Pediatric Case of Calcifying Epithelial Odontogenic Tumor-A Case Report
Calcifying epithelial odontogenic tumor (CEOT), also known as Pindborg tumor, is a rare, slowly growing, locally invasive epithelial odontogenic neoplasm. Among all odontogenic tumors, CEOT accounts for only 1% of cases. Although CEOT’s are mostly benign, malignant transformations have also been reported. Hence early diagnosis is important to improve the prognosis and the quality of life of the individual. Here we report a unique case of CEOT in a 12 year old male who presented with chief complaint of swelling in the lower right part of face. Sequential and systematic examination revealed the presence of thin walled solitary expansile lesion with subtle areas of calcification suggestive of CEOT. Proper clinic pathological and radiological correlation is essential in diagnosing this benign neoplasm. Complete surgical excision is essential to prevent its recurrence. Recurrence in the pediatric population is unknown hence close surveillance is of great importance.
Abbreviations
CEOT: Calcifying Epithelial Odontogenic Tumor.
Introduction
Calcifying epithelial odontogenic tumor (CEOT), also known as Pindborg tumor, was described by Danish oral pathologist Jens Pindborg in 1955. This benign odontogenic neoplasm is slow growing and expansile. Among all types of odontogenic tumors, CEOT accounts for only 1% of cases [1]. Primarily intraosseous, the tumor typically occurs in the posterior mandible, with over half of the described cases being associated with tooth impaction and most patients being asymptomatic. An extraosseous variant that is usually noted in the anterior gingiva, has also been reported [2].
A 12 year old male patient reported to the department of Oral Medicine with a chief complaint of swelling in the right lower third of face since 15 days. Swelling was initially pea sized and it rapidly progressed in size with no associated symptoms and with no history of trauma, pain, discharge or fever.
Extra Oral Examination
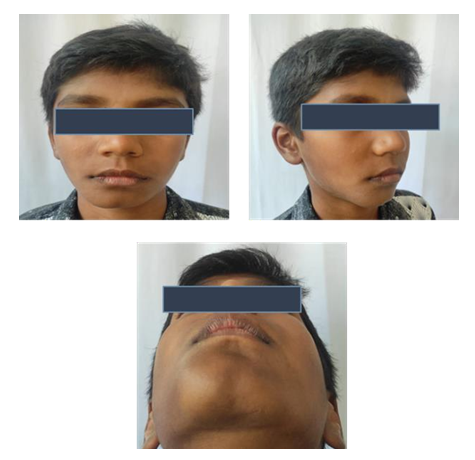
On inspection, diffuse swelling was noted on the right lower third of face of size measuring approximately 3x2 cm extending mediolaterally from midline of chin to imaginary vertical line drawn from outer canthus of right eye. Swelling extends super inferiorly from imaginary horizontal line drawn from corner of mouth to tragus of right ear to 0.5 cm below the inferior border of mandible. Swelling had indistinct edge and skin over swelling appeared normal. On palpation, the swelling was non tender, hard in consistency, non-fluctuant, non-compressible with no local rise in temperature or paraesthesia (Figure 1).
Intra Oral Examination
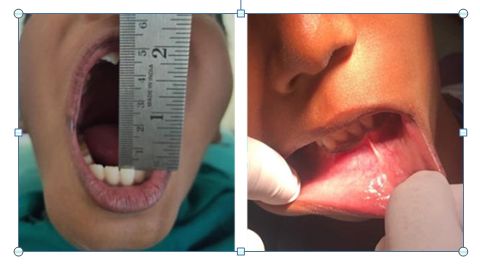
On inspection, Mouth opening was adequate. Swelling was noted of size 2x2 cm extending from 41 to 83 regions. Vestibular obliteration was noted in relation to 42, 83 region. On palpation, the swelling was non tender, hard in consistency.
Buccal cortical expansion was noted anteroposteriorly from 42 to 83 regions. Mild amount of lingual cortical expansion was also noted. Decortication noted in the vestibular region of 83 with the swelling being firm in consistency (Figure 2).
After the clinical examinations, the provisional diagnosis was central ossifying fibroma in the anterior mandible. The differential diagnosis of dentigerous cyst, calcifying epithelial odontogenic tumor and ameloblastoma were also considered. As part of investigations, FNAC was done which revealed the absence of any significant aspirate that signified that the lesion is a tumor.
OPG was done which revealed a well-defined mixed radiopacity and radiolucency of size measuring 3.5x2.5cm in the mandibular region extending anteroposteriorly from root of 31 to 85 regions. Erupting 43 and 44 were embedded in the lesion. Lesion was surrounded by well-defined radiopaque border. Roots of 41 and 42 were pushed distally. Inferior alveolar canal could be appreciated (Figure 3).

The diagnosis obtained after the radiographic investigations was calcifying epithelial odontogenic tumor and a differential diagnosis of adenomatoid odontogenic tumor was also considered.
Finally histopathological studies confirmed the diagnosis of CEOT. Histopathology showed sheets of polyhedral epithelial cells in a fibrous stroma. Prominent intercellular bridges were seen in epithelial island and tumour islands showed masses of calcification. Hyalinised areas resembling amyloid like material is seen amidst epithelial islands (Figures 5-8).
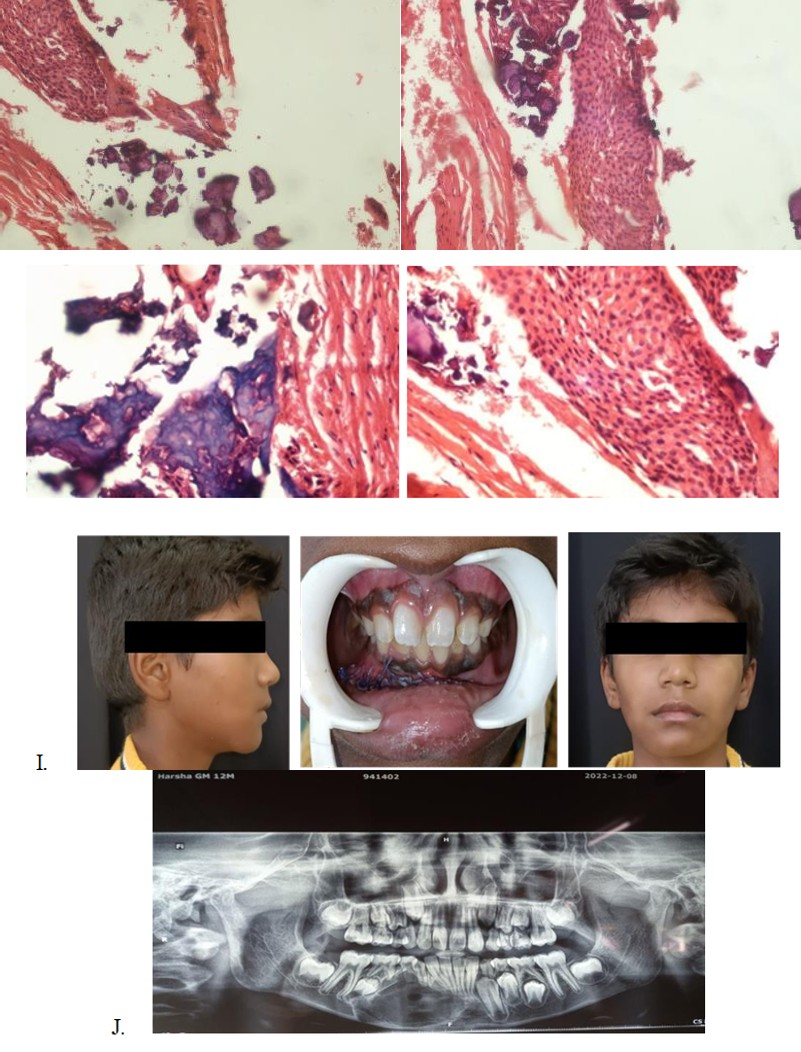
Figures 5,6: Sheets of polyhedral cells with hyperchromatic nucleus and Prominent intercellular bridge
Figures 7 & 8: Basophilic Calcification seen and High Power View.
The treatment done for this case was enucleation of the tumor with curettage along with removal of 43, 44. Also peripheral ostectomy and chemical cauterization with carnoy’s solution was performed (Figures 9 & 10).
Figures 9 & 10: Post op Extraoral, Intraoral and Post op OPG
Discussion
Calcifying epithelial odontogenic tumor (CEOT) is a rare benign neoplasm, which accounts for 1% of all odontogenic tumors. CEOT is usually seen in the posterior area of the mandible affecting 30 to 50 years of age groups without any sex predilection [1]. However the current case was reported in a 12 year old male, which is a rare occurrence in pediatric category.
Guerrisi M, et al. [3] in their 15-year experience with odontogenic tumors in children and adolescents reported 153 pediatric odontogenic tumors, of which only two were CEOT. Both patients were in their second decade of life [3]. Starr BW, et al. [2] had reported a rare case of intraosseous CEOT in a 5 year old patient [2].
Although CEOTs are frequently benign, there are reports about its malignant transformation. The surgical treatment options vary from conservative enucleation and curettage, resection and even hemimandibulectomy or hemimaxillectomy. Maxillary lesion is usually treated with maxillectomy as they grow more rapidly as compared to mandibular lesions [4, 5]. Treatment should be individualized for each lesion because of the variations in the clinical and histologic features.
The CEOT recurrence rate in adults is approximately 15%, and a long-term follow up of 5–10 years is suggested for the adult patients. Franklin and Pindborg reported of 113 CEOT patients treated with enucleation and curettage with 1 year follow up and a recurrence rate of 14–30%, with an average recurrence of 14% [6]. Chrcanovic BR, et al. [7] noted that the highest risk of recurrence was following treatment with excision and curettage. Patients undergoing either marginal resection (0% recurrence) or segmental resection (7.5% recurrence) had lower recurrence rates [7]. Since the CEOT recurrence rate in the pediatric population is unknown, we can only derive a recurrence rate based on the long term adult data.
Conclusion
CEOT is a rare odontogenic tumor which accounts for 1% of all odontogenic tumors. As CEOT is a rare occurence in pediatric patients, proper clinicopathological and radiological correlation is essential in diagnosing this benign neoplasm. Complete surgical excision is essential to prevent its recurrence. Recurrence in the pediatric population is unknown hence close surveillance is of utmost importance.
References
-
Sarkar F, Gayen S, Kundu S, Pal M (2019) Clinical, Radiological and Histological Features of an Unique Case of Calcifying Epithelial Odontogenic Tumor. J Oral Maxillofac Pathol 23(3): 478.
-
Starr BW, Lax EA, Barone AAL, Ulma RM, Pan BS, et al. (2022) Pindborg Tumor in Early Childhood: a Rare Tumor in the Youngest Patient Reported to Date. Case Reports Plast Surg Hand Surg 9(1): 61-65.
-
Guerrisi M, Piloni MJ, Keszler A (2007) Odontogenic Tumors in Children and Adolescents. A 15-year Retrospective Study in Argentina. Med Oral Patol Oral Cir Bucal 12(3): E180-E185.
-
Vigneswaran T, Naveena R (2015) Treatment of Calcifying Epithelial Odontogenic Tumor/Pindborg Tumor by a Conservative Surgical Method. J Pharm Bioallied Sci 7(Suppl 1): S291-S295.
-
Misra SR, Lenka S, Sahoo SR, Mishra S (2013) Giant Pindborg Tumor (Calcifying Epithelial Odontogenic Tumor): an unusual Case Report with Radiologic- Pathologic Correlation. J Clin Imaging Sci 3(Suppl 1): 11.
-
Franklin CD, Pindborg JJ (1976) The Calcifying Epithelial Odontogenic Tumor. A Review and Analysis of 113 Cases. Oral Surg Oral Med Oral Pathol 42(6): 753-765.
-
Chrcanovic BR, Gomez RS (2017) Calcifying Epithelial Odontogenic Tumor: An Updated Analysis of 339 Cases Reported in the Literature. J Craniomaxillofac Surg 45(8): 1117-1123.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells