An Alternative Technique for Ridge Reconstruction of Extraction Socket with Buccal Dehiscence: A Clinical Case Report
A clinical case report describing the use of an alternative ridge reconstruction technique to augment an extraction socket with buccal dehiscence. Unassisted healing following flapless extraction of teeth possessing such buccal wall defects leads to severe bone and soft tissue deformities, and an aesthetic compromise. Current treatment strategies are based on the assumption that maintenance of the buccal tissues leads to superior clinical outcomes. Our proposed ridge reconstruction technique challenges this concept by suggesting that a lack of buccal bone in fact, enhances bone augmentation with our proposed treatment strategy, as demonstrated by the positive radiographic changes. Our technique consists of socket grafting with deproteinised bovine bone particulates and socket sealing with an immediate ovate pontic. The ability to achieve effective circumferential socket seal is paramount in maximising ridge augmentation. The increase in bone volume thus provides the ideal surgical environment for implant placement in the prosthetically driven position, ensuring optimal aesthetics and function of the implant. The patients also benefit from the provision of an immediate tooth replacement and the reduced postoperative morbidity as this is a flapless technique, involving no sutures or barrier membranes. The ultimate result is the ability to achieve superior clinical outcomes with maximum benefit for the patients.
Introduction
Alveolar ridge resorption results in significant crestal height reduction of the buccal and lingual walls, as well as reduction of the ridge width from the outer surface inwards [1]. Bone remodelling results in a mean horizontal ridge with reduction of 4mm and crestal height reduction fo 1.5mm, [2] with two-third of bone loss occurring within the first 3 months [3]. The implications of postextraction dimensional changes include insufficient bone for implant placement, significant gingival recession, midfacial collapse resulting in mucogingival deformities and an aesthetic compromise.
Thus, alveolar ridge preservation (ARP) techniques have been designed to attenuate the post-extraction dimensional changes, by preserving the height and width of the alveolar ridge. An expert evidence-based workshop in periodontology acknowledged that although no specific ARP approach has been proven to be patently superior, the application of a bone grafting material to fill the fresh extraction socket and sealing the socket orifice using an autogenous or exogenous barrier was strongly recommended [4, 5].
Buccal dehiscence poses additional challenges for socket management and requires ridge reconstruction procedures to augment the hard and soft tissues 3 -dimensionally. Ridge reconstruction techniques typically involve the placement of a barrier membrane for space maintenance to prevent unwanted apical migration of the epithelium into the wound and socket grafting using materials such as autogenous bone, allograft, xenograft or allograft materials [6]. The literature is however scanty with regards to evidence-based protocols for the management of compromised extraction sockets containing bony dehiscence.
Current existing treatment strategies to manage extraction socket with buccal dehiscence is based on the assumption that the preservation of buccal tissues leads to superior clinical outcomes. The “ice-cream cone technique” has been commonly performed in the past to reconstruct the buccal wall by inserting a collagen barrier membrane shaped in the form of an ice-cream cone to cover the bone graft material [7]. However, the handling of the barrier membrane is technique sensitive, requiring flap elevation, suturing and often a re-entry procedure is needed if nonabsorbable barrier membrane is used. Additionally, membrane exposure is not uncommon, and this increases the risk of wound healing complications [8].
Similarly, the socket shield technique was developed to allow partial root retention of the buccal aspect to preserve the buccal tissue and thus, enable the immediate implant to be placed in an optimal position [9]. However, there is still some amount of ridge height loss and loss of buccal ridge contour. The SocketKAP and SocketKAGE are respective non-resorbable and resorbable devices designed to support sockets with buccal dehiscence [10]. However, the lack of prospective well-designed randomised clinical trials examining these techniques means that none of the treatment strategies have yet been recommended for the management of extraction sockets with dehiscence [11].
Recently proposed ridge reconstruction techniques included socket sealing with non-absorbable membrane (dPTFE) and socket grafting with allogenic bone particulate [12]. They report an increase in mid-buccal crestal height of 5.7mm and an overall increase in total bone volume of 9%. However, the current scientific evidence does not provide guidelines as to which technique and which biomaterial will results in the most favourable clinical outcomes, and there is no evidence to suggest which technique is superior [5].
In this clinical case report, we proposed an alternative ridge reconstruction technique consisting of socket grafting with deproteinised bovine bone and socket sealing with ovate pontic delivered immediately after extraction. The xenograft serves as a scaffold to promote bone augmentation while also providing a physical support for the surrounding soft tissue flap. The ovate pontic provides physical coronal containment of the graft material, soft tissue sealing by forming an epithelial attachment with the pontic, and a tooth replacement solution. The patient is also never left without a replacement solution during the interim treatment period. This technique also challenges the current clinical assumption regarding the importance of buccal tissue preservation by suggesting that a lack of buccal bone in fact, leads to enhanced bone augmentation with our proposed treatment strategy. The combination of the xenograft and ovate pontic promotes enhances bone augmentation, as demonstrated by the increase in radiographic bony infill and positive changes in radiographic buccal bony contour.
Clinical Report
A 37-year-old female patient presented with maxillary right first molar (#16) which was unrestorable and indicated for extraction (Figures 1A-C). Following discussion of various treatment options, it was decided that an implant solution would provide the ideal long-term restorative replacement for the tooth. The maxillary right second premolar (#15) had a failed root canal treatment and was diagnosed with apical periodontitis but considered restorable. The patient decided to maintain the #15 and consequently the tooth was retreated by a specialist Endodontist and internally restored with composite resin. Maxillary and mandibular preliminary impressions were taken using polyether impression material (Impregum, 3M) for study casts and the construction of the distal cantilever acrylic brige. Preoperative photographs, and a CBCT scan (iCAT Next Generation; Imaging Sciences International Inc.) were taken revealing a buccal fenestration (Figure 1C).
At the following appointment, subgingival debridement of #16 and the adjacent teeth was performed using both Gracey curettes (Hu-Friedy) and a piezo scaler (Piezo Master 700, EMS) under local anaesthesia (Lignocaine hydrochloride 2% and epinephrine 1: 80,000, Septodont). Crown preparation was performed on #15 to receive a distal cantilevered acrylic bridge (Figure 2).
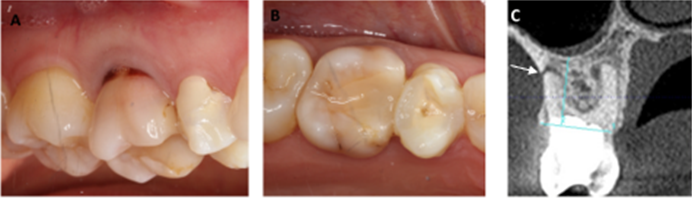
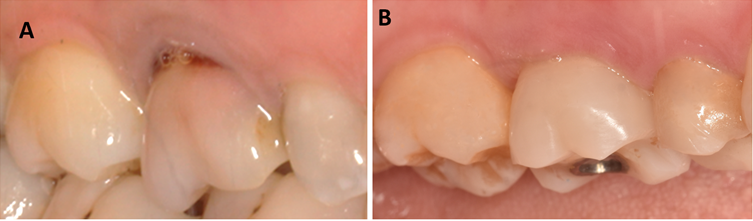
Figure 1: Baseline buccal and occlusal views of the maxillary right first molar (#16), indicated for extraction. #15 had a failed root canal treatment, and has been endodontically retreated and provisionally restored during the interim period (A,B). Cross- sectional view of baseline CBCT scan showed buccal fenestration of the #16. The while arrow points to the most apical part of the buccal defect.

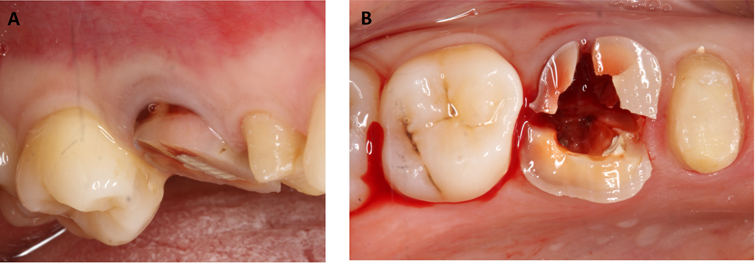
Minimally traumatic extraction of the tooth was performed utilizing a periotome (Periotome MSP 1F, Laschal) to ensure the integrity of the bone is maintained, and roots were carefully sectioned for a minimally traumatic extraction (Figures 3, 4A & B). Due to the presence of the buccal fenestration however, the slither of bone fractured revealing a buccal defecting measuring 11mm. The socket was debrided, irrigated with copious saline and inspected. The long term provisional was then tried-in, ovate pontic was relined with temporary composite (ProTemp 4, 3M) and the tissue -facing surface of the acrylic bridge was steam cleaned for 20 seconds (Touchsteam, Kerr).
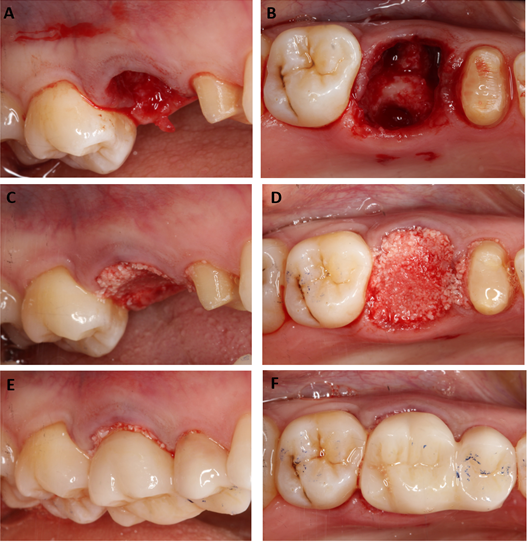
The socket was grafted with small particles of deproteinised bovine bone substitute (Bio-Oss granules, 0.25-1.0mm, Geistlich) up to the level of the free gingival margin (Figures 4 C,D). Consequently, the pre-fabricated long term provisional was bonded to the adjacent #15 using Temp Bond (Kerr) (Figures 4E, F). No sutures were needed. The patient was given detailed verbal and written postoperative instructions following surgery and prescriptions for ibuprofen 600mg every 6 hours for 3 days, co-amoxiclav 625mg every 8 hours for 7 days. The self-reported 100-point visual analogue score (VAS),13 which provides an indication of postoperative discomfort, at 1 week, 6 weeks and 6 months were 45, 8 and
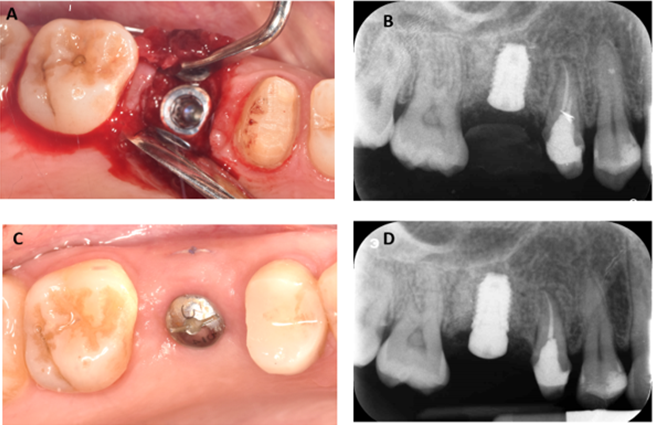
7, respectively. Healing at 8 weeks showed almost complete closure of the extraction socket. Approximately 6 months after alveolar ridge reconstruction, the socket was reviewed (Figure 5) which showed the extent of ridge augmentation in the horizontal dimension. The 6 months CBCT scan (Figure 6), revealing the extent of the buccal augmentation achieved. An 8.5x4.0mm (3i) implant was placed in the prosthetically driven position (Figures 7A, B), followed by the installation of the healing abutment at 3 months (Figures 7C, D) and fitting of the provisional restoration (Figure 8). The final review at 1 year showed optimal restorative emergence profile and soft tissue aesthetics (Figure 9).
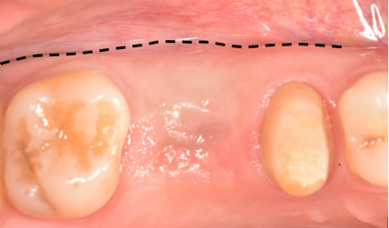
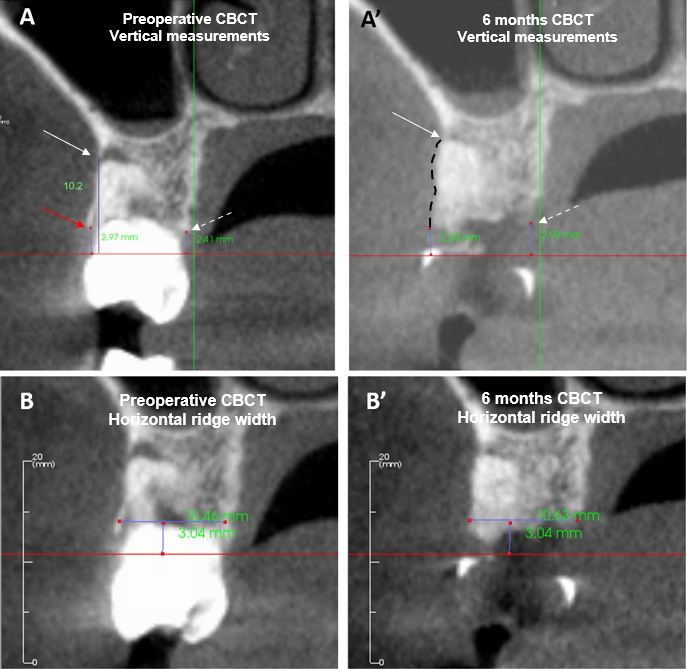
Figure 6: Preoperative CBCT (A, B) and at 6 months CBCT (A’, B’) were used for linear and horizontal measurements. The 6 months cross-sectional CBCT scan showed buccal augmentation (black dashed line) and infill to the apex of the buccal defect (A, arrowed). To anticipate the fracture of the coronal buccal plate during extraction (red arrow), the preoperative BRH was measured from the CEJ to the most apical part of the buccal defect (white arrow). Therefore, the preoperative BRH was 10.2mm, and this increased to 2.53mm at 6 months (A, A’). The LRH was measured from the CEJ to the alveolar crest (dashed arrow), which measured 2.41mm preoperative, and increased to 2.90mm postoperatively (A, A’). The preoperative HRW was 10.46mm and postoperatively, this increased to 10.63mm (B, B’).

Radiographic Measurements
Linear Assessment
A blinded examiner evaluated the CBCT scans at baseline and 6 months and obtained measurements of horizontal ridge width, mid-buccal and mid-lingual height using a software package (InVivo v.5.3, Anatomage, San Jose, CA). To ensure accuracy and consistency in measurements, the preoperative and postoperative datasets were registered to using the same anatomical landmarks. Vertical measurements were accomplished by using the same global image angulation and reproducible anatomic landmarks on the adjacent teeth, such as the cement-enamel junction (CEJ) or crown margins, for maximum consistency between measurements. Horizontal ridge width measurements were made at approximately 3 mm apical to a line connecting the mid-facial zenith of the CEJ of both teeth adjacent to the extraction site (Figures 6B, B’). This methodologic decision was driven by clinical relevance since this is often the level at which the restorative platform of a standard bone level implant is placed.
Volumetric Assessment
A blinded examiner performed the volumetric measurements. The pre-and postoperative CBCT images were superimposed to determine the changes in alveolar bone volume at 6 months. As the first CBCT scan is taken before the extraction, the tooth of interest was “digitally extracted” from the Pre-Operative scan, and the datasets were registered so that the anatomical features are accurately superimposed. DICOM files were processed, and the volumetric measurement were analysed using the Mimics software (Materialise, Leuven, Belgium), by defining a constant volume of interest (VOI) for both pre-operative and post-operative datasets. The six boundaries of the volume of interest were a plane over the crestal bone, a plane over the root apex, a plane over the most external aspect of the buccal and lingual bony plates and an extension in both the mesial and distal direction of approximately 2 to 3 mm, for reference purposes to facilitate reliable comparative assessments. The same segmentation settings were used for both the baseline and 6-months DICOM files. The total volume of the VOIs was quantified via subtraction analysis to ascertain the percentage loss of volume that occurred over the 6 months.
Clinical Outcomes
Ridge reconstruction of the #16 resulted in an increase in keratinised tissue width (KTW) by 1mm (Table 1); a gain in mid-buccal crestal ridge height (BRH) and horizontal ridge width (HRW) of 7.70mm and 0.17mm respectively (Table 2). The percentage of initial alveolar bone volume remaining across zones 0-3mm, 3-6mm, 6-9mm, were 120%, 157% and 126% respectively (Table 2). The clinical and radiographic outcomes are summarised in Tables 1 and 2.
| Preoperative | Postoperative (6 months after tooth extraction) | |||||
|---|---|---|---|---|---|---|
| #15 | #16 (indicated for extraction and RR) | #16 (implant crown) | ||||
| Plaque Index (%) | 0 | 0 | 0 | 0 | 0 | 0 |
| Bleeding index (0%) | 0 | 0 | 0 | 0 | 0 | 0 |
| Midbuccal probing depth (mm) | 1 | 2 | 1 | 1 | 1 | 1 |
| Midbuccal Gingival recession (mm) | 0 | 1 | 1 | 0 | 0 | 0 |
| Gingival thickness (mm) | 1 | 1 | 1 | 1 | 1 | 1 |
| KTW (mm) | 3 | 3 | 3 | 3 | 4 | 3 |
| Need for grafting at implant placement | - | yes | - | No |
Table 1: Preoperative clinical outcomes and comparative postoperative values taken 6 months following minimally traumatic extract
| Linear | #16 | ||
|---|---|---|---|
| Preoperative (mm) | Postoperative (mm), 6months after tooth extraction | Difference (mm) | |
| Midbuccal crestal ridge height (BRH) | 10.2 | 2.5 | 7.67 |
| Midlingual crestal ridge height (LRH) | 2.41 | 2.9 | -0.49 |
| Horizontal ridge width (HRW) | 10.46 | 10.63 | 0.17 |
| Volumentric | #16 | ||
| Preoperative (mm3) | Postoperative (mm3), 6months after tooth extraction | % alveolar bone remaining | |
| 0-3mm | 54 | 65 | 120 |
| 3-6mm | 214 | 317 | 157 |
| 6-9mm | 283 | 357 | 126 |
Table 2: Linear and volumetric radiographic bone measurements for tooth #16. Preoperative and postoperative measurements taken 6
Discussion
Compromised extraction sockets with buccal dehiscence pose a series of unique surgical and restorative challenges, including insufficient bone for implant placement, significant gingival recession and midfacial collapse leading to mucogingival deformities and an aesthetic compromise. Existing treatment strategies including the “ice-cream cone” technique, [7] “socket- shield” technique, [9] socketKAP [10] and SocketKAGE [10] are aimed at maintaining the buccal tissues. We propose a paradigm shift in treatment concepts by suggesting that a lack of buccal bone in fact, results in enhanced bone augmentation with our proposed ridge reconstruction technique, as demonstrated by the positive radiographic changes.
Our proposed technique consists of deproteinised bone graft and an immediate ovate pontic. The bone graft provides a scaffold for bony infill as well as providing physical support for the soft tissue flap. The choice of deproteinised bovine bone is based on its osteoconductive properties which has been demonstrated in in vitro and in vivo studies [14]. While socket grafting alone prevented horizontal width reduction by 2.0mm [15]; vertical mid-buccal reduction by 1.70mm and mid-lingual reduction by 1.20mm, 3-6 months following the intervention, [15] the latest EFP consensus recommends the combination of socket grafting and socket sealing techniques [5].
The ovate pontic serves as the socket seal by stabilising and protecting the fibrin clot, containing the graft material and maintaining space for bone remodeling [16, 17]. In addition, the pontic physically supports the soft tissues, facilitating the soft tissue augmentation in the horizontal and vertical direction. In a recent pilot study, immediate placement of a fixed ovate pontic provisional restoration into an intact extraction socket without grafting showed mean horizontal ridge width dimensional change of 0.90mm and mean vertical crestal height change of 1.60mm and at 3 months, suggesting preservation of tissue contour [18].
The delivery of the immediate ovate pontic also has several advantages in that it is less technique sensitive, requiring no sutures, membranes and flap elevation. The simplicity of the technique translates to less chairside time and reduced postoperative patient morbidity, as demonstrated by low VAS scores for both patients. The ability to provide an immediate tooth replacement following extraction will improve the patient journey. Currently, there is no data to demonstrate the use of ovate pontic and deproteinised bovine bone grafts in achieving bone augmentation following tooth extraction.
In this report, we presented favourable clinical outcomes following alternative RR of #16 to manage a compromised extraction socket containing a buccal fenestration. The partially missing or absence of buccal bone enabled maximum bone augmentation to be achieved. This implies a paradigm shift in treatment concepts, as it was previously thought that the lack of buccal bone resulted in less favourable outcomes and required further complex surgical procedures to manage the dimensional bone loss than would otherwise occur [7, 10, 15].
RR of #16 resulted in a gain in HRW of 0.20mm, and an increase in BRH of 7.70mm, indicating an increase in linear bone in the horizontal and vertical dimensions (Table 2). This
is in stark contrast to the 1.80mm reduction in ridge width and 1.50mm in vertical height following ridge preservation procedures, [4] reinforcing that the latter merely attenuates post-extraction dimensional changes, whereas ridge reconstruction results in bone augmentation.
In particular, the BRH surpassed the mid-buccal crestal gain in height of 5.80mm following RR with nonabsorbable collagen membrane and allograft bone particulates [12]. This could be due to the absence of buccal bone as thin bone forming the fenestration fractured away during extraction. The buccal bone loss extended almost to the root apex, which contrasted to the average buccal dehiscence extending to the coronal third in the aforementioned article [12]. The absence of the buccal wall created more space for the soft tissue to expand, to achieve maximum bone augmentation.
Bone augmentation is also reflected in positive volumetric radiographic changes following ridge reconstruction. The crestal 3mm, which is most susceptible to postextraction dimensional changes, [10] showed 120% of the initial alveolar bone remaining, indicating an increase in bone volume after RR. An increase in bone volume was observed in zones 3-6mm and 6-9mm (Table 2). By contrast, comparable extraction sockets containing buccal dehiscences treated with RR comprising of SocketKAP and SocketKAGE devices showed 76% of the initial alveolar bone volume remained in the crestal 3mm, while zones 3-6mm and 6-9mm both showed 86% of the initial bone volume remaining [10]. This suggests bone volume attenuation, rather than bone augmentation demonstrated in our case.
In this case report, the adjacent #15 required a full coverage restoration which enabled the option of the cantilevered ovate pontic at the site of the #16. We recommend this technique where the extraction site is bound by at least one natural tooth. In cases where the adjacent natural tooth is minimally restored or non-restored, we recommend a Maryland style resin retained cantilever bridge which would require minimal preparation compared to conventional bridge designs [19].
Conclusion
Ridge reconstruction consisting of deproteinised bovine bone covered by ovate pontic may be used to manage sockets with severe buccal dehiscence to achieve maximum hard and soft tissue augmentation. The ultimate result is the provision of an ideal surgical environment for implant placement in the prosthetically driven position, optimising aesthetics and functionality for the patient, while reducing the need for future complex surgical procedures. However, randomised clinical trials are needed to demonstrate whether ridge reconstruction with ovate pontic and deproteinised bone graft results in superior clinical outcomes compared to other ridge reconstruction techniques.
• Acknowledgement: We greatly appreciate the support Dr Anthony Reynolds, who is a Medical Physics Expert, for his analysis of CBCT images. There are no conflicts of interests. No financial support was received for this manuscript.
• Conflict of interest statement: The authors declare no competing or financial interests.
References
-
Araújo MG, Lindhe J (2005) Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol 32(2): 212-218.
-
Van der Weijden F, Dell’Acqua F, Slot DE (2009) Alveolar bone dimensional changes of post-extraction sockets in humans: a systematic review. J Clin Periodontol 36(12): 1048-1058.
-
Schropp L, Wenzel A, Kostopoulos L, Karring T (2003) Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent 23(4): 313-323.
-
Vignoletti F, Matesanz P, Rodrigo D, Figuero E, Martin C, et al. (2012) Surgical protocols for ridge preservation after tooth extraction. A systematic review. Clin Oral Implants Res 23: 22-38.
-
Tonetti MS, Jung RE, Avila-Ortiz G, Blanco J, Cosyn J, Fickl S, et al. (2019) Management of the extraction socket and timing of implant placement: Consensus report and clinical recommendations of group 3 of the XV European Workshop in Periodontology. J Clin Periodontol 21: 183- 194.
-
Gottlow J, Nyman S, Lindhe J, Karring T, Wennström J (1986) New attachment formation in the human periodontium by guided tissue regeneration. Case reports. J Clin Periodontol 13(6): 604-616.
-
Elian N, Cho SC, Froum S, Smith RB, Tarnow DP (2007) A simplified socket classification and repair technique. Pract Proced Aesthet Dent 19(2): 99-104.
-
Lim G, Lin GH, Monje A, Chan HL, Wang HL (2018) Wound Healing Complications Following Guided Bone Regeneration for Ridge Augmentation: A Systematic Review and Meta-Analysis. Int J Oral Maxillofac Implants 33(1): 41-50.
-
Hürzeler MB, Zuhr O, Schupbach P, Rebele SF, Emmanouilidis N, et al. (2010) The socket-shield technique: a proof-of-principle report. J Clin Periodontol 37(9): 855-862.
-
Abdelhamid A, Omran M, Bakhshalian N, Tarnow D, Zadeh HH (2016) An open randomized controlled clinical trial to evaluate ridge preservation and repair using SocketKAP(™) and SocketKAGE(™) : part 2 - three- dimensional alveolar bone volumetric analysis of CBCT imaging. Clin Oral Implants Res 27(6): 631-639.
-
Blaschke C, Schwass DR (2020) The socket-shield technique: a critical literature review. Int J Implant Dent 6(1): 52.
-
Antonious M, Couso-Queiruga E, Barwacz C, González- Martín O, Avila-Ortiz G (2021) Evaluation of a Minimally Invasive Alveolar Ridge Reconstruction Approach in Postextraction Dehiscence Defects: A Case Series. Int J Periodontics Restorative Dent 41(3): 335-345.
-
Avila-Ortiz G, Gubler M, Romero-Bustillos M, Nicholas CL, Zimmerman MB, et al. (2020) Efficacy of Alveolar Ridge Preservation: A Randomized Controlled Trial. J Dent Res 99(4): 402-409.
-
Berglundh T, Lindhe J (1997) Healing around implants placed in bone defects treated with Bio-Oss. An experimental study in the dog. Clin Oral Implants Res 8(2): 117-124.
-
Avila-Ortiz G, Chambrone L, Vignoletti F (2019) Effect of alveolar ridge preservation interventions following tooth extraction: A systematic review and meta-analysis. J Clin Periodontol 21: 195-223.
-
Trimpou G, Weigl P, Krebs M, Parvini P, Nentwig GH (2010) Rationale for esthetic tissue preservation of a fresh extraction socket by an implant treatment concept simulating a tooth replantation. Dent Traumatol 26(1): 105-111.
-
Steigmann M, Cooke J, Wang HL (2007) Use of the natural tooth for soft tissue development: a case series. Int J Periodontics Restorative Dent 27(6): 603-608.
-
Bakshi M, Tarnow D, Bittner N (2018) Changes in Ridge Dimension with Pontics Immediately Placed at Extraction Sites: A Pilot Study. Int J Periodontics Restorative Dent 38(4): 541-547.
-
Edelhoff D, Sorensen JA (2002) Tooth structure removal associated with various preparation designs for anterior teeth. J Prosthet Dent 87(5): 503-509.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells