Early Origins of Functional Jaw Orthopaedics
The purpose of the research was to highlight early orthodontic appliances described in the literature and illustrate how they evolved over time to produce the functional orthopaedic appliances currently in use. Functional appliances derive their motive force from the masticatory muscles rather than active components such as screws and springs. The main findings showed that there were two essential components Firs upper arch expansion and alignment, Second anteroposterior skeletal correction. The article also demonstrates how extraction and alignment treatment diverged from non-extraction functional jaw orthopaedics. This subject has not previously been dealt with from this point of view.
Introduction
The purpose of the study was to show how the present generation of functional orthopaedic appliances have been influenced by the designs of the past. The author has completed an exhaustive survey of the literature to demonstrate this from Hunter J [1] to the present date. It is significant that the later designs of appliance have become more efficient at meeting their clinical objectives.
The Inclined Plane Appliance
Inclined plane appliances were amongst the earliest known. A continuous evolution can be traced from the time of Hunter J [1] described a silver splint in the lower arch to correct anterior crossbite. “The best of these means is an instrument of silver, with a socket or groove shaped to the fore teeth of the lower jaw to receive them, so as to become fast to them, and sloped off as it rises to its upper edge, so as to rise behind the fore teeth in the upper jaw in such a Conceptual Paper manner, that, upon shutting the mouth, the teeth of the upper jaw may catch the anterior part of the slanting surface, and be pushed forward with the power of the inclined plane. The patient, who wears such an instrument, must frequently shut his mouth with this view.” This was a truly myofunctional appliance harnessing muscle force to align the teeth. No illustration was provided to show its precise design.
Sigmond J [2] refers to the use of gold plates or shields to correct irregularities of the teeth, but no clinical detail is given in what was intended as a domestic manual for the use of patients. Impressions of both jaws were taken and models cast. Daily and frequent inspection was necessary to regulate or alter the gold plate.
Catalan LJ [3] developed the inclined plane to push lingually positioned maxillary teeth forwards over the bite. Philippe J [4] did this but it was not until 1826 that it was published as a pamphlet entitled “The device suitable for correcting the deformity that involves the lower jaw overlapping in front of the top jaw.” Imrie W [5] describes a technique where a wax impression was taken, modeled to an inclined plane resembling a wedge and then embedded in plaster, leaving a small opening at the top. The wax was boiled out and the mould filled with molten tin. On removal of the plaster mould the tin block corresponded precisely to the wax impression and was fitted to the lower teeth where it was self-retaining.
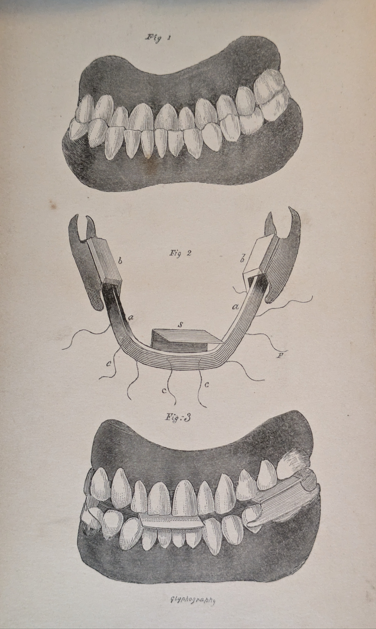
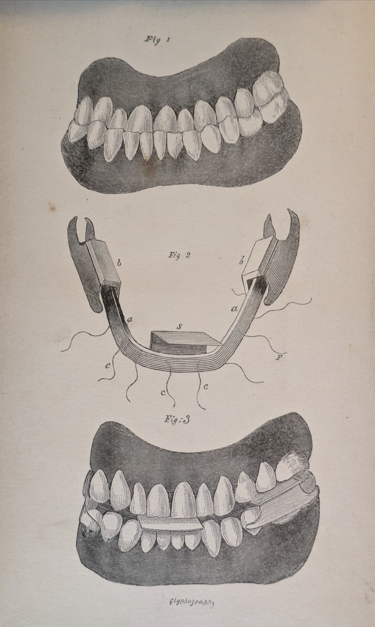
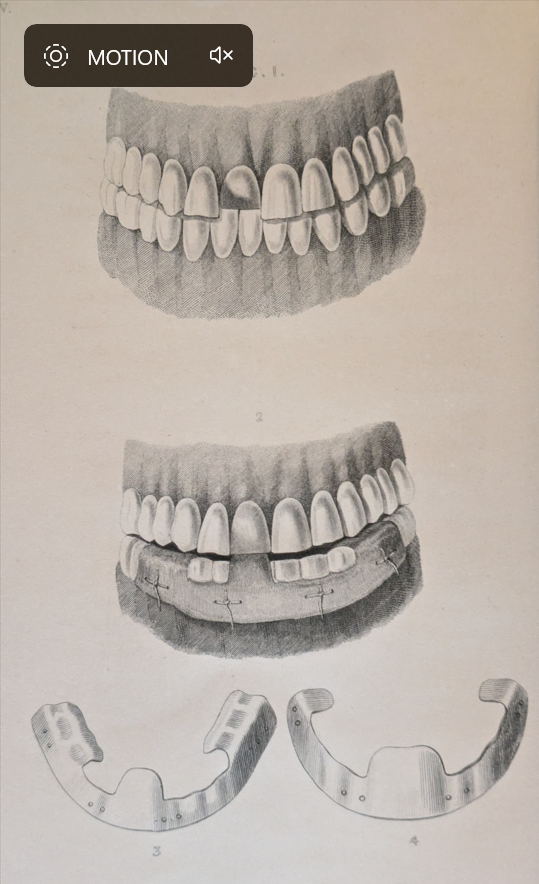
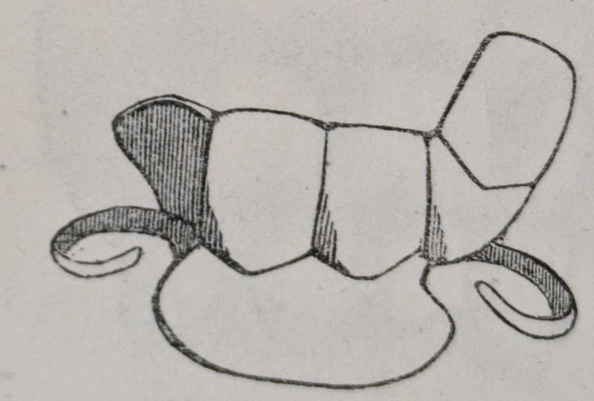
Delabarre CF [6, 7] Figure 1 on the illustration and Schange JMA [8] Figure 2 on the illustration describe and illustrate Catalan’s appliance before going on to develop their own modifications of his design. Both authors independently show the same illustration. A flat arch bar is fitted to the labial surfaces of the lower arch with extension plate’s lingual to the upper incisors to move them forwards as necessary and rests on the most distal molar for stability.
Delabarre mentions that “M Duval (1758-1854) speaks of a guttered plate, that has been in use for 20 years but he has not given us any description or design of it.” According to Delabarre it was probably a small inclined die placed on the deviated tooth. Catalan invented an instrument based on the same principles [6, 7, 8]. Delabarre considered Catalan’s design to be too traumatic and illustrated one of his own Figure 1. “In the application of a small metallic grate fashioned in the form of two inferior molars of one side; which, by preventing the closing of the mouth, suspends the contact of the teeth.” “With a fillet of silk or thread, I bind the teeth in such a way; that in a very short time, I succeed in leading the deviated tooth or teeth within the circle, of which they should form a part.” Thus Delabarre was using a lighter externally applied force rather than one generated by the masticatory muscles via the occlusion. This was the same principle as used by Fox J [9] and Bell T [10].
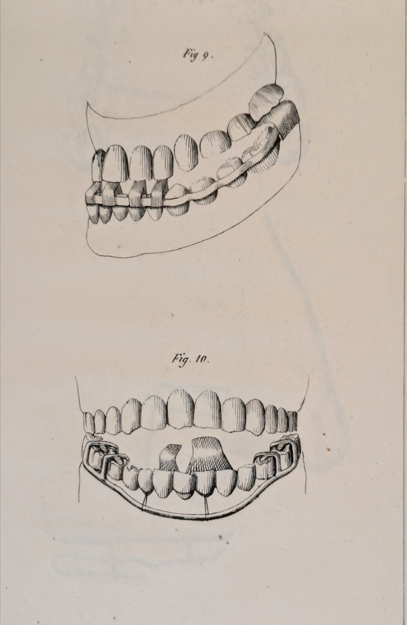
Schange JMA [8] published the first book entirely devoted to orthodontics in 1842. He emphasized that his design was neither that of Catalan nor that of Delabarre. Figure 2 (Figure 10 on the illustration) He had a lower labial arch bar that was away from the teeth to allow them to be drawn forwards with ligatures. At the same time he had molar rests for stability and retention. In addition he had a lingual arch bar from which plates extended lingual to the upper incisors to move them forwards using the inclined plane effect. Thus he utilized both masticatory muscle function and applied traction by ligatures.
Robertson W [11] believed that anterior crossbite resulted in protrusion of the lower face. “In order to rectify this deformity, a plate is adapted to the lower range of teeth, and so constructed as to produce pressure upon the irregular ones by which contrivance the rest of the teeth are prevented from coming in contact with each other, and the whole pressure of the mouth shutting is thrown upon the irregular teeth, which act against the inclined surface of the plate, and by degrees are moved forwards into their proper situations” (Figure 3).
Mortimer WH [12] described “a gold band to go inside all the under teeth and joined to a plate that will cover the large grinders on each side” (Figure 4). “In the centre, an inclined gold plane should come over the under teeth, so that every time the mouth closes, the upper teeth may strike against it, and be pushed outwards.”
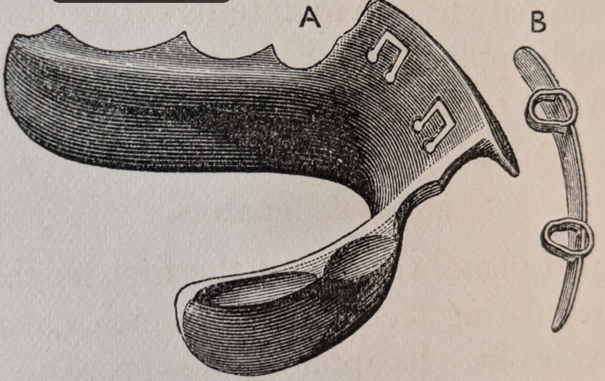
Robinson J [13] used a gold plate accurately fitted to the lower teeth. To the upper margin a gold flange was soldered, (Figure 5). “Every closure of the mouth must exert a constant and steady pressure upon the irregular teeth, until the deformity is counteracted by bringing them over those in the lower jaw.”
Salter SJA [14] states that “a very powerful method of bringing forward upper teeth in an underhung bite is by placing upon the lower incisor teeth a plate from the upper edge of which a process passes obliquely upwards and backwards, so that when the patient closes his mouth the upper teeth rest on the sloping surface and are pushed forwards” (Figure 6).
Norman Kingsley and the Sloping Anterior Bite Plane
Kingsley NW [15] “A treatise on oral deformities as a branch of mechanical surgery.” Although it was 541 pages in length only 3 ½ pages were devoted to the subject of bite planes.
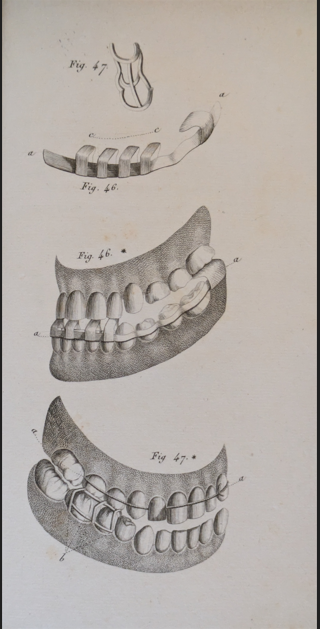
First the lower inclined bite plane was described and illustrated (Figure 7) (on the illustration). This was constructed in vulcanite and fitted in the lower arch. It impinged on any retroclined upper teeth to move those forwards over the bite in the traditional way described by previous workers. “The inclined plane was one of the first mechanical forces adopted for regulating teeth, and was much recommended in earlier text-books.”
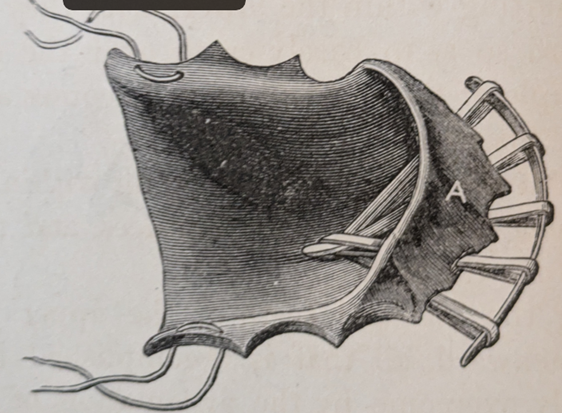
Kingsley’s genius was to flip the lower inclined bite plane upside down to the upper arch and change its function. The appliance consisted of a vulcanite base plate tied in situ with molar ligatures (Figure 8) (on the illustration). There was an anterior bite plane with a steep forward facing slope which caused the mandible to posture forwards. In addition, a gold bar was placed labially to the upper incisors. Elastic ligatures ran over the gold bar and then through the holes in the vulcanite base plate to a gold hook on the palate. When activated they helped to reduce the incisor prominence.
He was the first person to introduce the concept of functional orthopaedics to correct a Class II malocclusion by “jumping the bite.” “The object was not to protrude the lower teeth, but to change or jump the bite in the case of an excessively retreating lower jaw.” “The objection urged against the use of an incline, because the time required had a tendency to alter the articulation of the teeth, was in this case an argument in its favour, and an advantage, because a new articulation was desired and the incline, as adapted, offered no opposition to the antagonism of the teeth.” “The principle of the inclined plane is always operating in the mouth, and may often be taken advantage of beneficially, while at other times it will tax our ingenuity to the utmost to overcome its powerful influence.”
The Extraction Versus Non-Extraction Approach to Class II Division 1 Treatment
Chupein TF [16] is one of the earliest references to the extraction of maxillary first premolar teeth for the treatment of Class II division 1 malocclusion although the first person to propose this may well be lost in the mists of time. This landmark paper was published in Catching’s Compendium
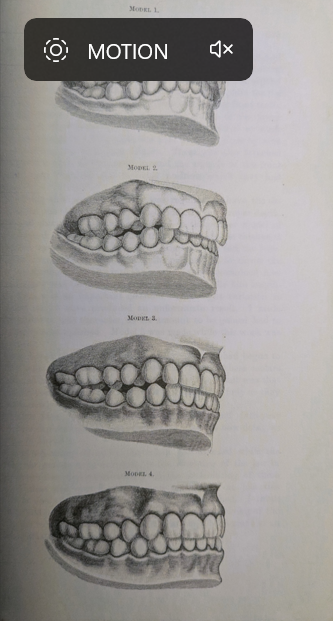
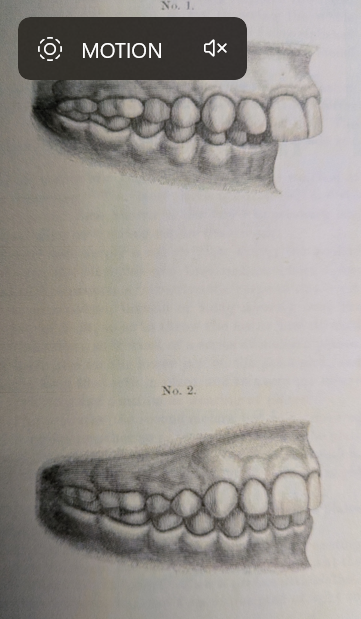
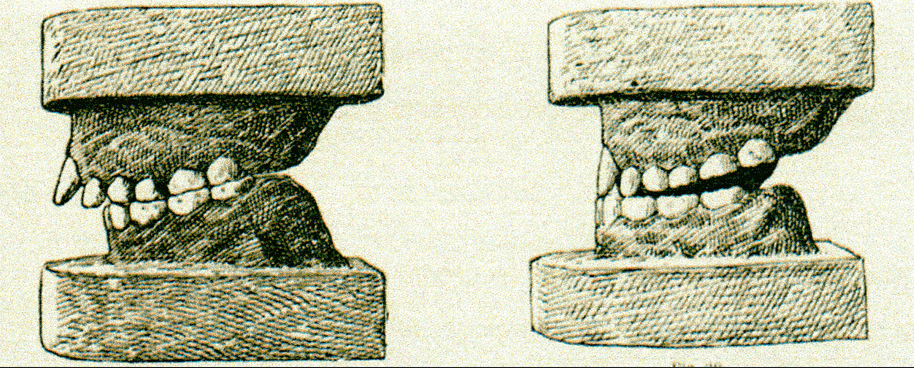
of Practical Dentistry entitled “Protrusion of upper teeth regulated.” He used a gold cap cemented onto the upper central incisors with two small distal hooks. German silver bands with buccal hooks were cemented on the upper first molars. Elastic bands were stretched from the hooks on the central incisor cap to the molar bands on both sides after extraction of the upper first premolars (Figures 9-11). Etchings of before and after models together with a profile view of the patient show a successful result.

Figure 9(A): Chupein TF profile view before treatment.
Figure 9(B): Chupein TF profile view after treatment.
Figures 11(A): Chupein TF dental models before treatment.
Figures 11(B): Chupein TF dental models after treatment.
Cutter HE [17] published an article entitled “Drawing the lower jaw forward” in the same volume of Catching’s Compendium. This article had no illustrations but a similar paper was read before the American Academy of Dental Science with illustrations [18] (Figure 12). This involved first upper arch expansion with a jack screw and vulcanite plate. This was followed by an early design of functional appliance. One was thickened in the molar and premolar regions with depressions to carry the mandible forwards on occlusion. This was followed with an appliance thickened behind the upper incisors to maintain the forward mandibular posture.
Hamilton originally described the functional appliances used by Cutter in the American Academy of Dental Science January 1892 [19] and Catchings Compendium June 1892 [20] (Figure 13). An uncrowded Class II division 1 case without pre-functional expansion was described. “The method used was simply a rubber plate fitting the roof of the mouth and over the bicuspids and first molars, where it was made thick and with depressions to receive the cusps of the lower teeth. But these depressions, instead of being directly over the cusps, were slightly in front, so as to throw the lower jaw forward when closed, by the action, as it were, of a series of inclined planes.” The upper plate was alternated with a lower one of similar design and the treatment was completed in four months. Hamilton speculated on the mechanism of action. “This advance of the lower jaw comes, I think, from preventing the condyle going to its place; but there is a change going on at the angle of the jaw which will ultimately allow a perfect articulation.” No illustration of the appliance itself was given.
Coffin, Headridge and the Origins of Upper Arch Expansion
Coffin CR around 1860 inserted a rigid vulcanite plate with Hickory wood sticks embedded to correct imbricated incisors. When exposed to saliva the wood expanded to apply a force. The incisors resisted successive increments of force with little progress. However, a sudden correction was achieved when the plate accidently fractured in the midline and the incisors spread due to the inadvertent expansion. The Coffin plate was made of vulcanite, split into two halves capping over the buccal segments and joined with a W – shaped spring formed from piano wire (Figure 14). Details of the design and construction of this appliance are given by Trenouth MJ [21]. It was not until 1881 that the technique was reported by his son Coffin WH [22] at the 7th International Medical Congress in 1881.
However this publication stimulated correspondence in the journals, first from Headridge P [23, 24] of 1, Lime Grove, Oxford Road, Manchester. To quote: “I must confess I was simply stupefied to find that the author of the paper claims unblushingly the invention of the expansion plate for his father, and all through the paper and subsequent discussion the plate is spoken of as Dr. Coffins Expansion Plate. Now I simply wish to state that Dr. Coffin has just as much to do with the invention of that plate as the man in the moon and no more. The invention in its entirety is wholly and absolutely mine, which I can abundantly prove, and in common justice it should be known , both now and here after, not as Dr Coffin’s but as Peter Headridge’s Expansion Plate, a claim supported by Williams J [25, 26] of Hollinwood House, Fallowfield, Manchester.” Details of the succeeding correspondence are given in detail by Trenouth MJ [21].
In response Coffin WH wrote [27, 28] “My father in common with others used expansion plates before Mr. Headridge entered the profession; that gentleman, however, (for many years my father’s assistant) about 1868, suggesting the employment of tempered steel springs in connection with them.” In 1869, Headridge took out a patient for: “Improvements in Dentistry for Expanding the Upper and Lower Maxillary, claiming, broadly, as new and never before used, first, dividing the base or plates into sections: second, giving these elasticity &c, by springs or other elastic substances. The patient was dated 10 April, No 1101 and was procurable for sixpence.
The final letter and therefore say in the controversy was submitted by Coffin WH himself [29]. It was prefaced by the editorial comment that “we do not hold ourselves responsible for the opinions expressed by our correspondents” and ended by the statement that “we cannot insert any more letters on this subject.-Ed.” To quote: “Sir, - I observe with pain and regret that my old friend Mr. Headridge of Manchester, is led by his extraordinary misconception of the origin of expansion plates into some remarkable and utterly unfounded statements, which prefer a serious charge of dishonesty, unfairness and inaccuracy against myself and son.”
Jackson’s Modification of the Coffin Appliance
Jackson VH [30] modified the Coffin appliance in two ways. First he eliminated the molar bite blocks and used clasps on the molars and premolars to reduce the bulk of the appliance. Secondly he inverted the spring from a W to an M-shape, reducing the number of loops from 5 to 3. He also thickened the diameter of the wire from 0.86 mm to 1.1mm (Figure 15). This became the predominant design for future appliances. In particular it was incorporated into the early Andresen appliance and is still used today in the modern Bionator.
Pierre Robin and the Monoblock
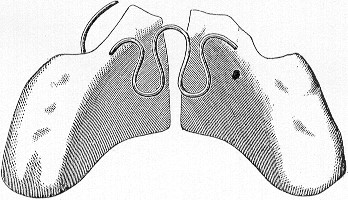
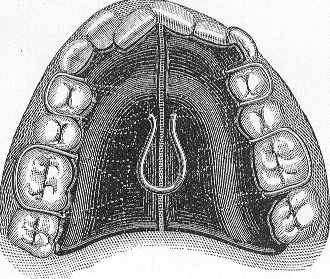
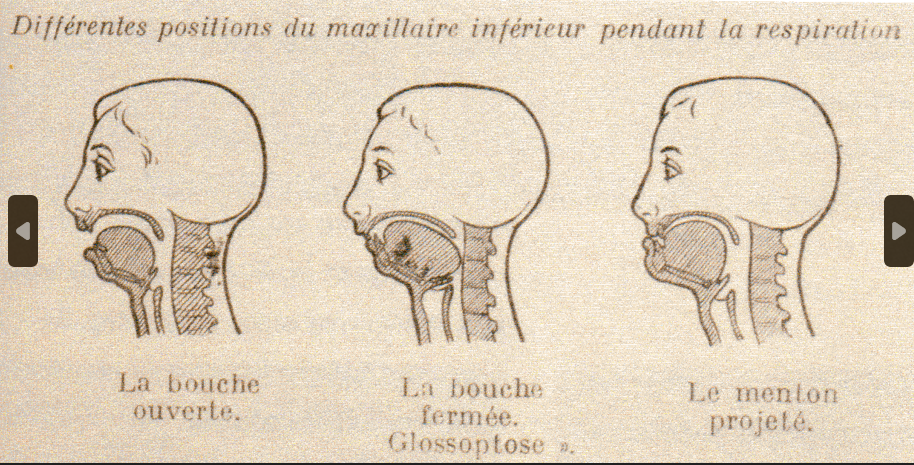
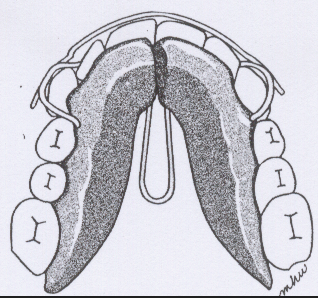
Robin P [31] first trained as a pharmacist then a dentist and finally became a Doctor of Medicine. He served as a maxilla-facial surgeon in the First World War He described a condition he named “glossoptosis” which involved backward movement of the tongue and mandible caused by narrowing of the maxilla (Figure 16). This led to enlarged adenoids, mouth breathing, airway obstruction, and being backward at school. The article by Robin P [32] which is often quoted is in fact two separate papers published in the same volume of the journal. The first [32] described maxillary expansion using an upper removable vulcanite plate with an midline expansion screw (Figure 17). The second [33] describes the monoblock to correct Class II jaw relationships (Figure 18). The monoblock could not be worn for eating so it was worn in conjunction with the mastication appliance which prevented the mandible from moving backwards when eating (Figure 19). The long term effect was to treat mandibular hypoplasia and glossoptosis by enlarging the airway.
The Early Andresen Appliance
Andresen V [34] developed his appliance initially as a retention device but later found it would work as an active functional orthopedic mechanism. He extended the sloping anterior bite plane of Kingsley into the molar regions and split the base plate, incorporating a “Coffin spring” after Jackson’s design (Figure 20). Andresen practiced in Norway but originally came from Denmark. Fixed appliances tended to be removed during the Summer holiday period in Norway as people went away for long periods to make the most of the good weather. For this reason the Andresen appliance was used as a retainer. In Class II cases some activation was put in to prevent relapse. It was soon discovered that the Andresen appliance acted as an active mode of Class II correction and was later modified to produce the “activator” as discussed by Andresen V, et al. [35].
Later Developments
All later functional appliance systems were variations of the Andresen appliance which have gradually evolved largely by a process of trial and error. This resulted in many variations in design, most of which bear the names of their originators; most notable amongst these are Schwarz AM [36], Bimler HP [37], Herren P [38], Muller GH [39], Stockfisch H [40], Frankel R [41], Balters W [42], Harvold EP [43]. A very comprehensive account of these and many other developments is given in the book “The masters of functional orthodontics” by Levrini A, et al. [44]. Two more recent advances have been the biobloc appliance of Mew J [45, 46, 47] and the twin-block technique of Clark WJ [48, 49]. Trenouth MJ [50] combined elements of these two techniques. First, semi-rapid maxillary expansion after Mew JCR [51] and alignment of the upper arch. Second, correction of the Class II relationships using a modification of the Twin block traction technique introduced by Clark WJ [48, 49]. who used a 45 degree block incline and relied on extra oral traction and intermaxillary elastics from the Concord facebow to produce mechanical forward posturing. A 70 degree incline on the blocks maintains the mandible in a forward position even when open in the rest position and induces an artificial forwards bite of accommodation, as a result of forwards reflex posturing. This meant the extra oral traction and intermaxillary elastics on the original Clark appliance could be dispenced with because they were no longer necessary for the appliance to function efficiently. This was initially reported in a paper read at the Consultants Orthodontists in February 1985. The concept of forward reflex posturing using 70 degree block incline was published in 1989 [50] a year after Clarks second paper describing a 45 degree incline however my 1989 paper was received for publication in May 1987 one year before Clark’s second 45 degree incline paper which is often misquoted as recommending a 70 degree incline [52, 53]. This approach has recently been evaluated by a prospective randomized clinical trial [54]. It was found that the presence of a Southend clasp on the upper and lower incisors limited their tipping which enhanced the skeletal correction. Further analysis of the trial data showed expansion of the oropharyngeal airway [55, 56] in a similar way to Robin’s monoblock.
Discussion and Conclusion
The origin of functional appliance treatment goes back a long way in time with elements of many simpler designs being incorporated in later appliances. Two important facts have been realized recently with lots of published evidence to support them. First that functional orthopaedics results in significant correction of skeletal malocclusion. Second following on from the skeletal correction is the expansion of airway volume. This harks back to the work pf Pierre Robin P [31, 32, 33]. This fact is clearly important in reducing the likelyhood of sleep apnoea.
References
-
Hunter J (1778) A Practical Treatise on the Diseases of the Teeth. In: Johnson J (Edn.), London pp: 84-86.
-
Sigmond J (1825) A Practical and Domestic Treatise of the Diseases and Irregularities of the Teeth and Gums: with Methods of Treatment. Bath: Wood & Cunningham pp: 120-122.
-
Catalan LJ (1836) The Device Duitable for Correcting the Deformity that Involves the Lower Jaw Overlapping in Front of the Top. USA.
-
Philippe J (2005) The Origin of Orthodontics. Two Centuries of Orthodontics around the Atlantic Paris: Bresson pp: 1-16.
-
Imrie W (1834) The Parents Dental Guide. A Treatise on the Diseases of the Teeth and Gums from Infancy to Old Age. In: Churchill J (Edn.), London pp: 48-49.
-
Delabarre CF (1819) Traite de la Second Dentition et Method Naturelle de la Diriger. Suives d’un apercu de Semeiotique buccale. USA.
-
Delabarre CF (1845) A Treatise on Second Dentition and the Natural Method of Directing it-Followed by a Summary of Stomatic Semeology. In: Harris CA (Edn.), Baltimore: J W Woods.
-
Schange JMA (1842) Precis le redressement des dents, ou expose des motens rationels de prevenir et de corriger led deviations des dents; suivi de quelques reflexions sur le obturateurs du palais. USA.
-
Fox J (1803) The Natural History of the Human Teeth, Including a Particular Elucidation of the Changes Which take Place during the Second Dentition, and Describing the Proper Mode of Treatment to Prevent Irregularities of the Teeth, to Which is Added an Account of the Diseases Which Affect Children during the First Dentition. London 1(12).
-
Bell T (1835) The Anatomy, Physiology and Diseases of the Teeth. Well come Collections pp: 85-103.
-
Robertson W (1835) A Practical Treatise on the Diseases of the Teeth in which the Origin and Nature of Decay are Explained and the Means of Prevention Pointed Out. 2nd (Edn.), London pp: 90.
-
Mortimer WH (1849) Observations on the Growth and Irregularities of Children’s Teeth. In: Higley S (Eds.), 2nd (Edn.), London pp: 67-69.
-
Robinson J (1846) The Surgical, Mechanical and Medical Treatment of the Teeth: Including Dental Mechanics. 2nd (Edn.), London, W Webster pp: 51.
-
Salter SJA (1874) Dental Pathology and Surgery. In: Longmans, et al. (Eds.), London pp: 46.
-
Kingsley NW (1880) A Treatise on Oral Deformities as a Branch of Mechanical Surgery. In: Appleton D, et al. (Eds.), USA.
-
Chupein TF (1895) Protrusion of the Upper Teeth Regulated. In: Byrd CP (Eds.), Catchings Compendium of Practical Dentistry for 1894. Atlanta pp: 185-188.
-
Cutter HE (1895) Drawing the Lower Jaw Forward. In: Byrd CP (Eds.), Catchings Compendium of Practical Dentistry for 1894. Atlanta pp: 167-169.
-
Cutter HE (1894) A Case of Drawing the Lower Jaw Forward. Int Dent J (Phila) 15(6): 353-355.
-
Hamilton HF (1892) Description of a Case of Regulating. Int Dent J (Phila) 13(6): 416-417.
-
Hamilton HF (1892) Throwing the lower jaw forward. Catchings Compendium of practical dentistry for 1892. C P Byrd, Atlanta pp: 180-181.
-
Trenouth MJ (2009) The Coffin Plate and Spring. Dent Hist 50: 90-101.
-
Coffin WH (1881) A Generalised Treatment of Irregularities. Trans 7th Int Med Congress 3: 542-547.
-
Headridge P (1882) Correspondance. Dent Rec 2: 91.
-
Headridge P (1882) Correspondance. Br J Dent Sci 25: 45-46.
-
Williams J (1882) The expansion plate. Dent Rec 2: 186- 187.
-
Williams J (1882) Correspondance. Br J Dent Sci 25: 102.
-
Coffin WH (1882) Correspondance, The expansion plate. Dent Rec 2: 141.
-
Coffin WH (1882) Correspondance, The expansion plate. Br J Dent Sci 25: 46-47.
-
Coffin WH (1882) Correspondance, The expansion plate. Br J Dent Sci 25: 254-255.
-
Jackson VH (1904) Orthodontia and Orthopaedia of the Face. JB Lippincott Company, Philadelphia and London.
-
Robin P (1934) Glossoptosis due to Atresia and Hypotrophy of Mandible. Am J Dis Child 48: 541-547.
-
Robin P (1902) Observation on a New Straightening Device. Rev Stomat 9: 423-432.
-
Robin P (1902) Practical Demonstration on the Construction and Installation of New Recovery Equipment. Rev Stomat 9: 561-590.
-
Andresen V (1936) On the so-called “Norwegan system” of functional jaw orthopaedics. Dtsch Zahnarztl Wschr 39: 283-286.
-
Andresen V, Haupl K (1936) Functional orthodontics. Hermann Meusser, Berlin.
-
Schwarz AM (1938) Teeth control with plates. Ueban & Schwarzenberg, Wien.
-
Bimler HP (1949) The elastic denture former. Zahnarztliche Welt 19: 499-503.
-
Herren P (1959) The activators mode of action. Am J Orthod 45: 512-527.
-
Muller GH (1962) The double plate with maxillary spur guide. Advances in orthodontics 23: 243-250.
-
Stockfisch H (1966) The Kinetor in Orthodontics. The Practice of the Polyvalent Bimaxillary Apparatus and its Rational Technology in Plastic Prefabricated Parts. Heidelberg, Huthig Verlag.
-
Frankel R (1969) The treatment of Class II division 1 malocclusion with functional correctors. Am J Orthod 55(3): 265-283.
-
Balters W (1973) An introduction to the Bionator healing method, selected writings and lectures. Heidelberg.
-
Harvold EP (1974) The activator in interceptive orthodontics. CV Mosby Co, St Louis.
-
Levrini A, Favero L (2003) The masters of functional orthodontics. Quintessence Verlag, Berlin.
-
Mew J (1979) Bioblock therapy. Am J Orthod 76(1): 29- 50.
-
Mew JR (1986) Factors influencing mandibular growth. Angle Orthod 56(1): 31-48.
-
Mew JCR (2004) The postural basis of malocclusion: a philosophical over-view. Am J Orthod Dentofacial Orthop 126(6): 729-738.
-
Clark WJ (1982) The twin block traction technique. Eur J Orthod 4(2): 129-138.
-
Clark WJ (1998) The twin block technique: A functional orthopedic appliance system. Am J Orthod Dentofacial Orthop 93(1): 1-18.
-
Trenouth MJ (1989) A functional appliance system for the correction of Class II relationships. Br J Orthod 16(3): 169-176.
-
Mew JCR (1977) Semi-rapid maxillary expansion. Br Dent J 143(9): 301-306.
-
Trenouth MJ (2000) Twin-block appliance therapy: design and mode of action. Cranio 9: 31-38.
-
Trenouth MJ (2017) Rationale behind twin-block incline. Am J Orthod Dentofacial Orthop 151(2): 232.
-
Trenouth MJ, Desmond S (2012) A randomized clinical trial of two alternative designs of Twin-block appliance. J Orthod 39(1): 17-24.
-
Trenouth MJ, Desmond SR (2016) A cephalometric evaluation of oropharyngeal airway changes during Twin-block appliance treatment. Int J Dent Oral Sci 2(2): 22-30.
-
Trenouth MJ (2019) Airway, Pierre Robin and functional jaw orthopedics. Cranio 10: 12-18.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells