Clinical, Radiographic, and Histopathologic Evaluation of Multiple, Non-Syndromic Hyperplastic Dental Follicles: A Unique Pediatric Case Report
Background: Hyperplastic Dental Follicle (HDF) is a hamartomatous oral lesion. HDF is characterized by the presence of fibromyxomatous connective tissue with nests and strands of odontogenic epithelial rests. HDF are infrequently reported and only accounts for 5-6% of all the pediatric jaw lesions that are biopsied. The mean age of HDF finding has been reported to be around 19 years. HDF is commonly associated with syndrome; however, non-syndromic HDF is rarely reported. HDF commonly affects posterior teeth and the canines. Description: Here, we presented a non-syndromic pediatric case with multiple HDF affecting canines and one premolar in an eight-year-old Hispanic female with three-year follow-up. The medical and dental history for the patient was non-contributory. A routine panoramic radiograph demonstrated multiple unilocular radiolucencies affecting all permanent canines and lower left second premolar. One of the mandibular canines spontaneously resolved while the contralateral canine needed surgical intervention. This case report provides a comprehensive literature review on HDF. Conclusion: Timely diagnosis, shorter follow-ups, and surgical intervention are key for management of HDF to allow for normal tooth eruption and the prevention of adjacent tooth displacement and root resorption.
Introduction
Hyperplastic Dental Follicle (HDF) is a hamartomatous oral lesion. HDF is characterized by fibromyxomatous connective tissue with nests and strands of odontogenic epithelial rests [1, 2]. Gardner first attempted to classify these lesions [1, 3]. HDF accounts for 5-6% of all the pediatric lesions submitted for biopsy [4]. The mean age of occurrence of HDF is around 19 years [4, 5]. There are very few pediatric cases of HDF reported in the literature [5, 6, 7, 8]. Sun CX, et al. reported that HDF may have a familial tendency thereby suggesting a genetic predilection [7]. While the HDF is associated with an unerupted tooth, the causes of which are uncertain, but have been attributed to endocrinal disturbances, metabolic disease, muscle pressure, febrile disease, inflammation, and vitamin D deficiency [9].
HDF is often associated with syndromes such as Gardner syndrome [5], Lowe syndrome [10], amelogenesis imperfecta [11], enamel renal syndrome [12], cleidocranial dysplasia [5], Noonan syndrome [5], and mucopolysacaridosis [5]. Non-syndromic HDF is rarely reported so the true incidence is unknown. Except for third molar involvement, multiple non-syndromic HDFs appear to be very rare in a young child [7]. HDF most frequently affects posterior teeth (molars or premolars) while canines and incisors are less frequently involved [5]. Therefore, non-syndromic HDF affecting multiple canines in a pediatric patient is rarely found in the literature. The occurrence of HDF in maxilla and mandible is comparable [5]. HDFs are often detected on routine panoramic radiographs [5, 7, 8, 11, 12, 13, 14, 15, 16] or periapical radiographs [5, 6, 17]. Normal radiolucency around an erupting tooth is about 1-3 mm wide; however, the radiolucency around an HDF affected tooth is more than 3 mm wide [7] and is often a sign of pathologic change [18, 19].
Radiographically, lesions that show a radiolucency associated with unerupted tooth, like HDF, are dentigerous cyst, odontogenic keratocyst, ameloblastic fibroma and unicystic ameloblastoma. Because small foci of dystrophic calcification are associated with some entities, especially those described as calcifying HDF, the calcifying odontogenic cyst, adenomatoid odontogenic tumor, ameloblastic fibro- odontoma, and calcifying epithelial odontogenic tumor are included in the differential diagnosis [14]. It is especially challenging to differentiate between a HDF developing around a tooth crown and a dentigerous cyst. A cyst should be considered with any evidence of tooth displacement or expansion of the bone or with asymmetric enlargement of the follicle. If uncertainty remains, the region should be re- examined in 4 to 6 months to detect any increase in shape or influence on surrounding structures characteristic of cysts [23]. HDF is often treated with curettage of the pericoronal tissue with or without extraction of the affected tooth. The potential differential diagnoses of HDF based on clinical and radiographic findings are presented in table 1. In this report, we present a non-syndromic, pediatric case with HDF affecting all permanent canines and one premolar with conservative management and three-year follow-up.
| Category | Conditions |
|---|---|
| Developmental Lesions | Hyperplastic dental follicle (single or multiple) |
| Calcifying hyperplastic dental follicle (single or multiple) | |
| Odontogenic Cysts | Dentigerous cyst |
| Odontogenic keratocyst | |
| Eruption cyst | |
| Buccal bifurcation cyst | |
| Calcifying odontogenic cyst | |
| Glandular odontogenic cyst | |
| Odontogenic Tumors | Unicystic ameloblastoma |
| Ameloblastic Fibroma | |
| Adenomatoid odontogenic tumor | |
| Odontoma | |
| Calcifying epithelial odontogenic tumor | |
| Odontogenic Myxoma | |
| Central odontogenic fibroma | |
| Ameloblastic fibro-odontoma | |
| Squamous odontogenic tumor | |
| Primordial odontogenic tumor | |
| Other Neoplasms | Melanotic neuroectodermal tumor of infancy |
| Intraosseous mucoepidermoid carcinoma | |
| Genetic conditions | Amelogenesis imperfecta |
| Hereditary gingivofibromatosis | |
| Enamel renal syndrome | |
| Lowe syndrome | |
| Gardner syndrome | |
| Cleidocranial dysplasia | |
| Nevoid basal cell carcinoma syndrome | |
| Noonan syndrome | |
| Mucopolysaccharidosis | |
| Cherubism | |
| Pycnodysostosis |
Table 1: In this report, we present a non-syndromic, pediatric case with HDF affecting all permanent canines and one premolar wit
Case Report
An eight-year-old Hispanic female with non-contributory medical, family, and dental history reported for routine dental examination at the Children’s Hospital Colorado’s Pediatric Dental Clinic. No identifying information for the patient has been included in the case-report. Patent’s height was 60th percentile, weight was 90th percentile, and the body mass index was over 99th percentile for her age. She was on cetirizine for environmental allergies.
Clinical and Radiographic Description
Patient reported for six-month recall dental examination.
A routine panoramic radiograph at age 8 revealed multiple unilocular pericoronal radiolucencies around all permanent canines #13, #23, #33, #43, and lower left second premolar #35 (Figures 1A-C). Patient was asymptomatic with clinically undetectable bony expansion, and the surrounding alveolar mucosa around #13, #23, #33, #35, and #43 was intact. The alveolar mucosa around the affected teeth was of the same color as the surrounding soft tissues without any pain, tenderness, or bleeding. Hence, no clinical photographs are provided with this case report. Since the radiolucency was more than 3 mm surrounding the unerupted teeth (#13, #23, #33, #35, and #43), quarterly clinical and biannual radiographic follow-ups were recommended.
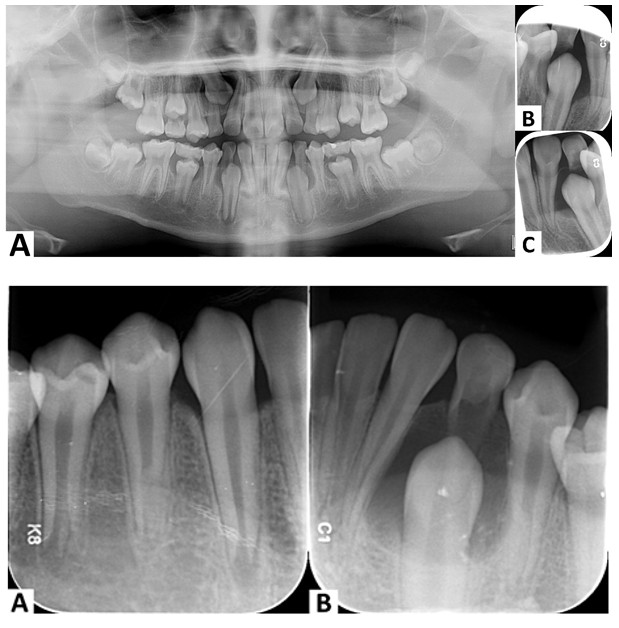
Figure 1A-C: Routine panoramic radiograph (A) and periapical radiograph of right and left mandibular canine region taken at age 8 demonstrating unilocular pericoronal radiolucent lesions surrounding all permanent canines and lower left second premolar indicating multiple hyperplastic dental follicles affecting canines and one premolar.
Figure 2A & B: Periapical radiograph of right (A) and left (B) canine-premolar region demonstrating resolution of right canine and left second premolar while lower left canine demonstrated unilocular radiolucency with sclerotic borders and evidence of resorption of lower left primary canine and mild displacement of roots of lower left lateral incisor and first premolar.
At 10 years of age, #43 and #35 were erupted but #33 was neither erupted nor its canine eminence could be clinically detected. There was radiographic evidence of partial root resorption of #73 with a well-defined radiolucency around unerupted #33 was still present with mild displacement of #32 and #34 (Figures 2A & B). An oral pathology consult was obtained with a differential diagnosis of HDF, dentigerous cysts, and odontogenic keratocyst. An oral and maxillofacial pathologist (CF) confirmed our findings and differential diagnosis with a recommendation for extraction of #73 and curettage of pericoronal tissue for histopathologic evaluation. Extraction of #73 was done under local anesthesia and nitrous oxide-oxygen anxiolysis and the resected pericoronal tissue (3mmX3mmX1mm) was submitted for histopathologic evaluation.
Microscopic Description
Hematoxylin-eosin-stained sections demonstrated thick and thin fragments of edematous and variably dense fibromyxomatous connective tissue containing scattered nests and strands of inactive odontogenic epithelium. Some of the tissue fragments were lined by reduced enamel epithelium ranging from columnar to cuboidal epithelial cells (Figures 3A & B). There was a focally prominent chronic inflammation within the connective tissue. The microscopic examination confirmed the diagnosis of HDF. Tooth #33 erupted normally after the extraction of #73. Clinical and radiographic follow-up was recommended to monitor eruption of #13 and #23 in the future.
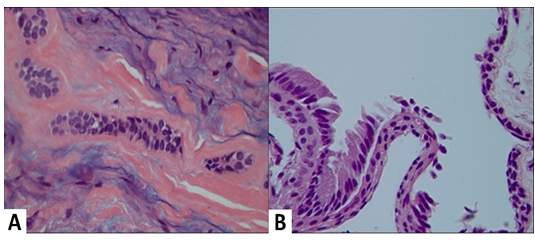
Figure 3A & B: High-power (400X), hematoxylin-eosin-stained photomicrographs of the hyperplastic dental follicle. A: Exhibits fibromyxomatous connective tissue with hyalinized induction around the nests and strands of inactive odontogenic rests. B: Highlights the epithelial lining of reduced enamel epithelium, ranging from tall columnar ameloblastic cells to flattened cuboidal cells.
Discussion
Tooth eruption is a highly orchestrated process [23, 24]. The osteoclastic removal of the bone overlying the erupting tooth and enzymatic lysis of the connective tissue is required for clearing the path of erupting tooth [25]. Prior to the eruption of the tooth, the enamel epithelium reduces and undergoes atrophy coronal to the tooth. Later, the connective tissue between oral epithelium and reduced enamel epithelium is broken down. This process is altered by fibromyxomatous hyperplasia in the connective tissue thereby, leading to the potential failure of tooth eruption [6]. Fibrous hyperplasia of the connective tissue is a classic histopathologic sign of HDF [6]. Various hypotheses for the fibrous hyperplasia has been presented including impacted tooth, presence of supernumerary tooth, chronic inflammation, and infection [6]. One study presented a strong association of impacted tooth with HDF [6]. Unerupted or impacted teeth can be seen in conditions such as endocrinal disturbances, metabolic disorders, vitamin D deficiency, and localized disturbances in the jaw [6]. Another study demonstrated that several collagen genes (Col I, IV, VIII, and XI and TIMP 1,2, and 4) were two-fold upregulated in the HDF, while the expression of matrix metalloproteinases (1, 2, 10, and 16) and interleukin 8 were two-fold downregulated [26]. Hence, the defective regulation of matrix metalloproteinases mediating connective tissue remodeling may be the underlying cause for fibrous hyperplasia leading to the abnormal tooth eruption, and resultant HDF. Since Kim SG, et al. presented information from a single individual, there is lack of comprehensive and reproducible evidence about the role of collagen metabolism in the process of tooth eruption and its association with HDF [26]. An abnormal osteoclastic function impeded tooth eruption in osteoporotic rats [27]. Ge J, et al. reported that as compared to normal pericoronal tissue, the tissue from HDF demonstrated lower osteogenic, osteoclastic, and matrix-degrading potential with lower RUNX Family Transcription Factor 2, which is involved in the development of hard tissues such as teeth, bones and cartilage [28]. Additionally, disproportionate expression of the receptors involved in bone remodeling (such as receptor activator of the nuclear factor kappa-B ligand and the decoy receptor osteoprotegerin) and decreased expression of matrix metalloproteinase 2 and 9, would lead to inactivation of osteoclasts and suppression of bone matrix remodeling in HDF cases [28]. It is important to note that impacted tooth eruption is often associated with syndromes [29], non- syndromic eruption disorders involving multiple teeth in a child are rarely reported [30]. Of interest, our case of multiple HDFs developed in a child who had a body mass index of 99th percentile for her age. It has been demonstrated that there is an association with obesity in children and accelerated tooth eruption [31]. It is interesting to speculate that in some children, meta-inflammation may influence the development of enlarged follicles due to an increase in inflammatory cytokines, chronic inflammation, edema, and subsequent fibrosis [31, 32]. Further studies are needed to determine if this is a potential marker for metabolic syndrome in the pediatric population.
HDF is often asymptomatic and may show mild expansion in the affected area [6]. In our case, the finding of HDF was incidental on routine panoramic radiograph and no swelling of the area was appreciated clinically. Radiographically, HDF presents as a well circumscribed unilocular radiolucency around an impacted tooth [6]. Slight resorption of adjacent tooth roots or speckled radiopacities of the lesions can be detected on radiographs [6], as the cells of dental follicles can give rise to the cementum, alveolar bone and periodontal ligaments. Hence, in some cases, HDF may demonstrate dystrophic calcification within the follicle, especially adjacent to the nests of odontogenic epithelium [3, 6]. If calcified material is abundantly present in the connective tissue then the HDF lesion is also known as calcified hyperplastic dental follicle [33]. Calcifications have been reported in about 25- 40% of HDF cases [8, 34]. Radiographic differential diagnosis for radiolucent cases without calcifications, such as the present example, includes dentigerous cyst, odontogenic keratocyst, and ameloblastic fibroma [5, 6, 17, 19, 20].
Microscopically, HDF lesions show fragments loosely or densely arranged connective tissue containing odontogenic epithelial rests scattered among the delicate or mature collagen fibrils with or without myxomatous change and inflammation. In our case, similar microscopic findings were noted. Due to these histopathologic findings, HDF can often be confused with odontogenic fibroma, myxoma, myxofibroma and ameloblastic fibroma [13, 19]. Within the fibrous connective tissue, epithelial components in HDF have been reported to be of three types: reduced enamel epithelium, remnants of dental lamina, and scattered odontogenic epithelial rests [6]. Epithelial cells in reduced enamel epithelium are columnar or cuboidal with pyknotic nuclei and eosinophilic cytoplasm [6]. Cells of the remnants of dental lamina are round in shape with round nuclei and pale cytoplasm [6]. Scattered odontogenic epithelial rests have been reported in the majority of the lesions with vacuolar degeneration and occasional keratinization [6]. Microscopically, the calcified areas were seen with osteodentin, cementum, psammomatous calcification, or Liesegang ring-like structures [8, 11, 15, 17, 35].
Fukuta Y, et al. in 1991, reported 11 cases of HDF of which only four were adolescent cases and only one was reported in a pediatric patient [6]. Cho YA, et al. reported two pediatric and three adolescent cases of multiple calcifying HDF and reviewed previously reported two pediatric and 6 adolescent cases [8]. Schmitd LB, et al. reviewed 12 studies with 18 cases of HDF, of which only three cases of HDF involved all four canines [17]. The same study reported only six pediatric HDF cases, while the rest were in adolescents or adults [17]. Sun CX, et al. reviewed eight reported cases with only one pediatric and three adolescent cases [7]. Some studies reported HDF has no sex predilection [6] while other studies reported 1-4.7 times higher incidence in males [5, 17]. HDF may demonstrate as multiple symmetrical lesions with unerupted teeth or as an unilateral finding with contralateral tooth eruption [6]. All of these study findings supports that our non-syndromic pediatric HDF case in a female Hispanic patient affecting all permanent canines is rarely reported. Furthermore, there are no reported cases evaluating the ethnic or racial predilection of HDF in humans or the role that obesity may play in the development of these odontogenic lesions.
Conclusion
Our case report demonstrated a rare non-syndromic HDF affecting all permanent canines in a pediatric female patient. Our case report also provides a comprehensive review of literature on HDF. We noted eruption of the permanent mandibular canine after primary canine extraction and removal of pericoronal tissue. This is the first reported case in the literature with over three-year clinical and radiographic follow-up. Implication for dentists:
- This case presents a rare, pediatric case of non- syndromic hyperplastic dental follicle affecting all permanent canines in a female patient.
- It is interesting to note that the canine affected with HDF demonstrated resolution with conservative surgical intervention only.
- This case report provides a comprehensive literature review including insights into potential causes, incidence, histopathologic findings, and management of hyperplastic dental follicles.
References
-
Gardner DG (1980) The central odontogenic fibroma: an attempt at clarification. Oral Surg Oral Med Oral Pathol 50(5): 425-432.
-
Rai DV (2019) Hyperplastic Dental Follicle with Calcification- A Case Report. Case Reports in Odontology 6(2): 1-4.
-
Gardner DG, Radden B (1995) Multiple calcifying hyperplastic dental follicles. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 79(5): 603-606.
-
Jones AV, Franklin CD (2006) An analysis of oral and maxillofacial pathology found in children over a 30-year period. Int J Paediatr Dent 16(1): 19-30.
-
Guardado LI, Haro AJ, Godinez RM, Puente de LSJA, Guirre MJ, et al. (2020) Multiple calcifying hyperplastic dental follicles: a major diagnostic consideration in multiple pericoronal lesions - report of two cases. BMC Oral Health 20(1): 159.
-
Fukuta Y, Totsuka M, Takeda Y, Yamamoto H (1991) Pathological study of the hyperplastic dental follicle. J Nihon Univ Sch Dent 33(3): 166-173.
-
Sun CX, Ririe C, Henkin JM (2010) Hyperplastic dental follicle - review of literature and report of two cases in one family. Chin J Dent Res 13(1): 71-75.
-
Cho YA, Yoon HJ, Hong SP, Lee JI, Hong SD (2011) Multiple calcifying hyperplastic dental follicles: comparison with hyperplastic dental follicles. J Oral Pathol Med 40(3): 243-249.
-
Bishara SE, Kommer DD, McNeil MH, Montagano LN, Oesterle LJ, et al. (1976) Management of impacted canines. Am J Orthod 69(4): 371-387.
-
Roberts MW, Blakey GH, Jacoway JR, Chen SC, Morris CR (1994) Enlarged dental follicles, a follicular cyst, and enamel hypoplasia in a patient with Lowe syndrome. Oral Surg Oral Med Oral Pathol 77(3): 264-265.
-
Roquebert D, Champsaur A, Gil del RP, Prasad H, Rohrer MD, et al. (2008) Amelogenesis imperfecta, rough hypoplastic type, dental follicular hamartomas and gingival hyperplasia: report of a case from Central America and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106(1): 92-98.
-
Molla MDL, Quentric M, Yamaguti PM, Acevedo AC, Mighell AJ, et al. (2014) Pathognomonic oral profile of Enamel Renal Syndrome (ERS) caused by recessive FAM20A mutations. Orphanet Journal of Rare Diseases 9(1): 84.
-
Chrcanovic BR, Freire MB, Gomez RS (2014) Small central odontogenic fibroma mimicking hyperplastic dental follicle and dentigerous cyst. J Maxillofac Oral Surg 13(3): 332-336.
-
Aydin U, Baykul T, Yildirim B, Yildirim D, Bozdemir E, et al. (2013) Multiple calcifying hyperplastic dental follicles: A case report. Imaging Sci Dent 43(4): 303-308.
-
Jamshidi S, Zargaran M, Mohtasham N (2013) Multiple Calcifying Hyperplastic Dental Follicle (MCHDF): A Case Report. J Dent Res Dent Clin Dent Prospects 7(3): 174- 176.
-
Desai RS, Momin YNA, Bansal S, Karjodkar FR (2017) Multiple Calcifying Hyperplastic Dental Follicles: A Case Report and Literature Review. J Oral Maxillofac Surg 75(8): 1702-1705.
-
Schmitd LB, Bravo CDM, Soares CT, Oliveira DT (2014) Hyperplastic dental follicle: a case report and literature review. Case Rep Dent 2014: 251892.
-
Walker LM, Wood AJ, McDonald A, Carpenter W (2004) Unerupted mandibular second primary molar with an unusual histopathological finding: a case report. J Dent Child (Chic) 71(1): 77-79.
-
Robinson RA (2017) Diagnosing the most common odontogenic cystic and osseous lesions of the jaws for the practicing pathologist. Mod Pathol 30(s1): S96-S103.
-
Bilodeau EA, Hunter KD (2021) Odontogenic and Developmental Oral Lesions in Pediatric Patients. Head Neck Pathol 15(1): 71-84.
-
Rajabi MM, Mozafari G, Abbaszadeh H (2022) Central odontogenic fibroma, hyperplastic dental follicle, or dentigerous cyst? A diagnostic dilemma: A case report. Clin Case Rep 10(7): e6163.
-
Neville B, Damm D, Allen C, Chi A (2016) Oral and Maxillofacial Pathology. 4th (Edn.), Elsevier.
-
Mallya SM, Lam EWN (2019) White and Pharoah’s Oral Radiology. In: Mallya SM (Eds.). Principles and Interpretation. 8th (Edn.), Elsevier.
-
Takahashi A, Nagata M, Gupta A, Matsushita Y, Yamaguchi T, et al. (2019) Autocrine regulation of mesenchymal progenitor cell fates orchestrates tooth eruption. Proc Natl Acad Sci USA 116(2): 575-580.
-
Park SJ, Bae HS, Cho YS, Lim SR, Kang SA, et al. (2013) Apoptosis of the reduced enamel epithelium and its implications for bone resorption during tooth eruption. J Mol Histol 44(1): 65-73.
-
Kim SG, Kim MH, Chae CH, Jung YK, Choi JY (2008) Downregulation of matrix metalloproteinases in hyperplastic dental follicles results in abnormal tooth eruption. BMB Rep 41(4): 322-327.
-
Marks SC (1981) Tooth eruption depends on bone resorption: experimental evidence from osteopetrotic (ia) rats. Metab Bone Dis Relat Res 3(2): 107-115.
-
Ge J, Guo S, Fu Y, Zhou P, Zhang P, et al. (2015) Dental Follicle Cells Participate in Tooth Eruption via the RUNX2-MiR-31-SATB2 Loop. J Dent Res 94(7): 936-944.
-
De Coster PJ, Verbeeck RMH, Holthaus V, Martens LC, Vral A (2006) Seckel syndrome associated with oligodontia, microdontia, enamel hypoplasia, delayed eruption, and dentin dysmineralization: a new variant? J Oral Pathol Med 35(10): 639-641.
-
Yildirim D, Yilmaz HH, Aydin U (2004) Multiple impacted permanent and deciduous teeth. Dentomaxillofac Radiol 33(2): 133-135.
-
Must A, Phillips SM, Tybor DJ, Lividini K, Hayes C (2012) The association between childhood obesity and tooth eruption. Obesity (Silver Spring) 20(10): 2070-2074.
-
Singer K, Lumeng CN (2017) The initiation of metabolic inflammation in childhood obesity. J Clin Invest 127(1): 65-73.
-
Sandler HJ, Nersasian RR, Cataldo E, Pochebit S, Dayal Y (1988) Multiple dental follicles with odontogenic fibroma-like changes (WHO type). Oral Surg Oral Med Oral Pathol 66(1): 78-84.
-
Suarez PA, Batsakis JG, El Naggar AK (1996) Don’t confuse dental soft tissues with odontogenic tumors. Ann Otol Rhinol Laryngol 105(6): 490-494.
-
Gomes VR, Melo MCS, Carnei HC, Pinho JET, Teixeira MA (2019) Hyperplastic dental follicle: case report. Jornal Brasileiro de Patologia e Medicina Laboratorial 55(3): 315-320.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells