The Repair of Resin-Modified Glass Ionomers with Bulk-Fill Flowable and Packable Composites using the Eight-Generation and Universal Dentin Bonding Agents
Background: To investigate shear bond strength regarding the repair of resin-modified glass ionomers (RMGIs) with bulk-fill flowable and packable composites using eighth-generation and universal dentin bonding agents. Materials and Methods: One-hundred-fifty specimens were prepared using polymethylmethacrylate-resin injected into preformed cylinders. Inverted recessed holes with convergent walls 4 mm deep and 4 mm wide were created using Operative Friction Grip 330L and inverted diamond burs. These holes were used as reservoirs for RMGI II LC. The resulting RMGI specimens were roughened with medium coarse diamond burs and placed in distilled water for 24 hours at 37o C to remove debris. RMGI surfaces were etched with 37% phosphoric acid for 20 seconds, rinsed with copious water, and air-dried without desiccation. Each RMGI specimen was placed in an Ultradent bonding clamp in preparation for adding the tested material. Specimens were divided into 6 groups: (1) Bulk-fill flowable composite (BFF) no adhesive (control), (2) Packable composite (PC) no adhesive (control), (3) BFF + iBond, (4) BFF + Futurabond-DC, (5) PC + iBond, and (6) PC + Futurabond-DC. Shear bond Strength was determined using an Ultra Tester Machine. Results: The SBS among and between groups were statistically assessed with repeated measures multivariate analysis of variance (MANOVA). The Tukey honestly significant difference test with an alpha level of 0.05 was used for post-hoc testing. Repeated measures MANOVA indicated that there were important differences between groups (Wilk’s lambda, P < 0.0001), with BFF + Futurabond-DC resulting in the highest SBS. Conclusion: The study indicates that BFF combined with eighth-generation dentin bonding adhesive is a reliable method for the repair of RMGIs
Introduction
Resin-modified glass ionomers were developed by adding resin to improve the mechanical properties of conventional glass ionomers (CGIs). CGIs form chemical bonds to tooth surfaces, either to dentin or enamel because of ion exchange between the material and the tooth surfaces [1]. The chemistry of CGIs was incorporated into resin- modified glass-ionomers (RMGIs) by adding hydrophilic monomers, such as 2-hydroxyethyl methacrylate (HEMA), resulting in increases in the diametral tensile strength as well as bond strength to teeth [2]. HEMA allows for light-curing (LC) that provides for immediate finishing after placement and results in increased strength. RMGIs (GC America, Alsip, IL, USA): (1) demonstrates improved mechanical bonding and esthetics when compared with CGIs; (2) are indicated for small lesions, non-stress-bearing restorations in permanent teeth, interim restorations of permanent teeth, atraumatic restoration techniques (ART) in geriatric patients, and as permanent restorations for deciduous teeth; (3) are considered to be the material of choice for the restoration of non-carious cervical lesions (NCCLs) in geriatric patients [3]; (4) are often advocated for class III, class V, and abfraction lesions due to their low modulus of elasticity; and (5) are used as the first layer in the proximal-gingival box for a class II restoration when the caries extends below the cemento- enamel junction (CEJ) with a technique called “open/closed- sandwich” [4]. These lesions are becoming more frequent in geriatric patients as they retain their teeth longer.
A study of the global population indicates that by 2030, there will be 400 million people above the age of sixty [5]. Increasing age can lead to a reduced unstimulated salivary flow that can cause coronal, root surface, and secondary caries [6]; thus, there is an increasing need for the maintenance and repair of RMGI restorations.
Bulk-fill flowable composite (BFF) is a nanohybrid with particle sizes ranging from 1 to 100 nm [7], which enables the resin to flow uniformly (a self-leveling feature [8] that allows intimate adaptation to the prepared form or wall of an existing restoration). The filler contains surface treated fume silicas to increase the viscosity when monomer is incorporated, and this allows an increased filler loading up to 60% by volume [6], which increases wear resistance. Their nano-sized filler particles offer the advantages of superior esthetic properties, high polishability, ease of handling, and are self-leveling [8]--all of which are essential for the repair of RMGIs.
Because packable composites (PCs) have stiffer viscosity than conventional composites, they are considered amalgam alternatives [9]. PCs contain up to 84% filler load that minimizes shrinkage and results in higher compressive strength, increased durability, easy placement, and superior polishing properties of restorations [9].
The combination of an eighth-generation bonding agent (Futurabond DC, Voco, Hanau, Germany) or a universal bonding agent (iBond, Heraeus Kulzer, Germany) with BFF resin may be a better choice for the repair of RMGIs than packable composites and bonding agents. Both dentin bonding agents have a notable moisture-controlled, simplified, all-in-one, single dose application.
iBond offers instant, reliable bond strength; whereas, Futurabond DC requires chemical and light-curing [10], is self-etching, bond reinforced, and has highly functionalized silicon dioxide (SiO2) nanoparticles that facilitate cross- linking with the resin components [10, 11]. Stress resulting from polymerization shrinkage of the resin with Futurabond DC can be counteracted by a thicker and thus more flexible interface of the nanofillers, which may improve repair strength, marginal integrity, and decrease microleakage [10]. These qualities are especially practical, and convenient for geriatric patients for whom optimal isolation often presents a challenge. The objectives of this laboratory-based study were to investigate shear bond strengths resulting from the repair of resin-modified glass-ionomers with bulk-fill flowable composite and packable composite, using eighth- generation and universal dentin bonding agents. The research hypothesis was that there is a difference between the shear bond strength (SBS) of the repaired RMGI with bulk-fill flowable resins and packable composites.
Materials and Methods
The materials used, manufacturers, their classifications, and chemical composition are included in Table 1.
| Material and Manufacture | Classification | Resin Matrix Composition | Filler Particles Composition | Vol% filler |
|---|---|---|---|---|
| SDR flow + bulk-fill flowable (Densply Sirona, York, Pennsylvania, USA) | Nanohybrid | TEGMA, modified urethane dimethacrylate resin, polymerizable dimethacrylate resin. | Silanated barium-alumino-fluoro-borosilicate glass; silanated strontium alumino-fluoro-silicate glass; surface treated fume silicas; ytterbium fluoride; synthetic inorganic iron; oxide pigments; titanium dioxide; and BHT. | 47.4 |
| Packable Composite (Kerr Corporation, Orange, CA, USA) | Nanohybrid | TEGMA | Barium aluminoborosilicate glass and Silica nanofiller | 69 |
| RMGI II LC (GC America Inc., Alsip, IL, USA) | Resin-modified glass ionomers | HEMA | Fluoroaluminosilicate glass; Glass ionomer; Polyacrylic acid; Tartaric acid; Glass; Water; Initiator; and Camphorquinone | n/a |
| IBond (Heraeus Kulzer, Hanau, Germany) | Universal All-in- one Adhesive | 4-META, 10-MDP, and UDMA | Acetone Water Glutaraldehyde Camphoroquinon Stabilizers | n/a |
| Futurabond DC (Voco, Cuxhaven, Germany) | Nanoparticles All-in-one Adhesive | BIS-GMA, HEMA, organic acids, and TMPTMA | Silanated barium-alumino-fluoro-borosilicate glass; silanated strontium alumino-fluoro-silicate glass; surface treated fume silicas; ytterbium fluoride; synthetic inorganic iron oxide pigments, BHT, ethanol, fluorides, CQ, amine, catalysts, and titanium dioxide | n/a |
Table 1: Dental materials used in the current study.
Bis-GMA: bisphenol A-diglycidyldimethacrylate; UDMA: urethane dimethacrylate; TEGMA: triethyleneglycolmethacrylate; 4-META: 4-methacryloxyethyltrimelliticacidanhydride; 10-MDP: 10-methacryloyloxydecyldihydrogenphosphate; BHT: butylated hydroxytoluene; HEMA: 2-hydroxyethyl methacrylate; CQ: camphorquinone (photoinitiator); TMPTMA: trimethylolpropane trimethacrylate. Table 1: Dental materials used in the current study.
One-hundred-fifty polymethylmethacrylate resin (Figure 1A, Biocryl Resin acrylic, Great Lakes Dental Technology, Tonawanda, New York, USA) specimens were created using preformed cylinders (Figure 1B, Ultradent Products, Inc., South Jordan, UT, USA), and in each specimen, a 4 mm deep and 4 mm wide reservoir (Figure 1D) was created using an Operative Friction Grip 330L carbide bur (Meisinger, USA- HM7L-008-FG, Benco Dental, Pittston, PA, USA) and an inverted diamond bur (1440A-Diamonds-FG, Benco Dental, Pittston, PA, USA).
| Group A1-E | No. of specimen | Surface treatment | Adhesives | Tested Dental Materials |
|---|---|---|---|---|
| Group A1 | 25 | Specimens were etched with 37% phosphoric acid for 20 s, rinsed with copious water using air-water spray with agitation, and dried with air (from the air-water spray) for 5 s without desiccating. | no | Bulk-fill flowable (BFF) was extruded into the 2 mm deep recessed hole (Figure 1H-J) in the bonding mold and light-cured for 40 s. The specimen was gently removed (Figure 1M) from the bonding mold using a composite instrument CIGFT2 (HU-Friedy, Chicago, IL USA), inspected using 4.5x magnification Prism loops to ensure no void or excess BFF was present, assembled in a test base clamp (Figure 1N) and transferred to the Ultra Tester machine (Figure 2) for SBS testing. |
Group A2 25 Specimens were prepared similar to Group A1. no Specimens were treated similar to Group A1/A2, then an iBond Universal was gently rubbed with a microbrush for 20 s to the surface of each specimen, dried with oil-free air flow using an air-water syringe until the adhesive film no longer moved, and the surface appeared glossy, and was light- cured. Each specimen was transferred and assembled in a bonding clamp (Figure 1I-K) Group B 25 Specimens were treated similar to Group A1/A2, then Futurabond DC was mixed with 1 drop of Liquid 1 and 1 drop of Liquid 2; the resulting solution was rubbed with a microbrush onto the surface of specimen for 20 s, dried with air from an air-water syringe for 5 s, and light-cured; each specimen was transferred and assembled in a bonding clamp (Figure 1I-K).
Packable composite (PC) was extruded into the 2 mm recessed hole (Figure 1L) with similar steps as Group A1. The specimen was gently removed (Figure 1M) from the bonding mold with similar steps as Group A1, assembled in a test base clamp (Figure 1N) and transferred to the Ultra Tester machine (Figure 2) for SBS testing.
BFF was extruded into the 2 mm deep recessed hole (Figure 1K) in the bonding mold and light-cured for 40 s. The specimen was gently removed (Figure 1M) from the bonding mold with similar steps as Group A1, assembled in a test base clamp (Figure 1N) and transferred to the Ultra Tester (Figure 2) for SBS testing.
iBond Universal
BFF was extruded into the 2 mm deep recessed hole (Figure 1K) in the bonding mold and light-cured for 40 s. The specimen was gently removed (Figure 1M) from the bonding mold with similar steps as Group A1, assembled in a test base clamp (Figure 1N), and transferred to the Ultra Tester machine (Figure 2) for SBS testing.
- Eighthgeneration adhesive,
- Futurabond
- DC
- Group C
- 25
- Group D
- 25
- Specimens were treated similar to
- Group A1/A2 and Group B. iBond
- Universal
- Eighthgeneration adhesive,
- Futurabond
- DC
- Group E
- 25
- Specimens were treated similar to
- Group A1/A2 and Group C.
Table 3: One-hundred-fifty specimens divided into 6 groups.
For the samples, Fuji II LC capsules (GC America Inc., Alsip, IL, USA) were activated by means of trituration using an amalgamator (OptiMix, Kerr, Orange, CA, USA), according to the manufacturer’s instructions, and the activated Fuji II LC were used to fill individual reservoirs (Figure 1D) with an initial 2 mm increment (Figure 1E), light-cured with a focus pen style light-emitting diode (LED, Densply, Sirona, Charlotte, North Carolina, USA); on top of this, a final 2
mm increment of Fuji II LC was injected, covered with a microscope-glass-slide (Fisher Scientific, Lenexa, KS, USA), and light-cured (Figure 1F). The 150 specimens were divided into six groups, A1-E, listed in Table 2.
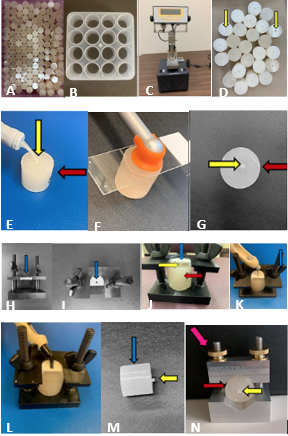
The resulting specimens were roughened to evenly uniform surfaces (Figure 1G) with medium coarse diamond burs (SS White 837-012M, Benco Dental, Pittston, PA, USA), rinsed with water using air-water spray, and placed in distilled water for 24-hour at 37°C to remove debris. The surfaces were etched with 37% phosphoric acid (Pentron Clinical, Orange, CA, USA) for 20 s, rinsed with copious water using oil-free, air-water spray, and dried without desiccation. For the control groups A1 and A2, no bonding agent was used. For groups B and D, an iBond Universal bonding agent was gently rubbed onto the surface of each specimen with a microbrush (Henry Schein, Chesterfield, MO, USA) for 20 s, dried with oil-free air flow using an air-water syringe until the adhesive film no longer moved, and the surface appeared glossy. The specimen was then light-cured for 10 s.
Each specimen was placed in a bonding clamp (Figures 1H-J, Ultradent Products, Inc., South Jordan, UT, USA) with group B filled with BFF (Figure 1K), and D filled with PC (Figure 1L), light-cured for 40 s, and carefully removed from the bonding mold using a composite instrument CIGFT2 (HU- Friedy, Chicago, IL, USA). For groups C and E, Futurabond DC bonding agent mixed with 1 drop of Liquid 1 and 1 drop of Liquid 2 was rubbed onto the surface of each specimen with a microbrush for 20 s, dried with air from an air-water syringe for 5 s, and light-cured for 10 s. Each specimen was placed in a bonding clamp (Figures 1H-J) with group C filled with BFF (Figure 1K), and E filled with PC (Figure 1L), light- cured for 40 s, and carefully removed from the bonding mold using a composite instrument (CIGFT2). The final specimens containing RMGIs with bonded 2 mm by 2 mm test materials (Figure1M) were individually placed in the test base clamp (Figure 1N) in preparation for SBS testing using the Ultra Tester Machine (Figure1C, Ultradent Products, Inc., South Jordan, UT, USA). With the Ultra Tester Machine (Figure 1C & Figure 2 (left)), the maximum SBS to fracture failure in Megapascal (MPa) was recorded for each specimen.
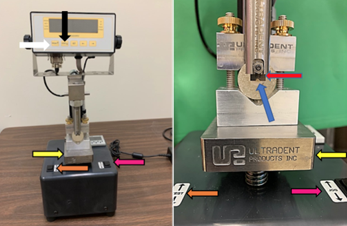
Figure 2: Ultra Tester Machine (left) and a close-up view of specimen testing (right). The clamped specimen (blue arrow) was placed under the crosshead (red arrow) on the loading platform (yellow arrow). By adjusting the “Jog” switch (pink arrow), the specimen was aligned to fit the notch in the crosshead (red arrow) leaving a 0.5 mm space, between the specimen and the notched crosshead. The back of the crosshead and the base of the specimen was verified to be flush with no space between them. The meter was set to “Peak” mode (black arrow) to record the maximum force applied to the specimen during each test. Before each test was activated, the meter was reset by pressing the “Zero” key (white arrow). When the test switch (orange arrow) was pushed upward, the test was activated, and the Ultra tester platform raised at a rate of 1mm/min to engage the specimen with the crosshead and break the specimen with the peak value recorded in Megapascal (MPa).
Statistical Analysis
The samples used in this study were created by injecting resin-modified glass-ionomers (RMGI) into inverted holes created in polymethylmethacrylate-resin specimens, with there being no difference in the polymethylmethacrylate- resin nor in the RMGI that was used to create samples. The resulting samples were equally divided into six groups, and for the six groups, six different test materials were added to the prepared surfaces of RMGIs. The sheer bond strengths (SBSs) were determined for the samples in each group (that is, SBSs were determined for each treatment). The different treatments were considered repeated treatments of the same material, and the SBSs that were determined for the samples for each treatment (group) were considered repeated measures of the same material. Paired t tests (dependent t tests) could be performed between each of the six treatments. Paired t tests would have more statistical power than unpaired t tests because assessing differences in specimens with paired t tests eliminates variations in samples that could be caused by anything other than differences caused by treatments. For our assessment, we, however, used repeated measures analysis of variance (ANOVA) to assess the differences between the six treatments (groups) [12], with repeated measures-ANOVA having more statistical power than multiple paired t tests. Although factors such as surface preparations could result in SBS differences, because 150 specimens were prepared, we were confident that such factors would not systematically affect the clinical importance of SBS differences in treatments. More specifically, as described above, all samples for the 6 groups had the surfaces roughened, etched with 37% phosphoric acid (Pentron Clinical, USA) for 20 seconds; rinsed with copious water using air-water spray with agitation for 5 s, and dried without desiccation. Rather than use standard repeated measures analysis of variance (ANOVA) for our analysis to assess differences in shear bond strength (SBS) among and between groups, we used repeated measures multivariate analysis of variance (MANOVA), with one within-subject (repeated measures) factor for which there were 6 levels (one repeated-measure for each of the 6 groups). An advantage of repeated measures MANOVA over standard repeated measures ANOVA is that it does not require the assumption of sphericity, which is the requirement that variances of the differences between all combinations of related groups (levels) are equal (orthogonal components)[13]. Multivariate ANOVA is also quite robust for all but severe violations of the assumptions of normality [14, 15]; nevertheless, for the six groups, we did assess the distributions of the raw data and the distributions of the residuals resulting from our analysis to assess whether the raw data or residuals had concerning departures from normality. To perform these assessments, we used normal quantile plots fitted with Lilliefor’s confidence intervals (an adaptation of the Kolmogorov-Smirnov test). For these assessments, examination of the normal quantile plots for the six groups revealed no serious concern with the normality of any distribution. The Tukey honestly significant difference test was used for post-hoc testing, and we include Table 3 that lists the results of Tukey HSD assessments.
| GROUPS | A1 | A2 | B | C | D | E |
|---|---|---|---|---|---|---|
| A1 | 0.0011 | 0.0007 | 0.0001 | 0.0005 | 0.3847 | |
| A2 | 0.0011 | 0.0001 | 0.0001 | 0.0001 | 0.0001 | |
| B | 0.0007 | 0.0001 | 0.2954 | 1 | 0.1911 | |
| C | 0.0001 | 0.0001 | 0.2954 | 0.3687 | 0.0004 | |
| D | 0.0005 | 0.0001 | 1 | 0.3687 | 0.1442 | |
| E | 0.3847 | 0.0001 | 0.1911 | 0.0004 | 0.1442 |
Table 4: Results of Post-hoc Testing with the Tukey Honestly Significant Difference (HSD) test.
Post-hoc comparisons of the 6 groups resulted in 15 P values. The P value presented in the lower- left triangular section of the table are also presented in the upper-right triangular section of the table. Either the Group name for a column can be matched with the Group name for a row or vice versa. For example, if column name A1 is matched with row name E, the resulting P value is 0.3847, and vice versa, if column name E is matched with row name A1, the resulting P value is 0.3847. A1- bulk-fill flowable resin (BFF), A2- packable composite (PC), B- BFF+ iBond, C- BFF+ Futurabond DC, D- PC+ iBond, E- PC+ Futurabond DC.
For testing, the alpha level was set at 0.05; however, as was recently recommended in an article (with 800 signatories) that was written by statisticians and scientists, our focus was on the clinical importance of the results rather than the P values [16]. In keeping with this recommendation, we include Figure 3 that contains a plot of mean responses (and 95% confidence intervals) for the six groups, and as part of the study, it was decided that if the mean values between two groups differed by ≥ two units of measurements in shear bond strength (SBS), this would be considered a clinically important difference.
28
| 22.4 | ||||||
| 19.7 | 19.8 | |||||
| 16.6 | ||||||
| 14.0 | ||||||
| 8.6 | ||||||
Figure 3: Group means and 95% confidence intervals. Shear Bond Strength (SBS) was recorded in Megapascal (MPa) units. The top and bottom crosshatches on a vertical line (above a group designation) represent the 95% confidence interval. If 95% confidence intervals for two groups do not overlap, the means for the groups represented by the confidence intervals are different (P ≤ 0.001). SBS was recorded in MPa. A1- bulk-fill flowable resin (BFF), A2 - packable composite (PC), B - BFF + iBond, C – BFF + Futurabond DC, D – PC + iBond, E – PC + Futurabond DC.
We had no preliminary data for a sample-size (power) calculation, and although we performed a careful search of the literature; no study could be identified that used a repeated- measures analysis (such as a paired t-test, repeated-measures analysis of variance, or multivariate repeated-measures analysis of variance); rather, most analyses were performed to determine differences between/among independent groups, and the resulting means and standard deviations of the means were reported. For a repeated-measures, sample- size calculation (power analysis) the research hypothesis that is tested is that the mean difference between paired observations for the two groups = 0.00. To perform such a sample-size calculation, the mean difference and standard deviation of difference are required; therefore, prior to collecting and analyzing our data, a power analysis could not be performed; however, in studies that used independent samples, most sample sizes ranged from 10 to 25. For our study, we, therefore, used the upper range (n=25) of these values for our sample sizes for each group. We thought that sample sizes of 25 would be sufficient to demonstrate the clinical and statistical importance of any differences that were detected. After our analyses, based upon our results, we performed several power analyses for paired t-tests, and for these assessments, our statistical power exceeded 99.9% (note: the statistical power of multiple paired t-tests is lower than the statistical power of a repeated measures MANOVA). Upon request, the data that we analyzed in this study are available from the lead author. Statistical analyses were performed with Tibco Statistica 13.5 (Palo-Alto, California), JMP Pro Statistical Software Release 15.2.1 (SAS Institute, Inc., Cary, NC), and Power and Precision Release 4.1 (Biostat, Inc., Englewood, NJ).
Results
Repeated measures MANOVA indicated that there were important differences in SBS among groups (Wilk’s lambda, P < 0.0001). Figure 3 contains a plot of group means and 95% confidence intervals. If the 95% confidence intervals do not overlap, the means for the groups represented by the confidence intervals are different (P ≤ 0.001), as is confirmed in Table 3 that contains the results of the Tukey HSD tests for differences between groups. Group C [bulk-fill flowable resin (BFF) + Futurabond DC] had the highest value for SBS (22.4 MPa), with this value not being statistically higher than the value (19.7 MPa) for B [BFF+ iBond] nor the value (19.8
MPa) for D [packable composite (PC) + iBond]. Because these respective differences (2.7 MPa and 2.6 MPa) in SBS exceeded what was considered to be a clinically important difference (2 MPa SBS units of measurement), the BFF + Futurabond DC group was considered to have higher SBS than either BFF + iBond or PC + iBond. The lowest SBS (8.6 MPa) was for A2 [packable composite (PC) without adhesive], which was lower than values for other groups (P ≤ 0.001).
Discussion
The results of this study support our research hypothesis and indicate that there are important differences between groups (Figure3), with BFF + Futurabond DC resulting in the highest SBS [17] and PC with etching but without dental bonding adhesive resulting in the lowest SBS. RMGIs are considered to be the material of choice for the restoration of the lesions in geriatric patients [1]. Clinically, the retention rate of RMGIs over 13 years is > 97% [18]. A 5-year clinical study determined the retention rate to be 96.4% when non- carious-cervical lesions (NCCLs) were restored with RMGIs versus a 51.5% retention rate when restored with composite resins [18]; however, the need for repair is unavoidable in cases for which proper contours are inadequate, marginal adaptations are substandard, color has changed over time, and voids are presence[19, 20, 21]. The cervical margin is frequently located in either cementum or dentin, and this presents a challenge in restoring NCCLs; moreover, this characteristic makes the cervical margin more susceptible to microleakage, causing cavosurface stains, post-operative sensitivity, and secondary caries in dentin—for which organic matrix degradation is prevalent due to a high concentration of the enzyme metalloproteinases (MMPs) that activate when the pH in the oral environment falls below a normal pH of 6.75 or when salivary flow decreases [18, 22, 23]. A clinical study on restoring class V lesions with RMGI versus composite resin restorations (with a similar adhesive) found that clinical performance of RMGI restorations surpassed that for composite resin restorations [24]. The benefits of repair outweigh total replacement by reducing cost, dental anxiety, and preserving tooth structure [25]. Previous studies demonstrated high SBS between BFF and dentin bonding adhesives [26, 27, 28, 29], with acceptable marginal adaption being shown for Futurabond DC, using the etch and rinse technique [28]. The cohesive strength on the surface of RMGI decreases when etched with 37% phosphoric acid6 due to the dissolved filler particles in the matrix leading to a decrease in viscosity 2-hydroxyethyl- methacrylate (HEMA) and functional methacrylate groups [29, 30, 31]. The authors speculating that the highest SBS resulted from BFF + Futurabond DC was attributable to the lower viscosity of Futurabond DC, its characteristics of dual-curing with the chemical-cured property reaching the inaccessible areas by curing light; and improved wetting of the RMGI leading to higher SBS achieved through the lower contact angle [32]. A systemic review and meta-analysis found that BFF composites are preferred over packable resin-based composites in the repair of RMGI in class III and V restorations because of their greater flexibility and better marginal adaptation [20, 33], which is supported by the present study. A study on the comparison BFF composites indicated that BFF resulted in the highest fracture toughness [24, 25]; this combined with thinner viscosity of Futurabond DC resulted in the authors concluding that BFF + Futurabond DC are clinically relevant in the repair of RMGI; moreover, the highest value of SBS on the repair of RMGI between BFF + Futurabond DC is the result of mechanical and chemical properties among RMGI, BFF, and Futurabond DC—with this result being caused by the interlocked micromechanical bond between adhesive, RMGI, and BFF. The limitations of our study are that we did not demonstrate SBS to dentin; therefore, the phosphoric acid did not play an important role in removing the smear layer and smear plugs from the dentinal tubules; however, studies of RMGI etching support the cohesive strength of RMGI, leading to increased SBS when dental adhesive is used [6, 29, 30, 31]. The direction of future research can focus on determining SBS of the repair RMGI in saliva at various temperatures. The current study resulted in the highest SBS for BFF with Futurabond DC in the repair of RMGI. The benefits of repair of RMGI defects consist of reducing chairside time and perhaps eliminating need for anesthesia that may result in lower anxiety for a patient, a reduction in dental care cost, preservation of tooth-structure, and decrease in post-operative sensitivity. Conclusion The present study found that the highest SBS occurred when BFF + Futurabond DC were used in the repair of RMGI; lower SBS resulted with PC + Futurabond DC, and the lowest SBS was between etched PC without dental bonding adhesive.
References
-
Gjorgievska E, Nicholson JW, Iljovska S, Slipper IJ (2008) Marginal adaptation and performance of bioactive dental restorative materials in deciduous and young permanent teeth. J Appl Oral Sci 16(1): 1-6.
-
Khoroushi M, Keshani F (2013) A review of glass- ionomers: From conventional glass-ionomer to bioactive glass-ionomer. Dent Res J (Isfahan) 10(4): 411-420.
-
Kampanas NS, Antoniadou M (2018) Glass Ionomer Cements for the Restoration of Non-Carious Cervical Lesions in the Geriatric Patient. J Funct Biomater 9(3): 42.
-
Brackett MG, Ryan JM, Haddock FJ, Romero MF, Bracket WW (2018) Use of a Modified Matrix Band Technique to Restore Subgingival Root Caries. Oper Dent 43(5): 467- 471.
-
Ehrlich, Paul R (1971) The Population Bomb, 8th edition, Sierra Club, New York, USA, Ballatine Books.
-
Pandey AS, Lokhande TM, Gulve NM, Kolhe JS, Aher BG (2019) Shear bond strength of composite resin to resin- modified glass ionomer cement using 2- hydroxyethyl methacrylate-based and 2-hydroxyethyl methacrylate- free adhesive system. J Conserv Dent 22(3): 292-295.
-
Kenneth JA, Shen C, Rawls HR (2013) Phillips’ Science of Dental Materials 12th (Edn.), St. Louis, Missouri, Elsevier.
-
Altinici P, Mutluay M, Tezvergil Mutluay A (2018) A Repair bond strength of nanohybrid composite resins with a universal adhesive. Acta Biomaterialia Odontol Scand 4(1): 10-19.
-
Leinfelder FK, Bayne CS, Swift JE (1999) Packable Composites: Overview and Technical Considerations. J Esthet Dent 11(5): 234-249.
-
Mishra A, Koul M, Upadhyay KV, Abdullah A (2020) A Comparative Evaluation of Shear Bond Strength of Seventh- and Eighth-Generation Self-etch Dentin Bonding agents in Primary Teeth: An _In Vitro_ Study. Int J Clin Pediatr Dent 13(3): 225-229.
-
Sidhu SK (2010) Clinical evaluations of resin-modified glass-ionomer restorations. Dent Mater 26(1): 7-12.
-
Altman DG (1999) Practical statistics for medical research. Boca Raton, Fla., Chapman & Hall/CRC. pp: 331-334.
-
Hill T, Lewiki P (2006) Statistics Methods and Applications. Tulsa, Oklahoma, StatSoft.
-
Lindeman RH, Merenda PF, Gold R (1980) Introduction to bivariate and multivariate analysis. New York, Foresman & Co.
-
Lindman HR (1974) Analysis of variance in complex experimental designs. San Francisco, California, WH Freeman & Co.
-
Amrhein S, Greenland B, McShane (2019) Scientists rise up against statistical significance. Nature pp: 567.
-
Taneja S, Kumari M, Bansal (2017) Effect of saliva and blood contamination on the shear bond strength of fifth-, seventh-, and eight-generation bonding agents: An _in_ _vitro_ study. J Conserv Dent 20(3): 157-160.
-
Welch D, Seesengood B, Hopp C (2015) Surface Treatments that Demonstrate a Significant Positive Effect on the Shear Bond Strength of Repaired Resin- modified Glass Ionomer. Oper Dent 40(4): 403-409.
-
Jain A, Bahuguna R (2015) Role of matrix metalloproteinases in dental caries, pulp and periapical inflammation: An overview. J Oral Biol Craniofac Res 5(3): 212-218.
-
Boukpessi T, Menashi S, Chaussain C (2017) Endogenous Enzymes in Root Caries. Oral Sci 26: 35-42.
-
Qahtani M, Shethri S (2010) Shear bond strength of one-step self-etch adhesives with different co-solvent ingredients to dry or moist dentin. Saudi Dent J 22(4): 171-175.
-
Kasraie S, Shokrpour M, Safari M (2013) Evaluation of micro-shear bond strength of resin modified glass- ionomer to composite resins using various bonding systems. J Conserv Dent 16(6): 550-554.
-
Heintze SD, Ruffieux C, Rousson V (2010) Clinical performance of cervical restorations-A meta-analysis. Dent Mater 26(10): 993-1000.
-
Gordan VV, Shen C, Riley J, Mjor IA (2006) Two-year clinical evaluation of repair versus replacement of composite restorations. J Esthet Restor Dent 18(3): 144- 153.
-
Zhang Y, Burrow MF, Palamara JE, Thomas CD (2011) Bonding to glass ionomer cements using resin-based adhesives. Oper Dent 36(6): 618-625.
-
Boruziniat A, Gharaei S (2014) Bond strength between composite resin and resin modified glass ionomer using different adhesive systems and curing techniques. J Conserv Dent 17(2): 150-154.
-
Arora V, Kundabala M, Parolia A, Thomas MS, Pai V (2010) Comparison of the shear bond strength of RMGIC to a resin composite using different adhesive systems: An in vitro study. J Conserv Dent 13(2): 80-83.
-
Manarte Monteiro P, Domingues J, Teixeira L, Gavinha S, Manso CM (2019) Multi-Mode adhesives performance and success/retention rates in NCCLS restorations: randomized clinical trial one-year report. Biomaterial Investigations in Dentistry 6(1): 53-53.
-
Gopikrishna V, Abarajithan M, Krithikadatta J, Kandaswamy D (2009) Shear bond strength evaluation of resin composite bonded to GIC using three different adhesives. Oper Dent 34(4): 467-471.
-
Pamir T, Sen BH, Evcin O (2012) Effects of etching and adhesive applications on the bond strength between composite resin and glass-ionomer cements. J Appl Oral Sci 20(6): 636-642.
-
Inoue S, Abe Y, Yoshida Y, De Munck J, Sano H, et al. (2004) Effect of conditioner on bond strength of glass- ionomer adhesive to dentin/enamel with and without smear layer interposition. Oper Dent 29(6): 685-692.
-
Mount GJ (1989) The wettability of bonding resins used in the composite resin/glass ionomer sandwich technique. Aust Dent J 34(1): 32-35.
-
Szesz A, Parreiras S, Martini E, Reis A, Loguercio A (2017) Effect of flowable composites on the clinical performance of non-carious cervical lesions: A systematic review and meta-analysis. J Dent 65: 11-21.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells