ozdemir M, Ozdemir G, Zencirci B, Oksuz H (2004) Articaine versus lidocaine plus bupivacaine for peribulbar anaesthesia in cataract surgery. Br J Anaesth 92(2): 231-234.
-
Pabst L, Nusstein J, Drum M, Reader A, Beck M (2009) The efficacy of a repeated buccal infiltration of articaine in prolonging duration of pulpal anesthesia in the mandibular first molar. Anesth Prog 56(4): 128-134.
-
Malamed SF, Tavana S, Falkel M (2013) Faster onset and more comfortable injection with alkalinized 2% lidocaine with epinephrine 1:100,000. Compend Contin Educ Dent 1: 10-20.
-
Steele EA, Ng JD, Poissant TM, Campbell NM (2009) Comparison of injection pain of articaine and lidocaine in eyelid surgery. Ophthalmic Plast Reconstr Surg 25(1): 13-15.
-
Tófoli GR, Ramacciato JC, de Oliveira PC, Volpato MC, Groppo FC, et al. (2003) Comparison of effectiveness of 4% articaine associated with 1: 100,000 or 1: 200,000 epinephrine in inferior alveolar nerve block. Anesth Prog 50(4): 164-168.
-
Vahatalo, K., Antila, H, Lehtinen R (1993) Articaine and lidocaine for maxillary infiltration anesthesia. Anesth Prog 40(4): 114-116.
-
Vree TB, Gielen MJM (2005) Clinical pharmacology and the use of articaine for local and regional anaesthesia. Best Pract Res Clin Anaesth 19(2): 293-308.
-
Whitcomb M, Drum M, Reader A, Nusstein J, Beck M (2010) A Prospective, Randomized, Double-Blind Study of the Anesthetic Efficacy of Sodium Bicarbonate Buffered 2% Lidocaine With 1: 100,000 Epinephrine in Inferior Alveolar Nerve Blocks. Anesth Prog 57(2): 59- 66.
-
Davies RJ (2003) Buffering the pain of local anaesthetics: A systematic review. Emerg Med (Fremantle, W.A.), 15(1): 81-88.
-
Strazar AR, Leynes PG, Lalonde DH (2013) Minimizing the pain of local anesthesia injection. Plast Reconstr Surg 132(3): 675-684.
-
Evans G, Nusstein J, Drum M, Reader A, Beck M (2008) A prospective, randomized, double-blind comparison of articaine and lidocaine for maxillary infiltrations. J Endod 34(4): 389-393.
-
Wright GZ, Weinberger SJ, Friedman CS, Plotzke OB (1989) Use of articaine local anesthesia in children under 4 years of age--a retrospective report. Anesth Prog 36(6): 268-271.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells