Crab Transpalatal Arch – A Clinical Innovation
Choosing an appliance for any orthodontic treatment now mostly depends on its usefulness. Transpalatal arch is one such appliance with benefits when used in fixed orthodontic treatment. The aim of this article is to present a modification of TPA and their used in bilateral impacted canine used in different cases as a modification.
Introduction
Clinical orthodontics frequently use of transpalatal arches. The TPA’s adaptability makes it a very helpful to both traditional and modern fixed appliance therapy. During fixed appliance orthodontic treatment, the maxillary molars are connected with a stainless-steel wire called the transpalatal arch to help anchorage reinforcement (Figure 1).
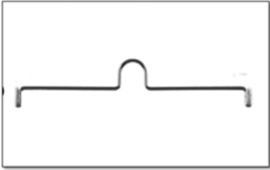

TPA was introduced by Robert Goshgarian [1] (Figure 2) which was a transpalatal arch to connect contralateral maxillary permanent molar made by using 18-to-20-gauge stainless steel wire (0.9 mm to 1.25 mm). The wire can be stabilized by either soldering directly to molar bands or indirectly by engaging into the lingual sheath welded to molar bands [2]. The advantages of using lingual sheath is that it can be removable without removing molar bands (which will otherwise requires recommendation). The lingual sheaths used is also known as Wilson tubes.
Uses of TPA
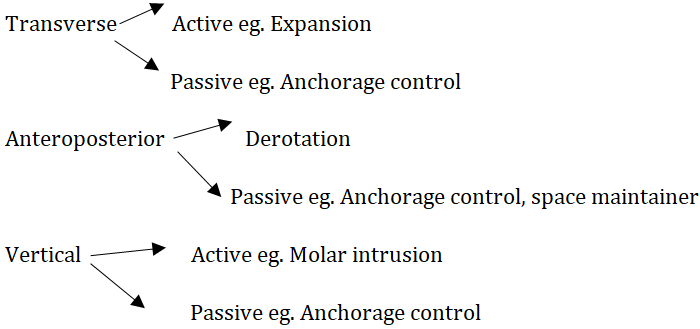
Advantages of TPA
- Can produced molar rotations and changes in root torque.
- Rotational molar correction.
- Upper molars’-controlled eruption.
- For maxillary expansion.
- Correct molar crossbites.
- Correct asymmetries mesiodistally.
- Prevent mesial migration of upper 1st molar during the transition from II deciduous molar to the second premolar.
- Maintain and stabilise arch widths.
- Intrusion of molar.
- Act as a space maintainer.
- For unilateral distalization of molars.
Disadvantages of TPA
- Breakage and cement failure.
- Oral hygiene difficulties.
- Poor patient tolerance.
- Interrupting on the palatal mucosa.
- Discomfort to the patient during eating.
The Nance appliance
Nance palatal arch introduced by Nance in 1947. Nance palatal arch (Figure 3) was one of the modifications of the TPA. An anterior acrylic button connects the palatal wire to the molar bands after they have been welded or soldered together. In the Indications for transpalatal, Nance TPA has great versatility. N TPA is one of the most commonly used appliances known for its versatility usages act not only as a independent appliances but also in combination with various fixed and functional appliances as well as combination with minor modification and or will banding can be incorporated in the appliances for case specific usage [3, 4].

Other auxiliary or attachment. The button which rests on palatal mucosa can be constructed from cold cure, heat cure or a light cure acrylic.
In pendulum appliance Nance palatal arch used to provide anchorage to distalize the molars, or rapid molar distalization. After distalization has been achieved, the Nance appliance is replaced by TPA to maintain the molar position.
Case Report – Showing Management of Impacted Canine by Modification of TPA/ Nance Button
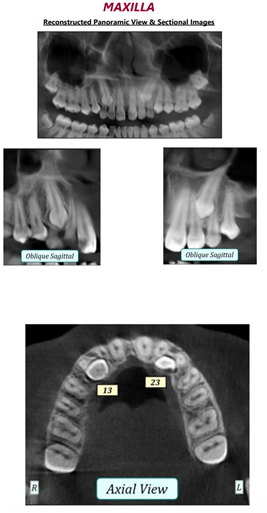
A 22-year- young female came to the department with the chief complains of Spacing in upper front teeth region. Presented with an Angle’s Class I molar relation on right side and End on molar relation on left side. She had a mesoprosopic facial form with a convex profile and a non-consonant smile and an unerupted upper right and left permanent canine (Figures 4-14). A bulge was present on labial alveolar mucosa in distal area with respect to right & left maxillary incisors which was hard on palpation. Orthopantomograph (OPG) showed impacted right &left maxillary canine.
Pre – Treatment Extra- Oral Photographs.

$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$

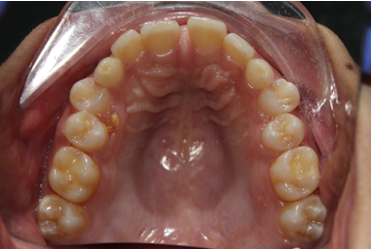
Pre- Treatment Intra- Oral Photographs.






Treatment Approach
After studying the diagnostic records, we decide to extract 53, 63, 83 and decided finger like extension in TPA / Nance button and allow to eruption of impacted maxillary canines along with fixed mechanotherapy. Finger like extension on both the sides (Figures 15 & 16) in the deciduous canine spaces for maintaining space and also space regaining which facilitates permanent canine eruption.


Appliance Construction and Clinical Steps
- Separators placement for 6−8 days for molar bands.
- Because the band’s lumen can decrease during laboratory welding and soldering procedure, use bands that are one size larger when making your selection.
- The bands are then adjusted within the impression, which is subsequently decontaminated before being transported to the lab.
- Impression with molar band transpalatal arch is welding/soldering after soldering transpalatal arch fixed with glass ionomer cements on upper maxillary 1st molars.
- After completing lab procedure that includes soldering, acrylization, finishing and poshing the appliance is finally ready for insertion in patient’s mouth.
- After appliance is placed in patient’s mouth it is then cemented and activation of spring is done with fixed mechanotherapy.
Status of the Case
After delivering the appliance patient is recalled every month for orthodontic visit. In order to view the status of the case OPG (Figure 17) and intraoral photograph (maxillary occlusal view) (Figure 18) is taken after six months which shows canine eruption in the same.


Discussion
TPA & Nance palatal arch uses in daily orthodontic treatment. They can be used for everything from anchoring control for difficult malocclusions to interceptive applications. A Dahlquist, et al. [5] studied effect of TPA on first molar rotation and it was found that transpalatal arch is effective in derotation of maxillary first molar accompanied by a slight expansion in majority of cases. A large derotation results in contraction. According to Braun [6] application of TPA can gain 2.1mm of arch length as it can exert a distal force which is equivalent to maxillary 1st molar centre of resistance. Asymmetric TPA for molar intrusion Riddhi & Prasad Sin [7, 8] modified TPA with asymmetric arms for intrusion of molar (mTPA). The shorter arm was engaged to the palatal sheath of the molar to be intruded, so that the appliance lies at 4 mm from palate.
Conclusion
This crab modification of TPA appliance work with fixed mechanotherapy to reduce overall treatment time. This modification helps in space maintaining along with space regaining. Facilitates canine eruption by providing space naturally. This modification can be used in any other treatment plan.
References
-
Goshgarian RA (1972) Orthodontic palatal arch wires. United States Government Patent Office.
-
Gunduz E, Zachrisson BU, Honigl KD, Crismani AG, Bantleon HP (2003) An improved transpalatal bar design. Part I. Comparison of moments and forces delivered by two bar designs for symmetrical molar derotation. Angle Orthod 73(3): 239-243.
-
Cobo JM, Diaz B, Carlos F de (1998) Maintaining anchorage with a combination Nance-Goshgarian transpalatal arch. Journal of clinical orthodontics 32(11): 681.
-
Massimiliano M, Laura B (2001) Asymmetric Distalization with a TMA Transpalatal Arch. J ClinOrthod 35(3): 174-178.
-
Dahlquist A, Gebauer U, Ingervall B (1996) The effect of a transpalatal arch for the correction of first molar rotation. Eur J Orthod 18(3): 257-267.
-
Braun S, Kusnoto B, Evans C (1997) The effect of maxillary molar derotation on arch length. Am J Orthod Dentofacial Orthop 112(5): 538-544.
-
Riddhi, Prasad S (2015) Molar intrusion with asymmetrical MTPA. International Journal of Oral Health Dentistry, October – December 1(4): 190-193.
-
Lyka I, Carlsson GE, Wedel A (2001) Dentists’ perception of risks for molars without antagonists. A questionnaire study of dentists in Sweden. Swed Dent J 25(2): 67-73.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells