1α,25-Dihydroxyvitamin D3 Improves Implant Osseointegration in T2DM Via Inhibiting Oxidative Stress
Hyperglycemia-generated oxidative stress would result in impaired osseointegration of implant and high rate of implantation failure. Previous studies have demonstrated that 1α,25-dihydroxyvitamin D3 (1,25VD3 ) favored glucose homeostasis and implant osseointegration in diabetic rats. However, its concrete mechanisms in osteogenesis still remains unclear. We investigated herein that 1,25VD3 might ameliorate the osseointegration through suppressing oxidative stress in type 2 diabetes mellitus (T2DM). T2DM rats was induced by administration of streptozotocin and received implants insertion, with or without 1,25VD3 treatment for 12 weeks. After sacrifice, the plasma oxidative stress-related biomarkers level, bone microarchitecture and biomechanical index of rats were measured systematically. Osteoblasts were isolated and exposed to high glucose, and osteogenic differentiation was evaluated by alizarin red staining, alkaline phosphatase (ALP) staining, revers transcription-qPCR and Western blotting analysis. The reactive oxygen species (ROS) level, malondialdehyde (MDA) level and superoxide dismutase (SOD) activity were detected to evaluate oxidative stress. The results suggested that 1,25VD3 could reverse the impaired osseointegration and mechanical strength by suppressing the hyperglycemia-generated oxidative stress. Our study also provides a new theoretical basis that the application of 1,25VD3 might be a novel approach to suppress oxidative stress and enhance implant osseointegration in diabetic patients.
Introduction
Currently, implant restoration has become a predictable and effective treatment option for the rehabilitation of edentulous or partially edentulous patients. Although high success rates of implant restoration have been widely reported, there still exists risk factors which could compromise the biological process of osseointegration, even result in implant failure. Type 2 diabetes mellitus (T2DM) is one of these risk factors [1]. T2DM is a complex chronic metabolic disease characterized by abnormal metabolism and durable hyperglycemia [2]. The pathophysiological mechanisms of T2DM, such as abnormal bone mineral density, reduction of vascular supply due to microangiopathies, decrease of host defense, disturbances in vitamin D, reduction of collagen production and increased collagenase activity [3, 4], can adversely affect implant osseointegration [5, 6]. Therefore, how to improve implant osseointegration among T2DM patients has important significance.
A growing body of evidences indicate that oxidative stress is one of the main causative factors that are responsible for the pathogenesis of insulin resistance, impaired insulin secretion from the β‐cells of pancreatic islets and pathogenesis of T2DM via activation of various pro‐inflammatory mediators, transcriptional mediated molecular and metabolic pathways [7, 8]. As reported in studies, oxidative stress inhibits the maturation of osteoblasts and osteoblastic differentiation [9, 10, 11], induces osteoblast insults and apoptosis [12, 13], and is associated with diabetic osteopenia [14]. This leads to a vicious cycle of metabolic stress and results in the increased production of reactive oxygen species (ROS), which has a direct impact on the function of osteoclasts, osteoblasts and osteocytes [15].
1α,25-dihydroxyvitamin D3 (1,25VD3), the active form of vitamin D, exerts its biological function by directly binding to the vitamin D receptor (VDR) [16]. 1,25VD3 is responsible for regulating calcium-phosphorus metabolism and bone mineralization [17, 18]. It is also recognized as a regulator of both osteoblast mediated bone formation and osteoclast mediated bone resorption [19]. According to epidemiological studies, vitamin D deficiency is associated with a higher incidence of T2DM [20], while the considerable inverse correlation between circulating 1,25VD3 levels and risk of T2DM has also been demonstrated [21]. Recently, researchers found that 1,25VD3 could promote bone remodeling, inhibit bone resorption and improve the impaired implant osseointegration capacity in diabetic rats [22]. Nevertheless, the concrete mechanisms by which the 1,25VD3 regulates implant osseointegration under poor glycemic control conditions still remains unclear.
Therefore, based on the well-explained background, we assume that the application of 1,25VD3 might improve implant osseointegration in T2DM via inhibiting oxidative stress.
Materials and Methods
Animals
All animal care and experiments were conducted in accordance with international standards on animal welfare experiments and approved by Institutional Animal Welfare and the Animal Ethics Committee of Shandong University (Jinan, China). Fifteen male Sprague-Dawley rats between 10 and 11 weeks old and weighing 180-220g were purchased and fed in the Experimental Animal Center of Shandong University (Jinan, China) under optimum rearing condition.
Inducement of T2DM
After 1-week adaptive breeding, rats were randomly divided into control group, T2DM group and 1,25VD3-treated group. Each group consisted of 5 rats. Five control group rats were given ordinary feed continuously, while rest ten rats were fed with high-fat and high-carbohydrate diet to induce T2DM model. Four weeks later, rats in model group were intraperitoneally injected with 30 mg/kg streptozotocin (STZ, Sigma, USA) solution after 12h fasting, and another group rats were treated with citrate buffer. Rats with fasting blood glucose (FBG) over 11.1 mmol/L at 1 week after injection were validated as hyperglycemia and used for further research.
Implant Surgery and Treatment
After weighing, the rats were anesthetized by intraperitoneal injections of 10% chloral hydrate (40mg/ kg, Sigma, USA). Special designed mini-Ti implants with 10mm in length and 1mm in diameter were implanted into intercondylar fossa under aseptic conditions as previously reported [23]. All the animals received intramuscular antibiotic injection for three postoperative days. Three days after implantation, the 1,25VD3-treated diabetic rats received 1,25VD3 (Sigma, USA) at a dose of 0.5μg/kg [24] during the entire period of experiment. 12 weeks after 1,25VD3 treatment, all rats were sacrificed, and the peripheral blood and bilateral femurs with implants were harvested for valuation. The specimens with implant were fixed in 4% polyformaldehyde.
Estimation of FBG and Body Weight
Blood samples were collected from tail vein of each animal after 12h-fasting on 0 day (before STZ inducement), 7th day and every 2 weeks after the 1,25VD3 treatment. Blood glucose levels were estimated by glucose oxidase method. The body weight of rats subjected to different treatments were recorded at the same time point mentioned above.
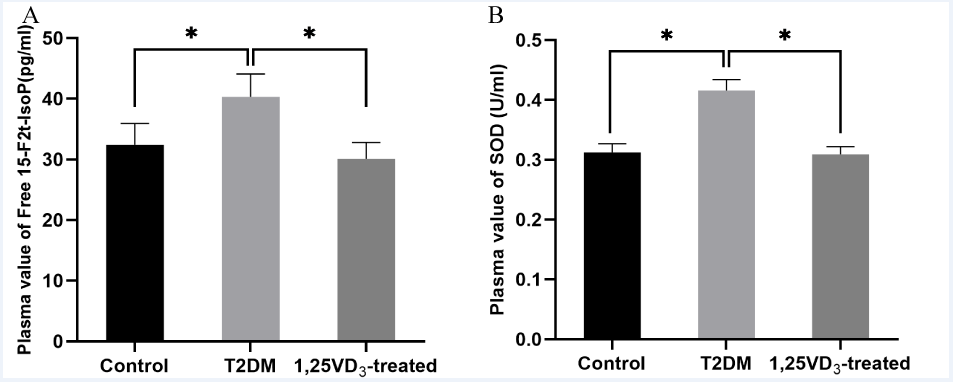
Plasma value of free 15-F2t-Isoprostane (15-F2t-IsoP) and Superoxide Dismutase (SOD)
Plasma values of free 15-F2t-IsoP and SOD were analyzed by commercial Kits strictly following the manufacturer’s protocol (Cayman, USA). The plasma value of free 15-F2t- IsoP was expressed by pg/mL and activity of SOD was expressed by U/mL.
Microscopic Computerized Tomography (micro- CT) Analysis
Fixed specimens were scanned by the micro-CT instrument (Rigaku, USA). The region of interest (ROI) was defined as bone tissues from 200μm around the implant for 3D reconstruction. The bone volume per total volume (BV/TV), trabecular thickness (Tb. Th), trabecular number (Tb. N), trabecular separation (Tb. Sp), and percentage of osseointegration (%OI) were analyzed by Mimics 19.0 [22].
Pull-Out Test
Pull-out test was performed by the universal material testing instrument (Shimadzu, Japan). The maximum pull- out force represents the maximum retention force obtained by the implant in the bone. The specimen was fixed on the machine, setting stretch speed was 1 mm/min and the maximum force was recorded at the moment of departure.
Histological Analysis
The histologic samples were dehydrated through a graded series of ethanol solutions and embedded in polymethyl methacrylate (PMMA, Merck AG, Germany) without decalcification. Subsequently, the embedded specimens were sectioned by hard tissue slicer (Leica, Germany) with a thickness of 100 μm. Then, the sections were stained in methylene blue-acid fuchsin. The index of bone-implant contact (BIC) was measured by NIS-Elements image software, which was defined as the length percentage of direct bone-implant interface to total implant surface in the cancellous bone [25].
Cell Culture
Osteoblasts were isolated from neonatal rat (<24h old) calvaria according to a previous study Jonason JH [26]. In brief, the calvaria were dissected and cut into 1×1 mm2 pieces and inoculated in culture flask containing 5 mL Dulbecco’s modified Eagle’s medium (DMEM, Hyclone, USA) medium supplemented with 10% fetal bovine serum (FBS, BI, USA), 100 U/mL penicillin G and 100 U/mL streptomycin (Beyotime, China), culturing at 37°C under 5% CO2 atmosphere in a cell incubator. Cell culture medium was changed every other day. Cells at the third passage were used for further research.
Osteoblasts were seeded in multiple-well plates and treated as following groups: (1) control group (NC), cells were cultured in complete culture medium containing 5.5 mmol/L D-glucose; (2) high glucose group (HG), cells were incubated with complete culture medium containing 30 mmol/L glucose [27]; (3) high glucose with 1,25VD3 group (HG+1,25VD3), cells were cultured in complete culture medium with 30 mmol/L glucose and 10-8mol/L 1,25VD3 [28]. For osteogenic induction, osteoblasts were cultured in an osteogenic induction medium containing DMEM supplemented with 10% FBS, 50 mg/L ascorbic acid (Sigma, USA), 10 nM dexamethasone (Solarbio, China) and 10 mM β-glycerophosphate (Solarbio, China).
Alkaline Phosphatase (ALP) Staining
After 7-day osteogenic induction, ALP activity was determined by 5-bromo-4-chloro-3-indolyl phosphate/nitro blue tetrazolium (BCIP/NBT) staining kit (Beyotime, China). Cells were rinsed with PBS and fixed in 4% paraformaldehyde and then stained with BCIP/NBT solution for 20 min in dark at room temperature. ALP-positive cells were indicated by dark purple staining under the light microscope (Olympus IX73, Japan).
Alizarin Red Staining
After 4-week osteogenic induction, the formation of mineralized nodule was detected by Alizarin Red staining. Cells were fixed with 4% paraformaldehyde for 30 min and rinsed with PBS, and then stained with 0.1% Alizarin Red (Sigma, USA) for 10 min at room temperature. Next, the mineralized nodule was observed by light microscope (Olympus IX73, Japan).
Western Blotting
Proteins from whole-cell lysates were extracted in RIPA buffer (Solarbio, China) containing 1% PMSF (Solarbio, China). The protein concentration was determined by BCA assay kit (Cwbio, China) according to the manufacturer’s protocol. Protein extracts were separated by 10% SDS-PAGE, transferred onto a PVDF membrane, and then incubated at 4°C overnight with primary antibodies RUNX2 (1:1000, CST, USA), COL1 (1:1000, CST, USA), BGP (1:1000, CST, USA), VDR (1:1000, CST, USA) and GAPDH (1:10,000, Proteintech, USA). After the successful binding of HRP-conjugated secondary antibody (1:20,000) to primary antibodies, immunoreactive bands were detected by the ECL chemiluminescence detection system and the gray values were analyzed by ImageJ 1.8.0.
Reverse Transcription-Quantitative PCR (RT- qPCR)
Total cellular RNA was extracted with Trizol (Takara, Japan) and the mRNA was reverse transcribed to cDNA using a PrimeScript RT reagent Kit (Takara, Japan). RT‐qPCR assay was performed by SYBRGreen PCR Core Kit (Takara, Japan) according to the manufacturer’s protocol: one cycle of 95℃ for 30s, followed by 40 cycles of 95℃ for 5s and 60℃ for 20s. Relative expression levels of target genes were calculated using the 2-ΔΔCT method [29], normalizing with glyceraldehyde-3-phosphate dehydrogenase (GAPDH) levels. The sequences of primers used in this study were as follows: GAPDH, 5’-ACCACAGTCCATGCCATCAC-3’ and 3’-TCCACCACCCTGTTGCTGTA-5’ ; ALP, 5’-CATCATGTTCCTGGGAGATG-3’ and 3’-GGTGGTGTACGTCTTGGAGA-5’.
Intracellular ROS Measurement
The level of intracellular ROS was measured by peroxide‐dependent oxidation of 2′‐7′‐dichlorofluorescein‐ diacetate (DCFH‐DA) (Beyotime, China). The osteoblasts were stained with 10μM DCFH-DA for 20 min at 37℃ under dark condition. The images were randomly obtained by an inverted microscope (Olympus IX71, Japan).
Measurements of SOD Activity and Malondialdehyde
The activity of SOD was analyzed by the Total Superoxide Dismutase Assay Kit (Beyotime, China) according to the manufacturer’s instructions. Values of malondialdehyde (MDA) in the supernatants were measured strictly following the manufacturer’s protocol (Beyotime, China).
Statistical Analysis
Statistical analysis was conducted by SPSS 20.0
and GraphPad Prism 8. The results are given as the mean ± standard deviation (SD) of three to five independent experiments. Data were analyzed by one-way ANOVA or the Student’s two-tailed t-test. Differences were considered statistically significant when P<0.05.
Results
1,25VD3 Decreased Effectively FBG and Maintained Body Weight
Before STZ administration, the blood glucose level of all rats were within the normal range. While after STZ injection, T2DM rats showed significantly greater blood glucose level than control rats (P < 0.05). Since the second week, 1,25VD3 treatment showed positive effects on lowering blood glucose in T2DM rats (P < 0.05), but still higher compared with normal rats in control group (P < 0.05) (Table 1).
Changes on body weight of all experiment rats were presented in Table 1. The body weight of T2DM rats was significantly decreased after the administration of STZ compared with controls (P < 0.05), while the application of 1,25VD3 helped mitigate the weight loss in diabetic rats (P < 0.05).
| Group | Fasting blood glucose (mmol/L) | |||||||
|---|---|---|---|---|---|---|---|---|
| 0 day | 7th day | 2 weeks | 4 weeks | 6 weeks | 8 weeks | 10 weeks | 12 weeks | |
| Control | 4.5±0.2 | 4.6±0.3*# | 4.7±0.2*# | 4.5±0.2*# | 4.7±0.3*# | 4.6±0.2*# | 4.6±0.3*#·· | 4.7±0.2*# |
| T2DM | 4.6±0.3 | 19.5±1.5 | 23.4±1.7 | 24.7±1.8 | 23.7±1.6 | 24.9±2.2 | 24.3±1.2 | 24.3±1.1 |
| 1,25VD - 3 treated T2DM | 4.6±0.3 | 16.9±1.5 | 14.7±1.3* | 13.7±0.8* | 11.1±1.1* | 9.5±0.5* | 10.1±0.8* | 10.5±0.9* |
Table 1: Effect of 1,25VD3 on fasting blood glucose levels in experimental rats (n =5/group).
n = 3/group, *P < 0.05, data are presented as mean ± SD. 0 day represented before STZ inducement, 7th day and 2-12 weeks represented after 1,25VD3 treatment, *: P < 0.05, for T2DM vs. other two group, #: P < 0.05, for 1,25VD3-treated T2DM vs. Control, data are presented as mean ±SD. Table 1: Effect of 1,25VD3 on fasting blood glucose levels in experimental rats (n =5/group).
1,25VD3 Inhibited the Level of Oxidative Stress in T2DM Rats
As shown in Figure 1, the level of oxidant biomarker 15-F2t-IsoP was significantly increased in untreated T2DM rats and was relegated to nearly normal range by 1,25VD3 treatment (P < 0.05). While as an antioxidant parameter, the SOD activity showed a contrary tendency. These results implied that 1,25VD3 might carry on its effect through inhibiting oxidative stress.
1,25VD3 Improved Implant Osseointegration in T2DM Rats
3D micro-CT images depicted and compared the peri- implant trabecular microstructures among different groups (Figure 2A). The bone trabecula of T2DM rats were clearly thinner and fewer than controls. Notably, 1,25VD3 treatment could improve the structure of bone trabecula and implant osseointegration in model rats. Furthermore, the results of quantitative evaluation also demonstrated the statistically significant differences between T2DM group and 1,25VD3- treated group (Figures 2B-F).
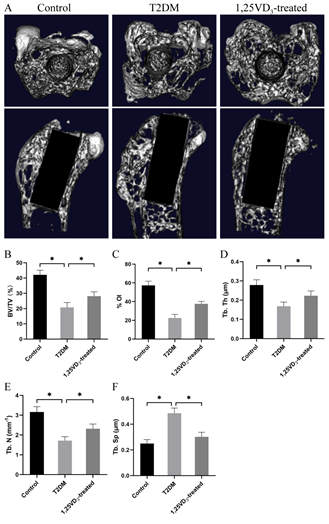
Figure 2: 1,25VD3 improved bone quality of T2DM rats. Micro-CT images of femur with implants (A) and quantitative results of micro-CT evaluation (B, C, D, E and F). (A) The upper column showed transverse 3D images through cross-sectional plane of implants, and the lower column exhibited coronary 3D images through the central portion of the long axis of implants; (B) BV/TV: ratio of bone tissue volume to total tissue volume; (C) %OI: ratios between bone and total voxels in direct contact with the implant; (D) Tb. Th: the mean trabecular thickness; (E) Tb. N: the mean trabecular number; (F) Tb.Sp: the mean trabecular separation, n = 5 specimens/group, *P < 0.05, data are presented as mean ± SD.
The BV/TV, %OI, Tb. Th and Tb. N showed the same tendency that these indicators were remarkably decreased in T2DM group while increased by the 1,25VD3 treatment. Inversely, 1,25VD3 treatment decreased the Tb. Sp by 37.8% in contrast with untreated T2DM rats.
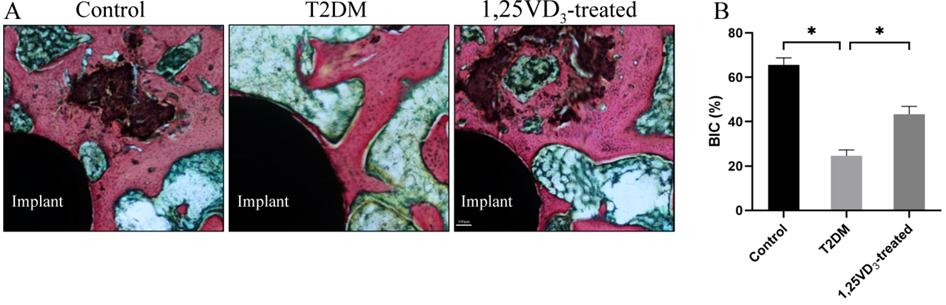
Staining slices showed the details of implant osseointegration and peri-implant bone microarchitecture (Figure 3A). The peri-implant bone mass was decreased and scattered in T2DM group and that was conspicuously ameliorated by the application of 1,25VD3. Results from histomorphometric analysis certified the manifestation of histomorphology. As shown in Figure 3B, the BIC of T2DM rats appeared as 24.6%, significantly less than controls and 1,25VD3-treated diabetic rats, which respectively had 65.6% and 43.4% BIC (P < 0.05).
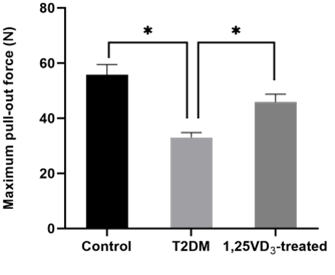
The biomechanical properties and the degree of osseointegration were examined by pull-out test. Compared with T2DM group, a significantly increase of maximum pull- out force by 1.4-fold was observed in 1,25VD3-treated group (P < 0.05) (Figure 4).
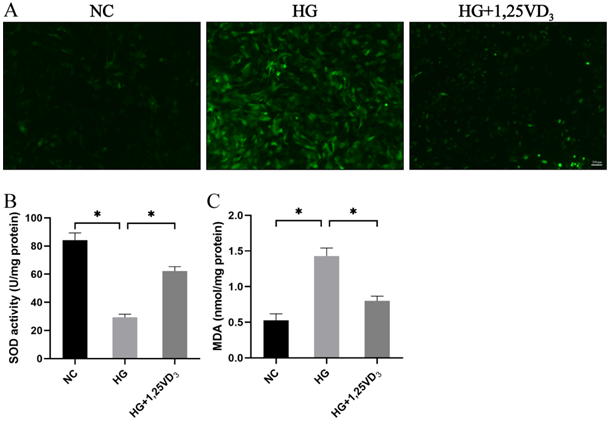
1,25VD3 Inhibited the Oxidative Status of Osteoblasts in High Glucose Conditions
The intracellular ROS level of osteoblasts was measured by fluorescent probe DCFH-DA staining. As shown in Figure 5A, the DCFH-DA fluorescence intensity of high glucose group was significantly increased as compared with control group. Whereas, the generation of ROS was significantly inhibited by 1,25VD3 (P < 0.05). Moreover, the oxidative stress-related biomarkers SOD activity and MDA were also detected to analyze the anti-oxidative effect of 1,25VD3. The SOD activity was significantly suppressed by high glucose concentration, and the declined SOD activity in high glucose environment was restored by the administration of 1,25VD3 (P < 0.05) (Figure 5B). As for the lipid peroxidation biomarker MDA, which is closely related with oxidative stress status of cells, was significantly increased in high glucose group but effectively decreased by 1,25VD3 (P < 0.05) (Figure 5C).
1,25VD3 Restored the OS-Mediated Damage in Osteogenesis
To further confirm the role of 1,25VD3 in osteogenesis under high glucose condition, we detected the Alizarin Red staining, ALP staining, gene expression levels of ALP and the expression of associated proteins in cells. After 7-day osteogenic induction, high glucose remarkably inhibited ALP activity, while significant higher ALP activity was detected in 1,25VD3-treated high glucose group as compared with high glucose group (P < 0.05)(Figure 6A). Similar tendencies were observed in Alizarin Red staining (Figure 6B), which was determined to evaluate the mineralized nodules after 4-week osteogenic induction. Less calcium nodules were found in HG group (P < 0.05), while 1,25VD3 treatment promoted the calcium deposition and mineralized nodules formation in high glucose environment. Besides, results pf gene and protein expression profiling pointed toward the same trend (Figures 6C-H).
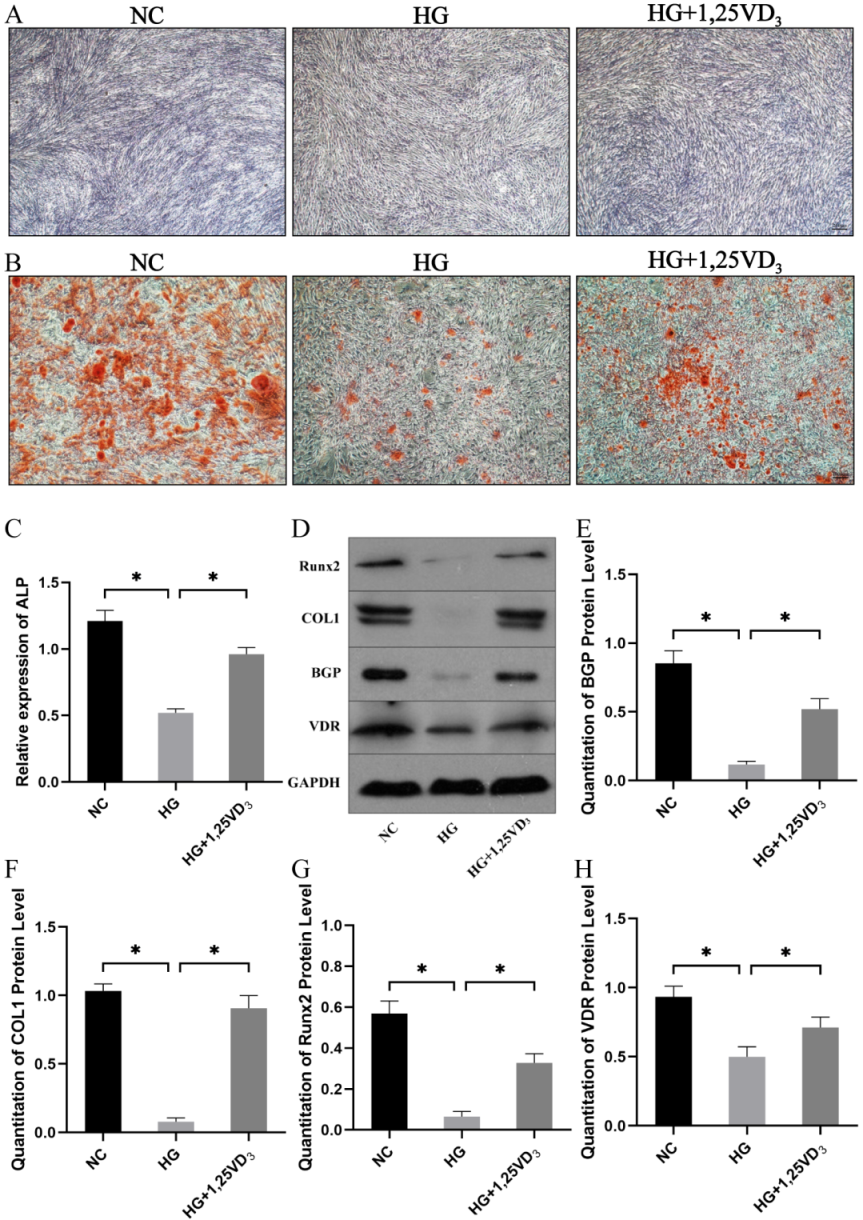
Figure 6: 1,25VD3 restored the OS-mediated damage in osteogenesis. (A)Representative ALP staining images (scale bar: 200 μm); (B) Representative Alizarin Red staining images (scale bar: 1000 μm); (C) Gene expression levels of ALP after 7-day induction; (D, E, F, G and H) Protein expression levels of RUNX2, COL1, BGP and VDR assessed by Western blot and the quantification analysis.
Discussion
In the present study, the hyperglycemia of rats was induced by high-glucose and high-fat diet with low-dose STZ injection, which is described to closely resemble T2DM [30]. We successfully established the T2DM model that the increased fasting blood glucose level and decreased body weight are similar to previous reports [31]. The adverse effects of T2DM on implant osseointegration have been widely studied, and the reduction of bone mineral content and impairment of bone healing and remolding in T2DM patients and rodents has been confirmed by previous experiments [32, 33]. Results of histological evaluation, micro-CT scanning and biomechanical analysis in our study demonstrated that the implant osseointegration, bone microarchitecture and implant fixation were significantly reduced in untreated T2DM rats.
It is well known that VD3 plays an important role in bone mineral homeostasis and maintaining glucose homeostasis. In our study, the 1,25VD3-treated T2DM rats showed a statistically significant decrease of blood glucose level and elevation of body weight compared to untreated T2DM rats. These findings confirm the ability of maintaining glucose homeostasis of 1,25VD3 as reported in previous studies [34], and also explain the result of micro-CT, histological staining and pull-out test which indicated that 1,25VD3 therapy could obviously promote the bone formation and reconstruction around implant and reverse the impaired osseointegration capacity to a certain extent in diabetic rats. Whereas, there was still a certain difference between the 1,25VD3-treated rats and the normal rats. This might be the result of uncontrolled hyperglycemia condition, in which 1,25VD3 couldn’t play its largest role in bone remodeling and glucose homeostasis [35]. These findings in our study are in accordance with the results in Wu’s [22] study, in which the effect of reversing the impaired osseointegration capacity of VD3 treatment in diabetic rats was firstly reported while the related mechanism was not illuminated.
To figure out the possible mechanism of this therapeutic effect, our group has done a host of researches. Our previous research had confirmed that 1,25VD3 promoted osseointegration of implant via downregulating AGEs/ RAGE pathway in T2DM [36]. Given the complex and diverse mechanism of 1,25VD3 on osseointegration, in this study, we verified the effect of 1,25VD3 on oxidative stress, which has been widely considered as an important role in the development of diabetic bone loss [10, 37]. Hamada et al. found that STZ-induced diabetic rats had low-turnover osteopenia associated with increased oxidative stress and the markers of oxidative stress were inversely associated with the histomorphometric parameters of bone formation [10]. As is well established, diabetes promotes oxidative stress through the production of ROS [20]. Several studies have demonstrated the involvement of ROS in modulating redox-sensitive signaling pathways that play major roles in bone cell differentiation, including mitogen-activated protein kinases (MAPKs) and Wnt/ β-catenin. Lee et al. showed that osteoclast differentiation stimulated by RANKL was mediated by ROS production and the subsequent activation of JNK, p38 and ERK1/2 [38]. By diverting the pool of β-catenin, ROS inhibited Wnt-induced osteoblastic gene expression and played a role in causing increased osteoblast and osteocyte apoptosis [39]. Results showed that the increased generation of ROS in high glucose condition was significantly inhibited by 1,25VD3. It has been widely reported that patients with T2DM show a decrease in antioxidant defenses and an increase in oxidative damage markers [40]. Data in present study corresponded with the foregoing research. All the results indicated that these positive effects of 1,25VD3 on bone metabolism may be achieved through the decline of oxidative stress.
Subsequently, we verified these findings by in vitro experiments. ALP staining, alizarin red staining, RT-qPCR and western blot were used to evaluate the osteogenic capacity of osteoblasts. ALP is an early osteogenesis marker that can mediate calcium phosphate into insoluble phosphate salts which is necessary for osteogenesis [41]. Alizarin red staining is one of the commonly used methods to observe the mineralized nodules, which are the markers of maturation of osteogenesis. Data showed that ALP activity of osteoblasts was inhibited and the malnourished mineralized nodules was observed in high glucose condition, while the application of 1,25VD3 could attenuate these adverse effects. Moreover, the relative mRNA expression of ALP and the translation level of osteogenic proteins such as BGP, COL1 and Runx2 obtained similar results. Besides, research has certified that high glucose indirectly down-regulates VDR expression in osteoblasts and weakens osteoblasts response to 1,25VD3 [42]. In the present study, high glucose suppresses the expression of VDR, which can be rescued by 1,25VD3 treatment. These evidences prove that the impaired cell differentiation caused by high glucose can be improved by 1,25VD3 treatment. Taken together, the results of this study reveals the beneficial effect of 1,25VD3 on implant osseointegration in T2DM and expand our understanding of the effect mechanism in a new perspective. In brief, our results demonstrated that 1,25VD3 inhibited the production of ROS and oxidative stress, thus regulated glucose homeostasis and bone metabolism, and further promoted implant osseointegration. However, the definite molecular mechanism of the inhibitory effects of 1,25VD3 on oxidative stress remains to be further investigated.
Funding
This work was supported by the Health Commission of Shandong Province (2019WS255), weifang science and technology bureau ( 2020YX006), the Health Commission of Weifang (WFWSJK-2020-049, WFWSJK-2020-078).
Authors contributions
ZH designed the experiment, CH listed the data systematically and wrote the manuscript; CH and LT performed the in vivo experiments; CH and FY performed the in vitro experiments; CH performed statistical analysis; ZH guided all aspects of this study. All the authors listed have approved the manuscript and agree to publish.
References
-
Naujokat H, Kunzendorf B, Wiltfang J (2016) Dental implants and diabetes mellitus-a systematic review. Int J Implant Dent 2(1): 5.
-
Zheng Y, Ley SH, Hu FB (2018) Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol 14(2): 88-98.
-
Forbes JM, Cooper ME (2013) Mechanisms of diabetic complications. Physiol Rev 93(1): 137-188.
-
Lee MS (2014) Role of innate immunity in the pathogenesis of type 1 and type 2 diabetes. J Korean Med Sci 29(8): 1038-1041.
-
Casap N, Nimri S, Ziv E, Sela J, Samuni Y (2008) Type 2 diabetes has minimal effect on osseointegration of titanium implants in Psammomys obesus. Clin Oral Implants Res 19(5): 458-464.
-
Oates TW, Huynh-Ba G, Vargas A, Alexander P, Feine J (2013) A critical review of diabetes, glycemic control, and dental implant therapy. Clin Oral Implants Res 24(2): 117-127.
-
Akash MSH, Rehman K, Chen S (2013) Role of inflammatory mechanisms in pathogenesis of type 2 diabetes mellitus. J Cell Biochem 114(3): 525-531.
-
Rehman K, Akash MSH (2016) Mechanisms of inflammatory responses and development of insulin resistance: how are they interlinked? J Biomed Sci 23: 87.
-
Mody N, Parhami F, Sarafian TA, Demer LL (2001) Oxidative stress modulates osteoblastic differentiation of vascular and bone cells. Free Radic Biol Med 31(4): 509-519.
-
Hamada Y, Fujii H, Fukagawa M (2009) Role of oxidative stress in diabetic bone disorder. Bone 45(1): 35-38.
-
Bai XC, Lu D, Bai J, Zheng H, Ke Z, et al. (2004) Oxidative stress inhibits osteoblastic differentiation of bone cells by ERK and NF-kappaB. Biochem Biophys Res Commun 314(1): 197-207.
-
Fatokun AA, Stone TW, Smith RA (2006) Hydrogen peroxide-induced oxidative stress in MC3T3-E1 cells: The effects of glutamate and protection by purines. Bone 39(3): 542-551.
-
Chen RM, Wu GJ, Chang HC, Chen JT, Chen TF, et al. (2005) 2,6-Diisopropylphenol protects osteoblasts from oxidative stress-induced apoptosis through suppression of caspase-3 activation. Ann N Y Acad Sci 1042: 448-459.
-
Hamada Y, Fujii H, Kitazawa R, Yodoi J, Kitazawa S, et al. (2009) Thioredoxin-1 overexpression in transgenic mice attenuates streptozotocin-induced diabetic osteopenia: a novel role of oxidative stress and therapeutic implications. Bone 44(5): 936-941.
-
Murray CE, Coleman CM (2019) Impact of Diabetes Mellitus on Bone Health. Int J Mol Sci 20(19): 4873.
-
Plum LA, DeLuca HF (2010) Vitamin D, disease and therapeutic opportunities. Nat Rev Drug Discov 9(12): 941-955.
-
Sergeev IN (2016) 1,25-Dihydroxyvitamin D3 and type 2 diabetes: Ca2+-dependent molecular mechanisms and the role of vitamin D status. Horm Mol Biol Clin Investig 26(1): 61-65.
-
Pérez López FR (2007) Vitamin D and its implications for musculoskeletal health in women: an update. Maturitas 58(2): 117-137.
-
Rapuri PB, Gallagher JC, Nawaz Z (2007) Caffeine decreases vitamin D receptor protein expression and 1,25(OH)2D3 stimulated alkaline phosphatase activity in human osteoblast cells. J Steroid Biochem Mol Biol 103(3-5): 368-371.
-
Maxwell CS, Wood RJ (2011) Update on vitamin D and type 2 diabetes. Nutr Rev 69(5): 291-295.
-
Song Y, Wang L, Pittas AG, Gobbo LC, Zhang C, et al. (2013) Blood 25-hydroxy vitamin D levels and incident type 2 diabetes: a meta-analysis of prospective studies. Diabetes Care 36(5): 1422-1428.
-
Wu YY, Yu T, Yang XY, Li F, Ma L, et al. (2013) Vitamin D3 and insulin combined treatment promotes titanium implant osseointegration in diabetes mellitus rats. Bone 52(1): 1-8.
-
Li Y, Zou S, Wang D, Feng G, Bao C, et al. (2010) The effect of hydrofluoric acid treatment on titanium implant osseointegration in ovariectomized rats. Biomaterials 31(12): 3266-3273.
-
Elattar S, Estaphan S, Mohamed EA, Elzainy A, Naguib M (2017) The protective effect of 1alpha, 25-dihydroxyvitamin d3 and metformin on liver in type 2 diabetic rats. J Steroid Biochem Mol Biol 173: 235-244.
-
Gao Y, Luo E, Hu J, Xue J, Zhu S, et al. (2009) Effect of combined local treatment with zoledronic acid and basic fibroblast growth factor on implant fixation in ovariectomized rats. Bone 44(2): 225-232.
-
Jonason JH, O Keefe RJ (2014) Isolation and culture of neonatal mouse calvarial osteoblasts. Methods Mol Biol 1130: 295-305.
-
Fang WJ, Wang CJ, He Y, Zhou YL, Peng XD, et al. (2018) Resveratrol alleviates diabetic cardiomyopathy in rats by improving mitochondrial function through PGC-1α deacetylation. Acta Pharmacol Sin 39(1): 59-73.
-
Xiong Y, Zhang Y, Xin N, Yuan Y, Zhang Q, et al. (2017) 1α,25-Dihydroxyvitamin D promotes bone formation by promoting nuclear exclusion of the FoxO1 transcription factor in diabetic mice. J Biol Chem 292(49): 20270- 20280.
-
Livak KJ, Schmittgen TD (2001) Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 25(4): 402-408.
-
Srinivasan K, Viswanad B, Asrat L, Kaul CL, Ramarao P (2005) Combination of high-fat diet-fed and low-dose streptozotocin-treated rat: a model for type 2 diabetes and pharmacological screening. Pharmacol Res 52(4): 313-320.
-
Furman BL (2015) Streptozotocin-Induced Diabetic Models in Mice and Rats. Curr Protoc Pharmacol 70: 5.
-
Napoli N, Chandran M, Pierroz DD, Abrahamsen B, Schwartz AV, et al. (2017) Mechanisms of diabetes mellitus-induced bone fragility. Nat Rev Endocrinol 13(4): 208-219.
-
Li G, Prior JC, Leslie WD, Thabane L, Papaiannou A, et al. (2019) Frailty and Risk of Fractures in Patients With Type 2 Diabetes. Diabetes Care 42(4): 507-513.
-
El Fakhri N, McDevitt H, Shaikh MG, Halsey C, Ahmed SF (2014) Vitamin D and its effects on glucose homeostasis, cardiovascular function and immune function. Horm Res Paediatr 81(6): 363-378.
-
Del Pino Montes J, Benito GE, Fernández Salazar MP, Covenas R, Calvo JJ, et al. (2004) Calcitriol improves streptozotocin-induced diabetes and recovers bone mineral density in diabetic rats. Calcif Tissue Int 75(6): 526-532.
-
Jia T, Wang Y-N, Zhang D, Xu X (2018) 1α,25- dihydroxyvitamin D3 promotes osseointegration of titanium implant via downregulating AGEs/RAGE pathway in T2DM. Endocr Connect 7(11): 1186-1195.
-
Giacco F, Brownlee M (2010) Oxidative stress and diabetic complications. Circ Res 107(9): 1058-1070.
-
Lee NK, Choi YG, Baik JY, Han SY, Jeong DW, et al. (2005) A crucial role for reactive oxygen species in RANKL- induced osteoclast differentiation. Blood 106(3): 852- 859.
-
Manolagas SC, Almeida M (2007) Gone with the Wnts: beta-catenin, T-cell factor, forkhead box O, and oxidative stress in age-dependent diseases of bone, lipid, and glucose metabolism. Mol Endocrinol 21(11): 2605-2614.
-
Kasznicki J, Kosmalski M, Sliwinska A, Mrowicka M, Stanczyk M, et al. (2012) Evaluation of oxidative stress markers in pathogenesis of diabetic neuropathy. Mol Biol Rep 39(9): 8669-8678.
-
Halling Linder C, Ek Rylander B, Krumpel M, Norgard M, Narisawa S, et al. (2017) Bone Alkaline Phosphatase and Tartrate-Resistant Acid Phosphatase: Potential Co-regulators of Bone Mineralization. Calcif Tissue Int 101(1): 92-101.
-
Ghodsi M, Larijani B, Keshtkar AA, Nasli Esfahani E, Alatab S, et al. (2016) Mechanisms involved in altered bone metabolism in diabetes: a narrative review. J Diabetes Metab Disord 15: 52.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells