A Possible Link between Non-Nutritive Sucking Habits and Herniated Dental Follicles: A Case Series
Background: Herniated dental follicle (HeDF) is an uncommon and poorly recognized gingival lesion, often misdiagnosed due to its subtle clinical presentation. Case Presentation: This case series presents two unique cases of HeDF in pediatric patients with possible contributing factors associated with a sustained oral habit. The first case involves a five-year-old male with an asymptomatic pink, raised, sessile, finger-like projection on the alveolar mucosa of the right maxillary molar region. The second case had similar clinical findings in a seven-year-old female overlying unerupted maxillary left lateral incisor. Both cases had a positive finding of nonnutritive sucking habit and were treated conservatively with restoration of normal anatomy after tooth eruption within six to eight months. Clinical Implication: This case series highlight the importance of recognizing HeDF for conservative management to prevent unnecessary surgical intervention and to explore whether a non-nutritive sucking habit could be an etiologic factor for HeDF.
Abbreviations
HeDF: Herniated Dental Follicle.
Introduction
Herniation of dental follicle is a rarely reported pathologic finding in children [1, 2, 3, 4]. Based on a previous report we defined herniated dental follicle (HeDF) as a localized, asymptomatic, papule or nodule extruded through the alveolar mucosa associated with an unerupted tooth [2]. After the first report by Geneser MK, et al. [2] there have not been any other reported cases of HeDF in the literature [2]. HeDF is speculated to be the result of disruptions in normal tooth eruption processes [5].
The dental follicle is located around the developing tooth germ and plays a crucial role in tooth eruption [5]. Dental
follicle is an ectomesenchymal structure that surrounds the developing tooth and orchestrates tooth eruption by spatio- temporal signaling for bone resorption and deposition to create an eruption pathway [6]. However, impaired signalling [7], trauma [8], physical barriers [8], anatomical limitations [9], age [10], nutritional deficiencies [10], genetic mutations [7], hormonal imbalances [11] or metabolic syndrome [11] can lead to impaired tooth development or eruption [12].
The etiologies of HeDF includes trauma of the alveolar mucosa, abnormal tooth development, or changes in pressure within the follicular sac [2]. Any or all of these factors result in a disruption of the mucosal surface, thus creating an opening for part of the follicle to be expressed out into the oral cavity. Clinically, HeDF presents as a soft-tissue papule or nodule with a sessile or pedunculated base. The surface is smooth and glistening in the early stages, but may become ulcerated with pseudomembranous surface. The lesion ranges in color from pink to red to yellowish-white. The surrounding alveolar mucosa is usually normal appearing, but may exhibit mild edema associated with tooth eruption [2]. Radiographically, HeDF is associated with normally developing crown of an erupting tooth [2]. HeDF is often asymptomatic, so the diagnosis may be delayed with underestimated prevalence.
Histopathologically, the follicle consists of fibromyxomatous connective tissue with areas of necrosis, granulation tissue, and acute or chronic inflammatory cells [2]. Variable amount of reduced enamel epithelium may be present while the underlying connective tissue may have bacterial colonization [2]. The differential diagnosis of HeDF includes eruption cyst [9], eruption sequestrum [13], parulis [2], and pyogenic granuloma [14]. Table 1 provides detailed information of all differential diagnoses along with HeDF.
Surgical intervention is seldom necessary as monitoring or conservative local curettage is often sufficient for resolving the condition without complications [2]. Understanding this entity and distinguishing it from other gingival lesions is important for developing differential diagnoses and providing appropriate treatment. This case series discusses two pediatric cases with HeDF along with clinical-radiographic findings and previously unreported contributing factors.
Case Description
The case series presents anonymized clinical information from two patients reported to the dental clinic at Children’s Hospital Colorado.
| Lesion | Site | Clinical findings | Radiographic findings | Histopathologic findings | Management | Predilection | Associated tooth/teeth | |
|---|---|---|---|---|---|---|---|---|
| Eruption Sequestrum | Alveolar ridge | Mineralized, rough fragment overlying the crown of erupting permanent molar after emergence of cuspal tips. | Thin, linear opacity overlying occlusal surface of unerupted molar | Fragment of osteodentin with acute inflammatory cells and necrosis around periphery | Conservative management and in rare cases surgical removal of mineralized fragment | Unknown | Mandibular first permanent molar | |
| Eruption Cysts | Alveolar ridge | Bluish gingival swelling overlying an unerupted primary or permanent tooth | Normal to enlarged pericoronal radiolucency that extends to the overlying alveolar mucosa | Thin squamous-lined cyst with variably dense inflammatory infiltrate and erythrocytes | No treatment to unroofing of the overlying alveolar mucosa and curettage to facilitate eruption | Males | Any tooth but most commonly the primary incisors and permanent first molar | |
| Pyogenic Granuloma | Any oral mucosal site but most common on gingiva | Red friable soft tissue nodule that bleeds freely; may be creamy white when ulcerated | Radiographs may identify local contributing factors such as calculus, dental caries, or restoration | Lobules of vascular granulation tissue with numerous congested blood vessels and a mixed inflammatory infiltrate; surface epithelium is usually ulcerated. | Surgical excision and removal of local contributing factors | Females | Any tooth but especially anterior teeth in children | |
| Parulis | Labial or buccal gingiva | Red or yellowish-white papule or nodule with a purulent discharge from sinus tract; usually tender | Periapical or interradicular radiolucency associated with a nonvital tooth that exhibits widening of periodontal ligament space, loss of lamina dura and often root resorption | Acutely inflamed granulation tissue with necrotic debris, bacteria and usually a sinus tract | Treatment of the associated tooth and local curettage of the infected gingival tissues | Unknown | Variable (non-vital tooth) | |
| Herniated dental follicle | Alveolar ridge mucosa | Finger-like projection or papule on alveolar ridge overlying unerupted tooth | Normally erupting tooth | Thin fragment of inflamed follicle with focal necrosis and remnants of reduced enamel epithelium with or without bacterial colonization. | No treatment to simple soft tissue curettage. In rare cases, surgical excision to prevent further trauma or secondary infection | Unknown | Primary and permanent incisors and molars |
Table 1: Reported Findings in Herniated Dental Follicle and Differential Diagnoses. Case 1 Five-year-old male patient that report
Table 1: Reported Findings in Herniated Dental Follicle and Differential Diagnoses. Case 1 Five-year-old male patient that reported to the dental clinic for routine care with a chief complaint of a raised lesion on the upper right side of the mouth for one week. Patient was healthy with no known allergies. The patient’s height was on 50th percentile, weight was 30th percentile while BMI was 20th percentile based on medical growth charts. The only significant dental history was the continuous and prolonged use of a pacifier.
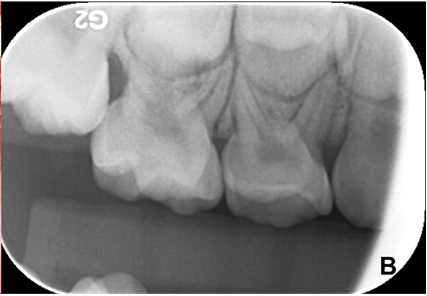
Figure 1A: Clinical presentation of a papule with a smooth, pink, sessile lesion (2 mm diameter, 4 mm height) on the alveolar mucosa overlying the unerupted upper, right, first permanent molar. Figure 1B: Periapical radiograph showed upper, right, first permanent molar close to eruption with only thin layer of overlying alveolar mucosa.
Case 2
Seven-year-old female patient reported to the dental clinic for routine care with a chief complaint of bump on the gingiva in the maxillary, left, anterior region that developed ten days ago. Patient was healthy with the exception of environmental allergies. Based on the growth charts, patient’s height was 75th percentile, weight was 58th percentile, while the BMI was 37th percentile. Dental history was significant for non-nutritive digit sucking habit (5 hours/day).
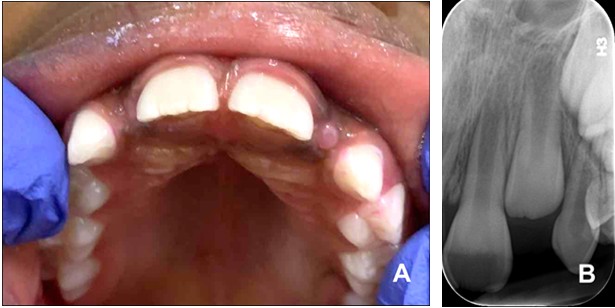
Figure 2A: Clinical presentation of a smooth, pink, sessile papule (3 mm in diameter, 1.5 mm in height) on the alveolar mucosa overlying the unerupted upper, left, permanent lateral incisor.
Discussion
Dental follicle is a loose connective tissue sac surrounding the enamel organ of the developing tooth that originates from the cranial neural crest mesenchyme [12]. The dental follicle develops and forms the future periodontal ligaments supporting the tooth in the alveolus [15]. Dental follicle is a component of the developing tooth complex that is vital for tooth eruption [5]. In addition to molecular and morphologic changes, dental follicle can give rise to spectrum of odontogenic lesions ranging from benign cysts such as dentigerous cysts to life threatening tumors including carcinoma [5].
HeDF is clinically significant as it mimics other pathological soft tissue conditions such as eruption cyst [9], eruption sequestrum [13], parulis [2] and pyogenic granuloma [14]. Due to the unique pathological findings associated with HeDF, recognition of this gingival lesion is important as it represents normal yet, early emergence of the tooth follicle [2]. Clinically, the lesion is asymptomatic Lesion Description: On clinical examination, the lesion appeared as a smooth, pink, sessile, papule measuring 3mm in diameter and 1.5 mm in height on the alveolar mucosa overlying the unerupted, upper, left, permanent lateral incisor (Figure 2A). The consistency of the lesion was spongy on palpation. Radiographically, the eruption of immature upper, left, permanent lateral incisor was noted with a space discrepancy and a thin amount of overlying alveolar mucosa (Figure 2B). The lesion resolved and the tooth erupted without intervention or complications, except for crowding.
Figure 2B: Periapical radiograph revealed an immature permanent lateral incisor with a space discrepancy but no bony obstruction.
but could cause periodic gingival bleeding from the site or cause secondary infection [2]. Inaccurate diagnosis of HeDF can lead to unnecessary surgical intervention [2].
External mechanical pressure from teething rings, gum pads massages, normal mastication can contribute to perforation of the alveolar mucosa overlying the developing tooth bud during near-eruption stage [2]. This case series provide anecdotal evidence that non-nutritive sucking habits could be an additional etiologic factors that may lead to increased intraoral pressures, allowing for herniation of the dental follicle associated with an erupting tooth. After herniation of the follicle, the HeDF is exposed to oral insults including trauma leading to bleeding, irritation, and infection. This case series further identifies potential association of non-nutritive sucking habits in patients with HeDF finding.
These cases underscore the importance of a conservative approach in asymptomatic HeDF cases, allowing natural resolution or simple curettage while avoiding invasive surgical intervention. For symptomatic or progressive HeDF cases, timely surgical intervention can effectively resolve symptoms and prevent complications. Most literature reviews contain articles on hyperplastic dental follicles rather than HeDF, as the former is more commonly documented [16]. Although both conditions involve problems in the dental follicle, the hyperplasic dental follicle refers to tissue enlargement while HeDF describes displacement of a dental follicle into the overlying soft tissues. Unlike HeDF, hyperplastic dental follicle can cause delayed eruption or tooth displacement. At this time, there is no evidence to support the association of hyperplastic dental follicle with HeDF finding [16].
This case series also emphasizes that HeDF can be seen in both anterior and posterior regions of the oral cavity. Clinically, HeDF may present as a soft-tissue swelling that may be mistaken for pyogenic granuloma or soft tissue abscess. Radiographic imaging is essential for accurate diagnosis, as it reveals the normal position and size of the follicle relative to the developing or erupting tooth. In the future, it would be valuable to study additional cases of HeDF to understand the causative factors, prevalence, and site predilection. From this case series and the previously published solitary case [2] it is clear that the HeDF finding coincided with the eruption timing of the underlying tooth. It would be interesting to study the pathophysiologic basis and molecular signaling underlying the emergence of HeDF. Thus, further studies are needed to support the association of HeDF with non- nutritive dental habits and other associated clinical findings.
Conclusion
This case series provided two cases of HeDF with detailed clinical and radiographic findings to create awareness among dental providers for appropriate diagnosis and timely management of HeDF cases. HeDF can be seen in anterior or posterior regions of the oral cavity. This case series highlights that a non-nutritive sucking habit could be an etiologic factor for HeDF. This case series also intends to attract attention of oral and dental researchers to study the mechanistic aspects underlying HeDF.
Conflicts of Interest
Authors declare no conflicts of interests.
References
-
Buchner A, Shnaiderman A, Vared M (2010) Pediatric Localized Reactive Gingival Lesions: A Retrospective Study from Israel. Pediatr Dent 32(7): 486-492.
-
Geneser MK, Hellstein JW, Flaitz CM (2014) Oral and Maxillofacial Pathology Case of the Month. Herniated Dental Follicle. Tex Dent J 131(2): 116-117, 164-165.
-
Gupta A, Shrestha P, Poudyal S, Kumar S, Lamichhane RS, et al. (2023) Prevalence and Distribution of Oral Mucosal Lesions and Normal Variants among Nepalese Population. Biomed Res Int 9375084.
-
Saraswathi TR, Ranganathan K, Shanmugam S, Sowmya R, Narasimhan PD, et al. (2006) Prevalence of Oral Lesions in Relation to Habits: Cross-Sectional Study in South India. Indian J Dent Res 17(3): 121-125.
-
Bastos VC, Gomez RS, Gomes CC (2022) Revisiting the Human Dental Follicle: From Tooth Development to its Association with Unerupted or Impacted Teeth and Pathological Changes. Dev Dyn 251(3): 408-423.
-
Wise GE (2009) Cellular and Molecular Basis of Tooth Eruption. Orthod Craniofac Res 12(2): 67-73.
-
Nieminen P (2009) Genetic Basis of Tooth Agenesis. J Exp Zoolog B Mol Dev Evol 312B(4): 320-342.
-
Amaral-Freitas G, Brasileiro CB, Zarzar PM, Ferreira FM (2020) Rare Dental Developmental Disturbance in Primary and Permanent Teeth Following Trauma Prior to Tooth Eruption: Case Report. Dent Traumatol 36(1): 79-83.
-
Bodner L, Goldstein J, Sarnat H (2004) Eruption Cysts: A Clinical Report of 24 New Cases. J Clin Pediatr Dent 28(2): 183-186.
-
Bastos VC, Vitório JG, Martins-Chaves RR, Leite-Lima F, Lebron YAR, et al. (2021) Age-Related Metabolic Pathways Changes in Dental Follicles: A Pilot Study. Front Oral Health 2: 677731.
-
Suri L, Gagari E, Vastardis H (2004) Delayed Tooth Eruption: Pathogenesis, Diagnosis and Treatment. A Literature Review. Am J Orthod Dentofac Orthop 126(4): 432-445.
-
Frazier-Bowers SA, Puranik CP, Mahaney MC (2010) The Etiology of Eruption Disorders-Further Evidence of a ‘Genetic Paradigm’. Semin Orthod 16(3): 180-185.
-
Queiroz AMD, Rocha CT, Silva LABD, Brentegani LG, Silva RABD, et al. (2012) Eruption Sequestrum--Case Report and Histopathological Findings. Braz Dent J 23(6): 764- 767.
-
Gordón-Núñez MA, Carvalho MDV, Benevenuto TG, Lopes MFF, Silva LMM, et al. (2010) Oral Pyogenic Granuloma: A Retrospective Analysis of 293 Cases in a Brazilian Population. J Oral Maxillofac Surg 68(9): 2185-2188.
-
Schmitd LB, Bravo-Calderón DM, Soares CT, Oliveira DT (2014) Hyperplastic Dental Follicle: A Case Report and Literature Review. Case Rep Dent 251892.
-
Puranik CP, Ghuman T, Flaitz C (2023) Clinical, Radiographic and Histopathologic Evaluation of Multiple, Non-Syndromic Hyperplastic Dental Follicles: A Unique Pediatric Case Report. Open Access J Dent Sci 7(4): 1-7.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells