Central Odontogenic Fibroma of Mandible: A Rare Case Report with Review of Literature
Central Odontogenic fibroma is an extremely rare neoplasm that develops from mature fibrous connective tissue with varying amounts of odontogenic epithelium. Its incidence is 0.1% of all odontogenic tumors. It occurs with equal frequency in the maxilla and mandible with female predominance. Two clinical variants are known: intraosseous or central and extraosseous or peripheral odontogenic fibroma. It is radiolucent and may present as a well-defined unilocular or multilocular slow-growing mass. Here we reported a case of central odontogenic fibroma in 44-year-old male in the posterior region of left mandible. We present this case because of its rarity.
Introduction
Odontogenic fibroma is a rare benign tumor of ectomesenchymal origin and it is poorly characterized out of all the tumours of odontogenic origin [1, 2, 3]. The tumor consists of strands or islands of inactive-looking odontogenic epithelium with or without evidence of calcification. Odontogenic fibroma was mentioned first time in WHO 1971 but its classification underwent changes only recently since 2017 where the lesions are distinguished based on their location (central or peripheral) not on histological basis anymore [4]. It is often asymptomatic and may be discovered incidentally during a routine dental examination [5]. Odontogenic fibroma sometimes radiographically presents as a radiolucent expansile multilocular tumor resembling ameloblastoma [5]. Given its rarity and radiolucent nature it is often clinically misdiagnosed as odontogenic cysts and tumors such as an odontogenic keratocyst, ameloblastoma, odontogenic myxoma and ameloblastic fibroma. Therefore, it is important to correctly identify and distinguish these tumors from other radiolucent neoplastic lesions including malignant ones.
A 44-year-old male came to the oral and maxillofacial surgery outpatient department with swelling present over the left lower jaw since 20 years. He noticed that the swelling was gradually increasing in size for the past 8 months. On external examination, there is no facial asymmetry. On intraoral examination, an expansile lesion is noted in the symphysis of alveolar process of the left mandible with absent left canine, 1st and 2nd premolar teeth (Figure 1).
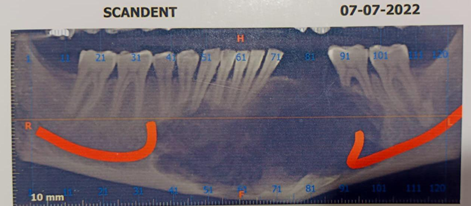
Clinical diagnosis was malignant tumor of odontogenic epithelium. PET CT revealed a lytic expansile lesion noted in the body and the alveolar process of the mandible showing a diffuse low-grade metabolism. No area of intense focal metabolism was noted thus ruling out the possibility of high-grade disease or malignant transformation. CECT Brain study revealed a solitary 2.1 x 4.7 x 2.7cm sized expansile lesion noted in the symphysis of the alveolar process of the mandible with resultant cortical thinning. There is no associated impacted tooth. There is no evidence of post- contrast enhancement. Few focal bony erosion are noted in the alveolar process of left hemi-mandable with absent dentition (left canine, 1st and 2nd premolar in lower jaw). There is no evidence of any extra mandibular extension seen (Figure 2).


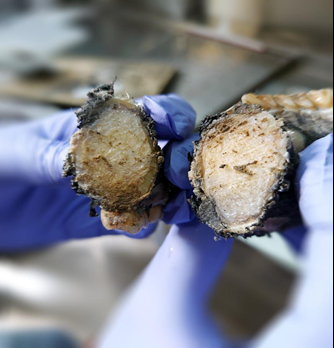
Biopsy was done which showed a paucicellular spindle cell lesion with abundant collagenised stroma. No epithelial cells were seen in the material. On immunohistochemistry, the spindle cells are negative for SMA, AE1/AE3, S100, B-catenin. MIB1 labelling is <1%. So the diagnosis of low grade spindle cell lesion was given and the possibility of odontogenic fibroma was considered. Left segmental mandibulectomy was performed. We received left segmental mandibulectomy specimen measuring 6.5cm along lower alveolus (Figure 3).
A single intraosseous firm to bony hard expansile lesion is identified, measuring 3 x 3 x 2 cm. The cut section of the tumor is grey-white, solid, homogenous and firm to hard in consistency (Figure 4).
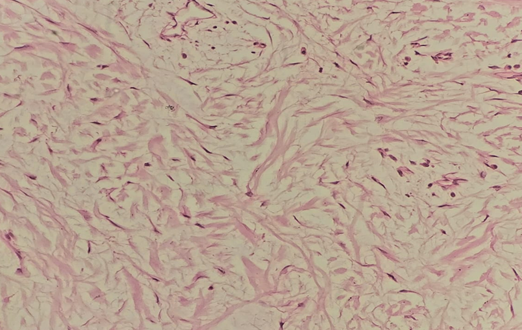
Microscopic examination showed a well-circumscribed tumor composed of moderately cellular mature fibrous connective tissue. The connective tissue stroma shows loosely arranged fascicles of bland spindle to stellate cells.
Odontogenic epithelium was absent (Figure 5).
The differential diagnosis of Desmoplastic fibroma, odontogenic myxoma, ameloblastic fibroma, central giant cell tumor, fibrosarcoma, ameloblastoma and adenomatoid odentogenic tumour were considered. As the histopathological features in the present case were of a benign lesion and considering the radiographic, clinical and histopathological findings, the final diagnosis of Central Odontogenic Fibroma was made.
Discussion
Odontogenic fibroma is a rare mesodermal odontogenic tumor in the jawbone. The origin of the tumor might be from the periodontal ligament, dental follicle, or dental papilla [2, 6]. Odontogenic fibroma is often asymptomatic, painless and present with bony expansion and loosening of teeth. Smaller tumors are unilocular radiolucencies but larger tumors are mostly multilocular. Daley, et al. reported in a literature review a slight female predominance [7].
| Central odontogenic fibroma | Desmoplatic fibroma | Odontogenic myxoma | Ameloblastic fibroma | Adenomatoid odontogenic tumor | |
|---|---|---|---|---|---|
| Histopathology | Collagenous connective tissue with variable amounts of odontogenic epithelium [8-10]. | Whorled aggregates of densely collagenous tissue containing uniform spindled [14]. | Stellate and spindle- shaped cells in a rich myxoid or mucoid stroma with few collagen fibrils [15]. | Branching and anastomosing proliferative odontogenic epithelium with a peripheral rim of columnar cells [16]. | Variably sized solid nodules of cuboidal odontogenic epithelium and eosinophilic amorphous material called “tumor droplets” can be found [17,18]. |
| Presentation | Maxilla and mandible in equal proportions, being most affected posterior [8]. | Locally invasive and aggressive Almost mandible (84%), and in the posterior portion of both jaws [19]. | Locally invasive and aggressive Mandible (63%) at posterior region and maxilla at premolar region [15]. | Expansive growth of Mandible mostly posterior [16]. | The absence of a tooth is observed Maxilla (twice mandible) at anterior region [17,18]. |
| Radiology | Well-defined radiolucency, unilocular in smaller and multilocular in larger [20]. | Well-defined, almost multilocular radiolucency. more likely to involve bone expansion and boundary destruction [19]. | Multilocular as “honeycomb”, “soap bubble” or “tennis racket” aspect with well-defined borders [15]. | Well- defined, uni/ multilocular radiolucency, in most cases exhibiting a radiopaque boundary [16]. | unilocular radiolucency associated with the crown and often part of the root of an unerupted tooth, with a displacement of neighbouring teeth[17,18]. |
Table 1: We have considered all the similar lesions in the jaw as described before coming into the final diagnosis.
In 1980 Gardner was first to classify odontogenic fibroma in three different types [8]. Various classifications have been made on odontogenic fibroma over the years.
| Gardner, 1980 [8] | Hyperplastic dental follicle | Neoplasm with varying collagenous fibrous connective tissue containing nests of odontogenic epithelium simple type. | Complex or WHO-type lesion with dysplastic dentine or tissue like cementum, fibrous tissue with myxoid area and sparse or often conspicuous inactive looking odontogenic epithelium |
|---|---|---|---|
| Lukinmaa PL, et al. [11] Langlais, et al. [12]. | Simple type | Complex or WHO type | Granular cell type |
| WHO, 2005 [13] | Epithelium-poor type | Epithelium-rich type | |
| WHO, 2017 [4] | Intra-osseous or central | Extra-osseous or peripheral |
Table 2
Table 3 Tables 2 & 3: Summarizes the histological classifications put forth by Gardner [8], Lukinmaa PL, et al. [11], Langlais, et al. [12], WHO [13] (2005) classified OF as epithelium-poor type and epithelium rich type which was revised in 2017 as extraosseous or peripheral type and an intraosseous or central type which we have summarized.
Peripheral odontogenic fibroma is usually located as a solitary lesion arising mainly in the incisor-canine and premolar area on facial gingiva of the mandible. The underlying bone is uninvolved, and it rarely causes displacement of teeth. Peripheral odontogenic fibroma is more common than the central type [21, 22]. Histopathologically the tumour is characterized by myxomatous connective tissue, islands of odontogenic epithelium, dysplastic dentin, amorphous ovoid cementum-like calcifications and trabeculae of osteoid [23]. As the clinical and histological features of peripheral odontogenic fibroma do not match with our case, we excluded the diagnosis of peripheral odontogenic fibroma.
Central odontogenic fibroma appears as an asymptomatic expansion of the cortical plate of the mandible or maxilla. The most usual site of presentation in the mandible is the posterior area, while in the maxilla is the anterior region [4]. Histopathologically; central odontogenic fibroma is composed of moderately cellular or collagenous connective tissue with varying amounts of inactive-looking odontogenic epithelium in the form of islands or strands. The epithelium can vary from being totally absent to being a conspicuous feature. According to many pathologists the absence of odontogenic epithelium does not exclude the diagnosis of central odontogenic fibroma [8, 9, 10]. In spite of extensive sampling in our case odontogenic epithelium is not identified. Correlating with the histopathological findings of a well-circumscribed tumor composed of moderately cellular mature fibrous connective tissue with the clinical and radiological findings of expansile radiolucent bony lesion, we came to the conclusion that it is a rare case of Central odontogenic fibroma with absent odontogenic epithelium in a 44-year-old male patient. Treatment of central odontogenic fibroma typically involves surgical excision. Recurrence after surgical excision is rare, but close follow-up is recommended to ensure that the tumor does not recur [24].
Conclusion
In summary, central odontogenic fibroma is a rare benign tumor of the tooth-forming apparatus that is typically treated with surgical excision. Close follow-up is important to ensure that the tumor does not recur. Early diagnosis and treatment are important to prevent potential complications and ensure a favourable outcome.
References
-
Hrichi R, Gargallo AJ, Berini AL, Gay EC (2012) Central odontogenic fibroma: retrospective study of 8 clinical cases. Med Oral Patol Oral Cir Bucal 17: 50-55.
-
Hara M, Matsuzaki H, Katase N, Yanagi Y, Unetsubo T, et al. (2012) Central odontogenic fibroma of the jawbone: 2 case reports describing its imaging features and an analysis of its DCE-MRI findings. Oral Surg Oral Med Oral Pathol Oral Radiol 113(6): 51-58.
-
Lin HP, Chen HM, Vu CH, Yang H, Kuo RC, et al. (2011) Odontogenic fibroma: a clinicopathological study of 15 cases. J Formos Med Assoc 110(1): 27-35.
-
El-Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ, et al. (2017) WHO classification of head and neck tumours. 4th (Edn.), Lyon: International Agency for Research on Cancer, pp: 347.
-
Shafer WG, Hine MK, Levy BM (2009) Shafer’s textbook of oral pathology. 6th (Edn.), Elsevier, pp: 294-295.
-
Santoro A, Pannone G, Ramaglia L, Bufo P, Muzio LL, et al. (2016) Central odontogenic fibroma of the mandible: A case report with diagnostic considerations. Ann Med Surg (Lond) 5: 14-18.
-
Daley TD, Wysocki GP (1994) Peripheral odontogenic fibroma. Oral Surg Oral Med Oral Pathol 78(3): 329-336.
-
Gardner DG (1980) The central odontogenic fibroma; An attempt at clarification. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 5: 425-432.
-
Wesley RK, Wysocki GP, Mintz SM (1975) The central odontogenic-fibroma clinical and morphological studies. Oral Surg Oral Med Oral Pathol 40(2): 235-245.
-
Bhaskar SN (1977) Synopsis of Oral Pathology. 5th (Edn.), the CV Mosby Company, St. Louis, pp: 259-261.
-
Lukinmaa PL, Hietanee J, Anttinen J, Ahonen P (1990) Continuous enlarged dental follicles with histologic features resembling the WHO type of odontogenic fibroma. Oral Surg Oral Med Oral Pathol 70(3): 313-317.
-
Langlais RP, Langland OE, Nortje CJ (1995) Multilocular radiolucencies, In: Diagnostic Imaging of the Jaws, Williams & Wilkins, Baltimore, pp: 370-376.
-
Philipsen HP, Reichart PA, Sciubba JJ, van der Waal I (2005) Odontogenic fibroma. In: Leon Barnes, et al. (Eds.), World Health Organization Classification of Tumours. Pathology and Genetics of Head and Neck Tumours, IARC Press Lyon, pp: 315.
-
Gardner DG (1996) Central odontogenic fibroma: current concepts. J Oral Pathol Med 25(10): 556-561.
-
Martinez MG, Mosqueda TA, Carlos BR, de Almeida OP, Contreras VE, et al. (2008) Odontogenic myxoma: clinico- pathological, immunohistochemical and ultrastructural findings of a multicentric series. Oral Oncol 44(6): 601- 607.
-
Chen Y, Li TJ, Gao Y, Yu SF (2005) Ameloblastic fibroma and related lesions: a clinicopathologic study with reference to their nature and interrelationship. J Oral Pathol Med 34(10): 588-595.
-
Handschel JG, Depprich RA, Zimmermann AC, Braunstein S, Kubler NR (2005) Adenomatoid odontogenic tumor of the mandible: review of the literature and report of a rare case. Head Face Med 24:1-5.
-
Philipsen HP, Reichart PA, Zhang KH, Nikai H, Yu QX (1991) Adenomatoid odontogenic tumor: biologic profile based on 499 cases. J Oral Pathol Med 20(4): 149- 158.
-
Said Al Naief N, Fernandes R, Louis P, Bell W, Siegal GP (2006) Desmoplastic fibroma of the jaw: a case report and review of literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101(1): 82-94.
-
Dunlap CL (1999) Odontogenic fibroma. Semin Diagn Pathol 16(4): 293-296.
-
Neville BW, Damm DD, Allen CM, Bouquot JE (2009) Oral and Maxillofacial Pathology, 3rd (Edn.), WB Saunders, Philadelphia, pp: 968.
-
Weber A, van Heerden WF, Ligthelm AJ, Raubenheimer EJ (1992) Diffuse peripheral odontogenic fibroma: report of 3 cases. J Oral Pathol Med 2: 82-84.
-
Kenney JN, Kaugars GE, Abbey LM (1989) Comparison between the peripheral ossifying fibroma and peripheral odontogenic fibroma. J Oral Maxillofac Surg 47(4): 378- 382.
-
Marx RE (2007) Diane stern, oral and maxillofacial pathology: A rationale for diagnosis and treatment. Quintessence Publishing Co, Chicago, pp: 672-174.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells