Adjunctive Antimicrobials in Nonsurgical Periodontitis Treatment: A Review of Recent Trials and Indications
This review collected the latest evidence from clinical trials on antimicrobials used as adjunctive medications for the mechanical management of periodontitis, a common condition affecting teeth that leads to tooth loosening and tooth loss. A search was conducted on PubMed in May 2024 to identify human clinical trial reports published in the last five years in English with a follow-up time of at least six months. This review included 29 randomized clinical trials. Nine trials studied the adjunctive use of systemic antibiotics, five investigated topical agents, and fifteen applied various antimicrobial photodynamic therapy (aPDT) protocols. The results of the included studies are discussed in the context of the latest evidencebased guidelines for the treatment of periodontitis. Adjunctive systemic antibiotics may benefit patients in selected severe periodontitis cases, providing clinical and subgingival microbiological improvements lasting more than six months when used with subgingival instrumentation. Localized treatment investigated in these studies demonstrated that aPDT and new locally delivered antimicrobials like ozone, 1% melatonin and 5% tea tree oil gel may provide benefits. Further research is needed to ensure more efficient uses for local delivery to provide a clinically significant improvement to the outcome of subgingival instrumentation in the treatment of periodontitis.
Abbreviations
PDL: Periodontal Ligament; CAL: Clinical Attachment Loss; Ca: Calculus; BOP: Bleeding On Probing; SRP: Scaling and Root Planing; aPDT: Antimicrobial Photodynamic Therapy; RCTs: Randomized Controlled Trials; MET: Metronidazole; AMOX: Amoxicillin; AZI: Azithromycin; SPT: Supportive Periodontal Therapy; NSPT: Non-Surgical Periodontal Therapy; SRP: Scaling and Root Planing; RPP: Residual Periodontal Pockets; CP: Chronic Periodontitis; T2D: Patient with type 2 Diabetes; HbA1c: Glycated Hemoglobin Percentage;. GCF: Gingival Crevicular Fluid; ICG: Indocyanine Green; PTC: Phenothiazine Chloride; MB: Methylene Blue; PD: Pocket Depth; CAL: Clinical Attachment Loss; BOP: Bleeding on Probing; Aa: Aggregatibacter actinomycetemcomitans; Pg: Porphyromonas gingivalis; Tf: Tannerella forsythia; Pi: Prevotella intermedia; Sp: Salvadora persica
Introduction
The scientific literature suggests that periodontitis affects a significant portion of the general population, impacting general health, oral health and overall quality of life [1]. The direct cost of periodontitis has been estimated to be 54 billion dollars worldwide. This oral disease is characterized by the destruction of the tissue attachment around teeth, leading to their potential loss. Establishment of a dysbiotic subgingival biofilm leads to periodontitis. Illustrations of alveolar bone (B), periodontal ligament (PDL) and tooth in health and in periodontitis are shown in Figure 1. The estimated percentage of the global population afflicted by the disease varies depending on severity. For severe cases, a report previously estimated that 11.2% of the global population was affected [2]. When all presentations of periodontitis are included, a prevalence close to 50% could be found [3]. Furthermore, the literature suggests that there is an association between periodontitis and adverse health outcomes like premature death, diabetes and cardiovascular disease [1].
![Figure 1: The estimated percentage of the global population afflicted by the disease varies depending on severity. For severe cases, a report previously estimated that 11.2% of the global population was affected [2]. When all presentations of periodontitis are included, a prevalence close to 50% could be found [3]. Furthermore, the literature suggests that there is an association between periodontitis and adverse health outcomes like premature death, diabetes and cardiovascular disease [1].](/fulltextimages/13668/fig_1.png)
Figure 1: Illustrations of alveolar bone (B), periodontal ligament (PDL) and tooth in health and in disease. (a) The healthy periodontal ligament and bone crest are localized 2–3 mm from tooth crown (Cr), with the gingival crevice depth (PD) varying from 1 to 3 mm, as shown using the UNC15 standardized probe marked at every millimeter. (b) A site affected by periodontitis presents an increased PD and subgingival biofilm on calculus (Ca) adherent to the root surface (R). Periodontal ligament destruction and bone resorption adjacent to the contaminated root surface represent clinical attachment loss (CAL).
Periodontitis is classified using a staging and grading process [4]. The most recent periodontitis classification system based on the 2017 World Workshop is shown in Table 1. Staging is based on the increasing severity of the destruction of tissues supporting the normal function of a tooth. Patients affected by Stage I or II periodontitis present milder, more easily managed disease, while Stage III or IV periodontitis cases are characterized by more severe periodontitis, causing tooth loss, the likely need for surgical intervention and a potential impaired ability to chew. An A, B or C grade is assigned to a patient to describe the progression of the destruction of supportive tissue around teeth. Grade A presents the slowest progressing disease, while Grade C presents the most aggressive disease. Additionally, the grading of periodontitis in a patient is adjusted using modifiable risk factors, which have been shown in prospective studies to increase the incidence and rapidity of periodontal destruction. The two risk factors used in this study are poorly controlled type 2 diabetes and smoking. Other risk factors that may be targeted to improve periodontitis control include physical activity and weight loss [1]. The health or disease of the periodontium is assessed via three principal measurements: the clinical attachment level (CAL) in millimeters, the periodontal pocket depth (PD) in millimeters and the presence of bleeding on probing (BOP) [4, 5]. The clinical attachment level is an indicator of the severity of the destruction of supporting tissue around teeth [5]. Pocket depth is an important clinical parameter when evaluating periodontal patients, with PDs of 6 mm or more being associated with a higher risk of progression and tooth loss [6]. The absence of BOP is an important predictor of periodontal stability [5].
| Periodontitis Severity and Complexity | ||||||
|---|---|---|---|---|---|---|
| Stage I | Stage II | Stage III | Stage IV | |||
| Initial Disease | Moderate Disease | Severe Disease, risk of tooth loss | Severe Disease, potential loss of all teeth | |||
| Progression risk | Grade A | Low risk | Patient assigned Stage and Grade | |||
| Grade B | Moderate risk | |||||
| Grade C | High risk |
Table 1: Most recent periodontitis staging and grading system based on the 2017 World Workshop [4].
The treatment of periodontitis has mostly been focused on the mechanical removal of its main etiology: dysbiotic dental plaque and associated mineralized deposits on the tooth root. The initial non-surgical step in periodontitis therapy is defined as scaling and root planning (SRP) in most of the periodontology literature, but other terms are increasingly being used, such as subgingival instrumentation [1, 7, 8]. This instrumentation is sometimes combined with antibiotics, typically systemic or locally administered to improve patient outcomes [9, 10]. Amoxicillin and metronidazole in combination is the most commonly investigated systemic adjunctive agent, while minocycline microspheres are often used when patients are selected for local delivery of antibiotics [9, 10]. Another emerging means of reducing the bacterial load within periodontal pockets is using lasers to potentiate the antimicrobial effect of a photosensitizer [11]. Known as antimicrobial photodynamic therapy (aPDT), this field has been difficult to study due to great variability in the method of delivery to patients, antimicrobial agents used and paired laser’s parameters. aPDT is a minimally invasive approach well tolerated by patients, with very little potential to encourage the emergence of resistant microorganisms.
As antibiotic resistance continues to rise, preventive strategies can increase the time available to develop new agents and modalities. These include guideline-based and culture-driven antibiotic prescriptions [12]. This review will gather and present the most recent available evidence from clinical trials regarding the clinical and microbiological effects of adjunctive antimicrobial agents used in the non- surgical treatment of periodontitis.
Materials and Methods
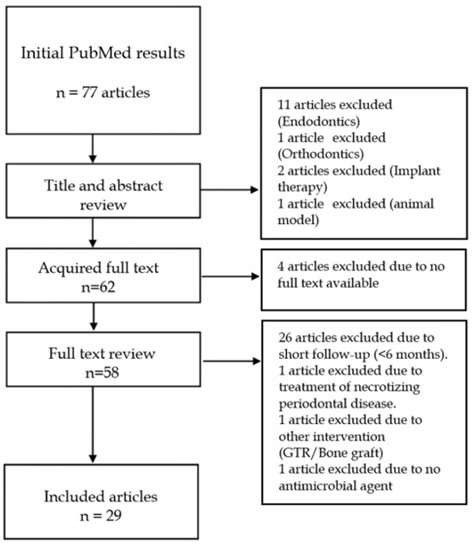
A search of randomized controlled trials (RCTs) published in the last five years was conducted in May 2024 in PubMed using the following search query: ((“periodontal disease”[All Fields]) OR (“periodontitis”[All Fields]) OR (“periodontal pocket”[All Fields])) AND ((“antimicrobial”[All Fields]) OR (“antibiotic”[All Fields])). The search was limited to publications in English on human subjects. This customized search on recent RCTs investigating periodontitis treatment using antimicrobial agents yielded 77 articles. Articles with a subject other than periodontitis treatment, as well as articles focused on the surgical management of periodontitis, the management of periimplantitis and studies not including an adjunctive agent were excluded. The literature search results, reviewing process and reasons for the exclusions are shown in Figure 2. A title and abstract review led to the exclusion of 15 articles. The remaining 62 articles were requested in full text for continued review. Four articles were not available and had to be excluded. After performing full-text reviews of the 58 remaining articles, 29 articles did not satisfy this review’s inclusion criteria, most importantly because of follow-up periods lasting less than 6 months. The remaining 29 papers were included in this review.
Results
The current review included 29 publications. Nine randomized controlled trials investigated systemic antibiotics as an adjunctive to subgingival instrumentation for periodontitis management. Experimental designs and results of randomized controlled trials on adjunctive systemic antibiotics with subgingival instrumentation are described in Table 2. Five out of nine studies used amoxicillin in combination with metronidazole in their treatment arm [13, 14, 15, 16, 17]. All studies on systemic antibiotics were performed during the initial phase of non-surgical treatment: subgingival instrumentation. The trials selected included patients with advanced periodontitis, i.e., at least Stage III. Three studies formulated their inclusion criteria to recruit patients presenting a rapid progression of the disease, and one of these studies clearly selected patients under 30 years old [14, 16, 18]. One study selected patients with type 2 diabetes [15]. All others selected systemically healthy patients. The follow-up period for systemic antibiotics ranged from six months to five years. Six of the nine studies were double- blind designs [13, 15, 17, 18, 19, 20]. The remaining used a triple- blind protocol [14, 16, 21]. All the trials used individual patients as a randomization unit. Seven investigations used a placebo in their control group [13, 15, 16, 17, 19, 20, 21]. Two trials used adjunctive amoxicillin/metronidazole as active controls [14, 18]. Cosgarea R, et al. [14] compared three days of the antibiotic combination in their test to the most used seven days of amoxicillin/metronidazole dosing in their control [14]. Araujo C, et al. [18] and colleagues compared clarithromycin in their test to a control receiving adjunctive amoxicillin/metronidazole, with both groups receiving adjunctive systemic antibiotics for seven days [18]. Three of the studies found favorable differences in microbiological analysis lasting six months [16, 17, 19]. Two of the three studies used amoxicillin/metronidazole [16, 17]. The remaining study used azithromycin [19]. Statistically significant improvements in clinical outcomes compared to a control using a placebo were only found in two studies [16, 17].
| (Ref.) Study | Random ization | Blinding | Population | Treatment Phase | Treatment | Control/ Placebo | n | Follow- Up (Months) | Results |
|---|---|---|---|---|---|---|---|---|---|
| Cosgarea R, et al. [13] | Patients | Double blind | Stage III/ IV grade B periodontitis | NSPT | SRP + [AMOX 500 mg + MET 500 mg tid × 3 days] or [AMOX 500 mg + METRO 500 mg tid × 7days] | SRP+ Placebo tid × 7 days | 75 | 12 | Antibiotic groups had reduced more than placebo periodontal pathogens numbers and detection at 6 months, and this difference was maintained at 1 year after NSPT for Pg. The results suggest that a shorter prescription may not be inferior to the commonly used 7-day AMOX+METRO for the treatment of severe periodontitis. |
| Cosgarea R, et al. [14] | Patients | Triple blind | Stage III/ IV grade C periodontitis, healthy | NSPT | SRP + AMOX 500 mg + MET 500 mg tid × 3 days followed by placebo pills tid × 4 days | SRP + AMOX 500 mg+ MET 500mg tid × 7 days | 50 | 6 | A 3-day course of antibiotics was not inferior to a 7-day course and had less frequent adverse events, potentially improving benefits/harms ratio for the AMOX/MET adjunct to SRP (3 adverse events in a 3-day protocol versus 15 in a 7-day protocol). |
| Cruz D, et al. [15] | Patients | Double blind | Severe periodontitis, T2D | NSPT | SRP + AMOX 500 mg + MET 400 mg tid × 7days SRP + placebo tid × 7 days | SRP + placebo tid × 7 days | 25 | 5 years | T2D Patients recalled 5 years after NSPT with antibiotic treatment presented with better clinical parameters than SRP-only patients when comparing their respective pretreatment baselines. Microbiological flora effects were no longer significantly different in favor of the treatment group, but red complex bacteria occupied 10%, on average, of the subgingival flora in the control compared to 7%, on average, in the treatment group. |
| Faveri M, et al. [16] | Patients | Triple blind | Stage III/IV periodontitis, <30 years old | NSPT | SRP + AMOX 500 mg + MET 400 mg tid × 14 days SRP + placebo tid × 14 days | SRP + placebo tid × 14 days | 30 | 12 | Lasting significant effects at 12 months were measured in the adjunctive AMOX/MET group compared to the control for red complex bacterial proportion and increasing beneficial Actinomyces. The antibiotic group was the only one that saw a reduction in A.a. Clinically, patients were more likely to achieve therapy goals at one year in the antibiotics group. |
| Hagenfeld D, et al. [17] | Patients | Double blind | Stage III/IV periodontitis | NSPT | SRP + AMOX 500 mg + MET 400 mg tid × 7 days | SRP + placebo tid × 7 days | 163 | 26 | BOP, percentage of sites with PD of 5mm or greater, the ribosomal sequence variant, and subgingival microbial dysbiosis indices were significantly improved by adjunctive AMOX/ MET compared to the effect of SRP alone. A reduction in putative pathogens was significantly greater in the test group up to 26 months after treatment. |
| Araujo C, et al. [18] | Patients | Double blind | Generalized aggressive periodontitis | NSPT | SRP + CLA 500 mg bid × 7days | AMOX 500 mg + MET 400 mg tid × 7 days | 46 | 6 | CLA performed as well as AMOX + MET in improving PD and CAL. |
| Cuk K, et al. [19] | Patients | Double blind | Stage III/IV periodontitis patients | NSPT | SRP + AZI 500 mg qd × 3days | SRP + placebo | 40 | 6 | No difference was found in adjunctive use of AZI in residual pockets at a probing depth of 5 mm or more after NSPT compared to SRP alone. Aa, Pg and Cr were more significantly reduced in numbers in the test group. More specifically, Aa and Cr were more often no longer present in the AZI group. |
| Povsic K, et al. [20] | Patients | Double blind | Stage III/IV periodontitis | NSPT | SRP + AZI 500 mg qd × 3days | SRP+ placebo tid × 3 days | 40 | 12 | No significant difference in the number of PDs of 5 mm or more with BOP compared to SRP + placebo. |
| Morales A, et al. [21] | Patients | Triple blind | Stage III periodontitis, healthy | NSPT | SRP + [L. rhamnosus SP1 probiotic qd × 3 months] or [AZI 500 mg qd × 5 days] | SRP + Placebo qd × 5 days + Placebo qd × 3 months | 47 | 12 | No significant differences were measured in PD, CAL or BOP; no microbiological tests were performed. |
Table 2: Experimental designs and results of randomized controlled trials on adjunctive systemic antibiotics with subgingival RCT: randomized controlled trial. MET: metronidazole. AMOX: amoxicillin. AZI: azithromycin. CLA: clarithromycin. NSPT: non- surgical periodontal therapy. SRP: scaling and root planing. T2D: patient with type 2 diabetes. bid: twice daily. tid: three times daily. qd: once daily. Aa: A. actinomycetemcomitans. Pg: P. gingivalis. Cr: C. rectus. PD: pocket depth. CAL: clinical attachment loss. BOP: bleeding on probing. Table 2: Experimental designs and results of randomized controlled trials on adjunctive systemic antibiotics with subgingival instrumentation (n=9).
Five RCTs were selected using local delivery agents. The experimental designs and results of randomized controlled trials on adjunctive local delivery agents with subgingival instrumentation are given in Table 3. Four of five studies used randomized patients [22, 23, 24, 25]. Four of the five studies did not report using a placebo [23, 24, 25, 26]. One study used a split-mouth design to randomize pairs of intrabony defects [26]. Most studies recruited patients at the initial stage of periodontal treatment, and one study investigated the treatment of patients with residual pockets through supportive periodontal therapy (SPT) [25]. Three studies were double-blind designs [22, 23, 26]. One trial followed a single-blind protocol [24]. One investigation stated that only the laboratory analyst was blinded to the patient assignment [25]. Single studies found significant clinical improvement using treatment protocols based on adjunctive tea tree oil, melatonin and ozonated water [23, 24, 26].
| (Ref.) Study | Randomization | Blinding | Population | Treatment Phase | Treatment | Control/Placebo | n | Follow-Up(Months) | Results |
|---|---|---|---|---|---|---|---|---|---|
| Ilyes I, et al. [22] | Patients | Double blind | Stage III/IV periodontitis | NSPT | SRP + [PTG] or [DOX] | SRP + Placebo gel | 64 | 6 | No significant difference was found in PD, CAL, BOP or numbers of keystone periodontal pathogens between local delivery groups and SRP with a placebo gel. |
| Rapone B, et al. [23] | Patients | Double blind | Moderate-to-severe periodontitis, healthy | NSPT | SRP + OZ irrigation associated with ultrasonic instrumentation | SRP | 90 | 6 | Clinical parameters for PPD, CAL and BOP show a significant difference in favor of SRP with the adjunctive ozone protocol compared to SRP alone. |
| Taalab MR, et al. [24] | Patients | Single blind | Stage II periodontitis | NSPT | SRP + TTO | SRP | 30 | 6 | Significantly greater improvement compared to SRP alone was seen with adjunctive TTO, measured as a greater reduction in MMP-8, and a statistically greater improvement in CAL at six months of follow-up. |
| Teles FRF, et al. [25] | Patients | Laboratory blind | Stage III/IV periodontitis SPT, active NSPT within 1 year | RPP | SRPSRP + MM at PD>4mm | SRP | 32 | 6 | No difference in PD, CAL or BOP, minocycline resistant bacteria were increased at 1 month and to a lesser degree at 6 months post treatment. Aa, Tf and Pg rarely presented resistance to minocycline. |
| Gonde NP, et al. [26] | Split mouth, intrabony defect pair | Double blind | Periodontitis with bilateral intrabony defects | NSPT | SRP + MEL | SRP | 22 | 6 | PD, CAL improvements and radiographic bone fill were significantly greater in the adjunctive MEL group compared to SRP in paired intrabony defects. |
Table 3: Experimental designs and results of randomized controlled trials on adjunctive local delivery agents with subgingival RC
Table 3: Experimental designs and results of randomized controlled trials on adjunctive local delivery agents with subgingival RCT: randomized controlled trial. MM: minocycline microspheres. TTO: 5% tea tree oil gel. PTG: piperacillin and tazobactam gel. DOX: 14% doxycycline gel. MEL: 1% melatonin gel. OZ: ozone treatment. NSPT: non-surgical periodontal therapy. SRP: scaling and root planning. RPP: residual periodontal pocket after initial subgingival instrumentation. Aa: A. actinomycetemcomitans. Tf: Tannerella forsythia. Pg: P. gingivalis. Cr: C. rectus. PD: pocket depth. CAL: clinical attachment loss. BOP: bleeding on probing. MMP-8: matrix metalloproteinase-8. Table 3: Experimental designs and results of randomized controlled trials on adjunctive local delivery agents with subgingival instrumentation (n = 5).
Fifteen publications in the last five years combined a photosensitizer and a diode laser to treat periodontitis. The experimental designs and results of randomized controlled trials on adjunctive antimicrobial photodynamic therapy with subgingival instrumentation are presented in Table 4. Seven studies used a split mouth design [27, 28, 29, 30, 31, 32, 33]. Five investigations randomized patients [34, 35, 36, 37, 38]. The final three experimental designs randomized the sites treated by either treatment or a control [39, 40, 41]. Three studies investigated photodynamic therapy in patients with type 2 diabetes [31, 35, 36]. Four studies designated periodontitis Stage III as the minimum disease severity for recruited patients [27, 34, 35, 39]. Nine studies were conducted at the initial phase of periodontal treatment [27, 30, 32, 33, 34, 35, 37, 40, 41]. The remaining six reports investigated the effects of photodynamic therapy in residual pockets found in patients enrolled in a maintenance program [28, 29, 31, 36, 38, 39]. In total, six photosensitizers were investigated, using diode lasers of wavelengths ranging from 625 nm to 909 nm. Six studies used repeated applications of photodynamic therapy, without repeating subgingival instrumentation [28, 29, 34, 35, 39, 40]. Four studies used a type of irrigation in the control group as a placebo, either using saline or the selected photosensitizer without laser irradiation [28, 31, 40, 41]. Two studies used simulated laser irradiation as part of their control [28, 29]. One study compared repeated aPDT to subgingival instrumentation with systemic antibiotics [34]. Eight of the included studies reported clinical improvement in their treatment arm compared to the control after six months of follow-up [27, 29, 33, 34, 35, 37, 38]. The two studies investigating phenothiazine chloride aPDT found clinical changes lasting up to six months [34, 38]. Of the six protocols using indocyanine green (ICG), two found no significant differences [30, 40]. Of the remaining studies on ICG, one found significant clinical improvement in patients with type 2 diabetes, regardless of the level of glycemic control [27]. Three other experiments using ICG found a significant clinical advantage in favor of the test group at six months follow-up [28, 33, 37]. Methylene blue-based aPDT was used in four protocols [32, 35, 36, 39]. In the non-surgical periodontal therapy (NSPT) phase of periodontal treatment, one study found a significant improvement in clinical parameters in the aPDT group [35], while the other found no difference between the groups [32]. In the treatment of residual pockets, both studies using methylene blue found no difference in periodontal parameters at six months [36, 39]. Methylene blue aPDT was compared to surgical access for debridement, with surgical access presenting a greater improvement in PD at initially deeper sites, and also greater recession compared to the aPDT treatment [39]. Antimicrobial photodynamic therapy caused significantly less dentin hypersensitivity.
| (Ref.) Study | Random ization | Blinding | Population | Treatment Phase | Treatment | Control/ Placebo | n | Follow- Up (Months) | Results |
|---|---|---|---|---|---|---|---|---|---|
| Al-Momani MM, et al. [27] | Split mouth | Double blind | Stage III periodontitis, T2D. | NSPT | G1: Non- diabetes patient G2: T2D G3: T2D (HbA1c>10%) Test subgroups: SRP + diode laser (810 nm) + ICG | Control subgroups: SRP alone | 50 | 6 | In patients without diabetes, PD improvement and CAL improvement were greater in the test group at 6 months. In the patient with well-controlled diabetes group, improvements in BOP%, PD, and CAL were all greater at 6 months than in the control group. In patients with poorly controlled diabetes, BOP% and CAL both presented greater improvements at 6 months than the control. Across groups, aPDT led to greater reductions in Pg and Tf at 6 months compared to SRP alone. |
| Costa FO, et al. [28] | Split mouth, contralateral quadrants | Unclear | SPT patients. | RPP | SRP + diode laser (909 nm) + ICG. aPDT on day 1 and day 15 | SRP + sham aPDT saline irrigation | 24 | 6 | No difference in CAL, PD or plaque index. The test group presented greater reductions in BOP, periodontal inflamed surface area index, Pg and Aa. |
| Harmouche L, et al. [29] | Split mouth random block for quadrants | Double blind | SPT, healthy, non-smoker. | RPP | SRP + diode laser (625–635 nm) + toluidine blue. aPDT at day 1, day 7, and 3 months | SRP+ sham irradiation | 36 | 6 | A reduction in PD > 5mm in the aPDT group compared to SRP alone. The authors noted greater responses in non- smokers and patients compliant with their home oral care. |
| Hill G, et al. [30] | Split mouth, pattern assignment | Blinded labora tory | CP, healthy, non-smoker. | NSPT | SRP + diode laser (808 nm) + ICG | SRP | 20 | 6 | No significant change in BOP, CAL and PD after six months of follow-up. |
| Ivanaga CA, et al. [31] | Split mouth, quadrants | Single blind | SPT, T2D. | RPP | SRP + [diode laser (465–485 nm)] or [laser with curcumin (aPDT)] or [curcumin alone] | SRP + saline irrigation | 23 | 6 | Three months of follow-up showed a greater increase in CAL gain in T2D patients assigned to the diode laser and diode laser and curcumin (aPDT) groups, with no difference at six months when compared to the control group. |
| Katsikanis F, et al. [32] | Split mouth, quadrants | Single blind | Moderate- tosevere periodontitis, healthy. | NSPT | SRP + [diode laser (940 nm)] or [diode laser (670 nm) + MB] | SRP | 21 | 6 | No significant difference in PD or BOP measured after six months of follow-up. |
| Sukumar K, et al. [33] | Split mouth, mandibular posterior sextants | Single blind | Stage II or more periodontitis. | NSPT | SRP + diode laser (810 nm) + ICG | SRP | 30 | 6 | All clinical parameters (plaque index, gingival index, BOP, PD, CAL) presented greater improvements in the aPDT group compared to the control. Microbiological analysis revealed that aPDT groups presented a greater reduction in periodontal pathogens at six months. |
| Al-Khureif AA, et al. [34] | Patients | Unclear | Stage III/ IV Grade C periodontitis. | NSPT | SRP + diode laser (670 nm) + PTC. aPDT on days 1, 3, 7, and 14 | SRP +AMOX 500 mg+ MET 500 mg | 17 | 6 | aPDT presented a greater improvement than the control in sites with PDs of 7 mm or greater for PD and CAL at 6-month follow-up. Only the control group treated with adjunctive AMOX/MET presented an improvement in GCF cytokines (reduced IL-17, increased IL-10). |
| Cláudio MM, et al. [35] | Patients | Single blind | Stage III/ IV Grade C periodontitis, T2D. | NSPT | SRP + diode laser (660 nm) + MB. aPDT on days 1, 2, and 4 | SRP | 31 | 6 | Significantly greater reductions in mean PD and residual pockets at 6 months for the test group. No differences were found in the numbers of Pg and Pi. |
| Cláudio MM, et al. [36] | Patients | Double blind | T2D, SPT patients. | RPP | SRP + [oxygen releasing gel + diode laser (660 nm) + MB] or [oxygen releasing gel] | SRP | 45 | 6 | No significant differences at 6-month follow-up in the management of poorly controlled diabetes in patients (HbA1c > or equal to 7%). |
| Niazi FH, et al. [37] | Patients | Unclear | CP, healthy. | NSPT | SRP + [Sp gel] or [ICG + diode laser (810 nm)] | SRP | 73 | 6 | The aPDT group presented a significantly greater PD reduction at 6 months in initially deep sites (6mm or more). The Sp gel group presented a significantly greater reduction in BOP at 6 months. |
| Schär D, et al. [38] | Patients | Single blind | SPT. | RPP | SRP + diode laser (670 nm) + PTC | SRP | 40 | 6 | The test group presented a statistically significant difference in BOP improvement at 6 months; otherwise, both treatment and control performed the same in improving CAL and PD. |
| Andere NMRB, et al. [39] | Residual pockets | Single blind | Stage III/ IV Grade C periodontitis in SPT. | RPP | SRP + diode laser (660 nm) + MB. aPDT on days 1, 2, 7, and 14 | OFD using MPPF | 46 | 12 | Comparing OFD to repeated aPDT, the aPDT group presented a significantly greater 14-day improvement in cytokine profile. OFD with MPPF presented greater improvement in PD at initially deep sites. OFD also presented greater gingival recession and dentin hypersensitivity compared to the test. Also, OFD reduced numbers of Aa, while the aPDT treatment did not do so. |
| Annunziata M, et al. [40] | Sites presenting PD > 4 mm | Single blind | Generalized stage II/III periodontitis, healthy. | NSPT | SRP + diode laser (810 nm) + ICG aPDT on days 7 and 28 | SRP + ICG irrigation | 24 | 6 | No significant difference in PD, CAL and BOP after six months of follow-up. |
| Silva DNDA, et al. [41] | Residual pockets | Double blind | Periodontitis, healthy. | NSPT | SRP + Diode laser (660 nm) + chloro aluminum phthalo cyanine | SRP + saline irrigation | 63 | 6 | No significant difference in PD, CAL and BOP after six months of follow-up. |
Table 4: Experimental designs and results of randomized controlled trials on adjunctive antimicrobial photodynamic therapy RCT: randomized controlled trial. aPDT: antimicrobial photodynamic therapy. Diode laser (wavelength of laser used). MET: metronidazole. AMOX: amoxicillin. AZI: azithromycin. SPT: supportive periodontal therapy. NSPT: non-surgical periodontal therapy. SRP: scaling and root planning. RPP: residual periodontal pockets following initial subgingival instrumentation. CP: chronic periodontitis. T2D: patient with type 2 diabetes. HbA1c: glycated hemoglobin percentage. GCF: gingival crevicular luid. ICG: indocyanine green. PTC: phenothiazine chloride. MB: methylene blue. PD: pocket depth. CAL: clinical attachment loss. BOP: bleeding on probing. Aa: A. actinomycetemcomitans. Pg: P. gingivalis. Tf: Tannerella forsythia. Pi: Prevotella intermedia. Sp: Salvadora persica. Table 4: Experimental designs and results of randomized controlled trials on adjunctive antimicrobial photodynamic therapy with subgingival instrumentation (n = 15).
Discussion
Systemic Antibiotics in the Treatment of Periodontitis
The paradigm has shifted from attributing periodontitis to specific putative microbiological pathogens to an understanding that it is likely caused by a change from commensal flora to opportunistic pathogenic bacteria [42, 43]. Using antibiotics can reduce the bacterial load following NSPT and eliminate periodontal pathogens, which can stay hidden within the periodontal tissues [10, 44]. Teughels W, et al. [10] concluded after a systematic review on antibiotics and periodontitis treatment that the evidence supported a small but statistically significant improvements in PD (a weighted mean difference of 0.485 mm), CAL (a weighted mean difference of 0.285 mm), and BOP as well as a decreased number of residual pockets [10]. The use of amoxicillin and metronidazole was the most investigated systemic antibiotic treatment and presented the most adverse events. These results support the most recent clinical periodontitis treatment guidelines, which recommends considering systemic antibiotics only when treating severe periodontitis in young adults and recommends against their routine use [1]. This is important, especially since unnecessary antibiotics and their excessive use in both humans and animals are involved in the rise of antimicrobial resistance worldwide [12].
Cosgarea R, et al. [13] found that periodontal pathogens were still reduced in number at six months, and Porphyromonas gingivalis was still reduced a year after the administration of a 7-day regimen of amoxicillin and metronidazole [13]. Cosgarea R, et al. [14] also tested a 3-day course of an antibiotic combination for treating patients with at least Stage III Grade C periodontitis, a fast progressing and advanced disease [14]. The authors found that the 3-day course and the standard 7-day prescription were nearly identical in reducing residual pockets (6 mm or greater) after six months of follow-up. Both treatments led to improvements in clinical parameters, microbiological analysis and inflammatory markers measured in the gingival crevicular fluid (GCF). Five times as many adverse events were observed in the full 7-day course compared to the 3-day course of amoxicillin/metronidazole. Cruz D, et al. [15] recalled patients who had been treated five years prior with subgingival instrumentation and a combination of metronidazole and amoxicillin [15]. They found that without supportive therapy, clinical gains were mostly lost after five years for both the treatment and the control groups. Hagenfeld D, [17] used 16s rRNA sequencing to explore subgingival microbiota diversity and used the subgingival microbial dysbiosis index (SMDI) to evaluate the effects of adjunctive amoxicillin and metronidazole in severe periodontitis patients (periodontitis stage III-IV) [17]. Significant reductions in periodontal pathogens were seen up to 26 months after treatment. Faveri M, et al. [16] treated young patients with severe periodontitis and reported both clinical and microbiological data over one year of follow- up [16]. After 14 days of amoxicillin and metronidazole treatment, patients who had taken the antibiotics presented significantly greater decreases in red complex bacterial proportions, greater proportions of health-associated Actinomyces, and a greater chance of reaching endpoints of therapy. Red complex bacteria consist of Treponema denticola, Tannerella forsythia and P. gingivalis, which were increased in the subgingival samples of the patients affected by periodontitis [45, 46, 47, 48]. In addition, Aggregatibacter actinomycetemcomitans is a bacterial species specifically associated with juvenile periodontitis [49]. A specific serotype was identified as the exogenous pathogen causing periodontal breakdown. The authors then concluded that using antibiotics was justifiable in cases presenting a A. actinomycetemcomitans serotype b infection.
Araujo C, et al. [18] tested 500 mg of clarithromycin bid for seven days against the more widely used amoxicillin/ metronidazole combination [18]. Patients affected by rapidly progressing severe disease responded similarly to both antibiotic regimens. Azithromycin regimens were used for 3–5 days, with minimal-to-no clinical differences reported by the two publications included in this review [20, 21]. Morales et al. also included a probiotic treatment based on Lactobacillus rhamnosus SP1 consumption once daily for three months as an adjunct to subgingival debridement, which showed no difference compared to the control or adjunctive azithromycin group [21]. Although Cuk K, et al. [19] and colleagues found no difference in periodontal clinical parameters after using systemic azithromycin for 3 days as an adjunctive to subgingival instrumentation, they found that A. actinomycetemcomitans and Campylobacter rectus were more commonly absent in the test group [19]. The same publication reported greater decreases in A. actinomycetemcomitans, C. rectus and P. gingivalis in the adjunctive azithromycin group.
Local Delivery and Other Agents
Systemic antibiotic courses have been linked to more adverse events for patients, and their use is contributing to a community-wide rise in antibiotic resistance [1, 12]. Local delivery has the advantage of reducing adverse events, improving compliance and decreasing chances of bacteria developing resistance [50]. As an example of the low potential for increasing resistance, an investigation into locally delivered doxycycline showed a temporary increase in the proportion of resistant bacteria in the subgingival microflora, which was not present after three months or six months of follow-up [51]. Most importantly, the resistant bacteria had been identified at baseline. A recent systematic review and meta-analysis showed that, overall, local antimicrobial delivery resulted in a statistically significant decrease in mean PD of 0.365 mm and a mean CAL gain of 0.263 mm, while no increase in adverse events was found compared to the control [9]. The small difference seen, which may not be clinically meaningful, paired with the high heterogeneity between studies led to the recommendation that providers may use locally delivered antiseptics and antibiotics as adjuncts to subgingival instrumentation [1]. Most locally delivered antimicrobials studied were antibiotics, with the notable exception of chlorhexidine [9]. More specifically, previously investigated agents made commercially available included tetracycline, minocycline, doxycycline, chlorhexidine, metronidazole and piperacillin/ sodium tazobactam in combination. The articles published in the last five years included in this review investigated different locally delivered agents; these agents included antibiotics, ozonated water, tea tree oil and melatonin.
Teles FRF, et al. [25] treated residual pockets of patients with subgingival instrumentation and minocycline microspheres, finding that there was no clinical difference at six months between the use of adjunctive locally delivered antibiotics compared to subgingival instrumentation use alone [25]. There was a measurable increase in bacterial resistance to minocycline at one month after application, which was diminished but still present at 6 months of follow- up. This was the case for both plaque and saliva isolates. They also found that periodontal pathogens isolated during this study were rarely resistant to minocycline.
Four articles enrolled periodontitis patients who required initial subgingival instrumentation [22, 23, 24, 26]. Initial disease severity was variable. Taalab MR, et al. [24] enrolled Stage II periodontitis patients [24]. These patients were expected to respond well to non-surgical therapy [4]. The treatment group received adjunctive 5% tea tree oil gel, which was selected for its antimicrobial and immune- modulating potential. They found that the treatment resulted in significantly greater CAL at six months and there was also a significant reduction in the GCF levels of matrix metalloprotease 8 (MMP-8). MMP-8 is considered a host enzyme contributing to the tissue destruction seen in periodontitis. Gonde NP, et al. [26] used subgingival instrumentation and a 1% melatonin gel compared to subgingival instrumentation alone [26]. The enrolled patients had bilateral paired intrabony defects that were randomized to either the treatment or control according to a split-mouth experimental design. They found that the treatment group presented significantly better clinical and radiographic parameters, including PD reduction and bone fill calculated using cone beam computed topography. Melatonin was used for its potential as an immune modulator, improving osteoblastic differentiation.
Rapone B, et al. [23] investigated adjunctive ozonated water [23]. Through a powered unit, the treated water was used in a step-by-step oral disinfection protocol described, which included rinsing and irrigation paired with ultrasonic instruments. They found statistically significant improvements in PD, CAL and percentage BOP at six months. Ilyes I, et al. [22] used a protocol including piperacillin and tazobactam in a gel [22]. The trial also employed a treatment arm using a 14% doxycycline gel, and for the control, they used a placebo gel as the adjunctive to subgingival instrumentation. They found no differences between any of the treatment groups.
Photoactivated Antimicrobials
Photodynamic therapy is a treatment modality that has various uses in medicine and uses a photosensitizer to absorb the wavelength of a low-energy light source [11]. In turn, light absorption by the sensitizer leads to reactive oxygen species forming in the medium, effectively killing microorganisms. A systematic review from 2018 by Chambrone, et al. concluded that the evidence available at the time was insufficient to support a clinically significant difference in periodontal parameters following adjunctive photodynamic therapy for periodontitis and peri-implantitis treatment. The authors noted significant variation between studies. Wavelength of the lasers and agents used as photosensitizer are important in explaining the desired effect on bacteria and host tissues, but other determining parameters vary significantly between studies such as duration of exposure, power output and diameter of a diode tip used. These specifications should be reported by every trial protocol. The current review included 15 articles on this treatment modality.
Indocyanine green was used as a photosensitizer, and it is reported to cause cellular damage through increased intracellular temperature in free-floating bacteria and periodontal pathogens [28]. Hill G, et al. [30] used an 808 nm diode laser with ICG and found no difference compared to subgingival instrumentation alone in the residual pockets of patients in SPT [30]. Niazi FH, et al. [37] used ICG-based aPDT using an 810 nm laser as an adjunct to non-surgical periodontal therapy [37]. Patients in the treatment group presented significantly better PD reduction at six months in pockets that were 6 mm or greater in depth at baseline. In another treatment group, an adjunctive uncalibrated Salvadora persica gel was locally applied in periodontal pockets. The plant was selected for potential antimicrobial- and inflammatory-modulating properties and presented a greater reduction in BOP at six months compared to the control and aPDT groups. Sukumar K, et al. [33] also used ICG with an 810 nm diode laser for NSPT and found a significantly greater improvement in microbiological, but not clinical, parameters [33]. They found a significant reduction in periodontal pathogens at six months compared to subgingival instrumentation alone. Al-Momani MM, et al. [27] stratified patients in three groups prior to randomization: patients without diabetes, patients with diabetes presenting a glycated hemoglobin (HbA1C) percentage of less than 10% but greater than 6% and patients with more severely uncontrolled diabetes for whom HbA1C was greater than 10% [27]. Stratified groups based on glycemic control were then randomly assigned to the treatment and control subgroups. The adjunctive use of aPDT using ICG with an 810 nm diode laser led to a greater reduction in periodontal pathogens and improvement in clinical parameters in all groups, regardless of glycemic status. Annunziata M, et al. [40] used ICG aPDT with an 810 nm laser as an adjunct to subgingival instrumentation, providing three applications (day 1, 7, 28) and using ICG irrigation without laser activation as a placebo in the control subgingival instrumentation [40]. No statistical significance was found between the test and control groups at six months after treatment. Costa FO, et al. [28] investigated residual pockets in SPT patients. Patients with residual periodontal pockets were assigned to SRP with ICG aPDT (application at day 1 and day 15) or SRP with sham aPDT using saline irrigation [28]. The research group then found limited differences, with only BOP, periodontally inflamed surface area index and periodontal pathogen reductions being greater in the treatment group, while CAL and PD improvements were the same as those in the control.
Methylene blue was part of protocols developed by four authors. Katsikanis F, et al. [32] compared a higher- energy 940 nm diode laser to aPDT using a 670 nm diode laser and methylene blue [32]. They reported no significant difference six months after a single application, as both the 940 nm diode laser and the aPDT combination performed as well as subgingival instrumentation alone. Cláudio MM, et al. [35] compared adjunctive aPDT using a 660 nm diode laser with methylene blue to subgingival instrumentation alone [35]. They applied the aPDT protocol three times: once on the day of instrumentation, and they then retreated without performing further instrumentation on day 2 and day 4. The researchers found that, clinically, the mean PD and the number of residual pockets were significantly less in the test group. Andere NMRB, et al. [39] applied a similar methodology to treat residual pockets in periodontitis patients on maintenance [39]. They tested the same wavelength (660 nm) diode laser with methylene blue but applied the aPDT protocol once on the day of instrumentation, before repeating it on days 2, 7 and 14 for four exposures. Because initial subgingival instrumentation had been already performed six months prior to patients’ enrollment in the study, aPDT was compared to surgical debridement using a modified papilla preservation flap [39, 52]. This is the only study that made a comparison with open flap debridement (OFD) in the control group [39]. Andere NMRB, et al. [39] found that OFD performed better with significantly greater pocket depth reduction at initially deeper sites. In turn, OFD resulted in greater gingival recession and root sensitivity compared to the aPDT treatment of residual pockets. Inflammatory analysis of GCF found differences after two weeks in favor of aPDT in the cytokines measured, but these differences were not maintained after one year of follow- up. Only the surgical access in the control group led to a decrease in A. actinomycemtemcomitans. Cláudio MM, et al. [36] incorporated an oxygen-releasing gel into aPDT using a 660 nm diode laser and methylene blue [36]. There was also a control group using SRP alone and a group treated only with the adjunctive oxygen-releasing gel. Patients enrolled in the study had poorly controlled type 2 diabetes (HbA1C 7% or greater) and were already enrolled in SPT, presenting residual pockets requiring treatment. The results showed no difference between subgingival instrumentation alone and the repeated use of adjunctive aPDT in residual pockets.
Harmouche L, et al. [29] used another photosensitizer, toluidine blue, with a diode laser of 630 nm [29]. Patients enrolled in the study were systemically healthy patients receiving periodontal supportive therapy, presenting residual pockets requiring treatment. The aPDT test arm led to a greater reduction in the number of pockets with depths greater than 5 mm compared to subgingival instrumentation alone.
Al-Khureif AA, et al. [34] used a 670 nm diode laser with phenothiazine chloride as a photosensitizer in patients enrolled for initial subgingival instrumentation [34]. The application in the aPDT group was quadruple, starting on day 1 and continuing on days 3, 7 and 14. This is the only article using adjunctive systemic amoxicillin and metronidazole in the control group compared to aPDT. They also enrolled patients with Stage III Grade C or worse periodontitis, i.e., cases presenting with faster progression of CAL and a high level of pre-existing destruction. They found that the aPDT group improved significantly more for PD and CAL measured after six months of follow-up in sites with initially severe pocketing (7 mm or greater PD). The GCF analysis revealed that only the control group experienced improved cytokine profiles related to reduced IL-17 and increased IL-10 at six months Schär D, et al. [38]. used a 670 nm diode laser with phenothiazine chloride and compared it to subgingival instrumentation alone for the treatment of residual pockets in SPT patients [38]. The only statistical difference at six months was a greater reduction in BOP in the aPDT group; otherwise, both treatments presented similar improvements.
Ivanaga CA, et al. [31] treated residual pockets in patients with type 2 diabetes, using curcumin as a photosensitizer with a 475 nm diode laser [31]. There was another treatment group who only received pocket irrigation with curcumin, as well as a group who received pocket irradiation with the diode laser, and the control received saline pocket irrigation; all groups received subgingival instrumentation. Curcumin, an extract of Curcuma longa roots, was investigated to study its antimicrobial properties, as well as its anti-inflammatory potential. After three months, they found a statistically significant improvement in CAL gain using both the laser alone and the aPDT combination. These differences were not maintained at six months in these patients with type 2 diabetes (HbA1C percentage mean ± SD, 8.73% ± 1.82). Silva DNDA, et al. [41] investigated adjunctive chloro-aluminum phthalocyanine aPDT using a 660 nm laser for the initial subgingival instrumentation of periodontitis patients [41]. The control received subgingival instrumentation with saline irrigation, and both groups presented similar improvements after six months of follow-up.
Study Limitations
When comparing the results from the articles included in this review, care must be taken to understand the great variability in experimental protocols. Systemic agents were studied using randomized patients, while locally administered therapies like aPDT and medicated gels often were tested using split-mouth approaches. A split- mouth design allows the patient to act as their own control. When comparing results for the same patient, the authors could eliminate variability between subjects and identify a statistically significant difference with a smaller sample [9]. This was most significant in aPDT, where split-mouth randomization and the randomization of sites (periodontal pockets) were the most used experimental designs. One major consequence of split-mouth designs is the potential for a carry-across effect, where the treatment may affect more than just the target site.
Another limitation shared by many included studies in this review is the lack of a placebo/vehicle control. In particular, this was the case for most studies on local delivery [23, 24, 25, 26]. A similar trend was visible in the included studies on aPDT [27, 30, 32, 33, 34, 35, 36, 37, 39]. Specifically for aPDT, even for studies that included placebo in their control groups, there was heterogeneity in selection. Some protocols compared aPDT to active controls using systemic antibiotics and even surgical management of residual pockets [34, 39]. All the studies included in this review presented a small sample size, with only one study performing follow-up on more than 100 patients [17].
It is vital to present long-term data that justify the cost, risk of adverse events and additional treatment time incurred by using an adjunctive antimicrobial. Studies showing that statistically significant differences are maintained one year after treatment are rare, with only one aPDT trial and six out of nine adjunctive systemic antibiotic trials being identified. None of the locally administered agents were followed-up for 12 months or more. In total, 26 randomized controlled trials were also excluded from the initial 58 articles in the full-text review because of follow-up periods being less than 6 months long. Targeting patients with type 2 diabetes at a higher risk for disease progression was included in five trials. Various definitions were used to define patients with controlled and poorly controlled type 2 diabetes and guide inclusion in the studies. A threshold of seven percent HbA1C was used for uncontrolled diabetes used in the latest periodontitis staging and grading [4]. Al-Momani MM, et al. [27] considered diabetes controlled with a range from 6 to 10% [27]. Cruz D, et al. [15] and Cláudio MM, et al. [35] investigated patients with uncontrolled diabetes using a 7% glycated hemoglobin threshold [15, 35, 36]. Ivanaga CA, et al. [31] recruited diabetic patients reporting at least a 6.5% glycated hemoglobin [31]. Since poor glycemic control is associated with an increase in periodontal destruction and a decreased response to traditional treatment, the inclusion of patients with better controlled blood sugar levels in RCTs may not result in a response representative of the population most at risk of periodontitis progression, as would be found in patients with HbA1C levels greater than 7% [4, 53]. Future studies should include longer follow-up periods to help distinguish short-term benefit from lasting differences with any of the discussed agents on clinical, radiographical and microbiological outcomes. They should also use patients as a randomization unit, consider including all relevant treatment groups and controls, to identify the contribution of individual components of a combination treatment. This is especially important in the case of trials on aPDT. Complete disclosure of the selected diode laser parameters should be included. Finally, studies should also include patient- centered outcomes such as measures of discomfort during and after procedures.
Overall, the conclusions drawn from this review are limited because it did not follow the methodology of a systematic review. However, using the PubMed database, the review had a wide reach in capturing relevant published scientific articles in the past five years. The scope of the search was also limited to trials that included antimicrobials. This likely led to trials investigating agents for their immunological-modulating or bone-modulating properties such as statins being excluded in the search results [54].
Conclusions
The results of the current review support the continuing efforts being made to investigate the most efficient use of adjunctive antimicrobials for the non-surgical management of periodontitis, either initially when the patient presents or when residual pockets are seen during SPT. Systemic antibiotics have a long history of statistically significant improvement of most clinical parameters, but the small difference does not justify their use in most periodontitis patients due to high incidence of adverse events and the need for the careful use of antibiotics in the face of rising resistance [1]. RCTs investigating the use of a shorter course of amoxicillin/metronidazole for periodontitis Stage III/ IV Grade B/C treatment are needed before a shorter course can be recommended to reduce the incidence of adverse events in clinical practice. While specific indications were noted for the adjunctive use of systemic antibiotics, further better designed trials are needed to define indications surrounding adjunctive local delivery and aPDT in the non- surgical treatment of periodontitis. Research is needed to identify new locally delivered medications, with long-term trials confirming a lasting clinical improvement. Future studies should go beyond improving pocket depth, with new agents and non-invasive methods of delivery being needed to optimize healing and promote periodontal ligament regeneration in patients affected by severe periodontitis.
Author Contributions
Conceptualization: W.G.B. and L.F.W.; methodology: W.G.B. and L.F.W.; investigation: W.G.B. and L.F.W.; resources: W.G.B. and L.F.W.; data curation: W.G.B. and L.F.W.; writing- original draft preparation: W.G.B. and L.F.W.; writing—review and editing, W.G.B., L.F.W., and I.K.; project administration, W.G.B. and L.F.W.; funding acquisition, L.F.W. All the authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. This research was supported by a University of Minnesota School of Dentistry, Division of Periodontology grant (L.F.W.).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The PubMed search strategy is included within the article.
Acknowledgments
The authors thank Daya Leboeuf Roy for her support in editing and proofreading the current manuscript. The authors also thank Dao-Li Leboeuf Roy for her original illustration, seen in Figure 1 of the current manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
-
Sanz M, Herrera D, Kebschull M, Chapple I, Jepsen S, et al. (2020) Treatment of stage I–III periodontitis-The EFP S3 level clinical practice guideline. J Clin Periodontol 47(S22): 4-60.
-
Kassebaum NJ, Bernabe E, Dahiya M, Bhandari B, Murray C, et al. (2014) Global Burden of Severe Periodontitis in 1990-2010: A Systematic Review and Meta-regression. J Dent Res 93(11): 1045-1053.
-
Billings M, Holtfreter B, Papapanou P, Mitnik G, Kocher T, et al. (2018) Age-dependent distribution of periodontitis in two countries: Findings from NHANES 2009 to 2014 and SHIP-TREND 2008 to 2012. J Clinical Periodontol 45(S20): S130-S148.
-
Tonetti M, Greenwell H, Kornman K (2018) Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Periodontol 89(S1): S159-S172.
-
Lang N, Bartold P (2018) Periodontal health. J Periodontol 89(S1): S9-S16.
-
Matuliene G, Pjetursson BE, Salvi GE, Schmidlin K, Lang NP, et al. (2008) Influence of residual pockets on progression of periodontitis and tooth loss: Results after 11 years of maintenance. J Clinical Periodontology 35(8): 685-695.
-
Cobb CM (2002) Clinical significance of non-surgical periodontal therapy: an evidence-based perspective of scaling and root planning. J Clin Periodontol 29(2): 6-16.
-
Cobb CM, Sottosanti JS (2021) A re-evaluation of scaling and root planning. J Periodontol 92(10): 1370-1378.
-
Herrera D, Matesanz P, Martin C, Oud V, Feres M, et al. (2020) Adjunctive effect of locally delivered antimicrobials in periodontitis therapy: A systematic review and meta-analysis. J Clin Periodontol 47 (Suppl 22): 239-256.
-
Teughels W, Feres M, Oud V, Martin C, Matesanz P, et al. (2020) Adjunctive effect of systemic antimicrobials in periodontitis therapy: A systematic review and meta- analysis. J Clinical Periodontology 47(S22): 257-281.
-
Chambrone L, Wang L, Romanos G (2018) Antimicrobial photodynamic therapy for the treatment of periodontitis and peri-implantitis: An American Academy of Periodontology best evidence review. J Periodontol 89(7): 783-803.
-
Keck J, Viteri A, Schultz J, Fong R, Whitman C, et al. (2024) New Agents Are Coming, and So Is the Resistance. Antibiotics 13(7): 1-7.
-
Cosgarea R, Eick S, Jepsen S, Arweiler NB, Juncar R, et al. (2020) Microbiological and host-derived biomarker evaluation following non-surgical periodontal therapy with short-term administration of systemic antimicrobials: secondary outcomes of an RCT. Sci Rep 10(1): 16322.
-
Cosgarea R, Heumann C, Andronescu B, Rosu A, Arweiler NB, et al. (2022) Clinical, microbiological, and immunological effects of 3- or 7-day systemic antibiotics adjunctive to subgingival instrumentation in patients with aggressive (Stage III/IV Grade C) periodontitis: A randomized placebo-controlled clinical trial. J Clinical Periodontology 49(11): 1106-1120
-
Cruz D, Figueiredo L, Silva H, Retamal V, Feres M, et al. (2021) Metronidazole and amoxicillin for patients with periodontitis and diabetes mellitus: 5-year secondary analysis of a randomized controlled trial. J Periodontology 92(4): 479-487.
-
Faveri M, Souza J, Retamal V, Mestnik M, Figueiredo L, et al. (2023) Microbiological effects of amoxicillin plus metronidazole in the treatment of young patients with Stages III and IV periodontitis: A secondary analysis from a 1-year double-blinded placebo-controlled randomized clinical trial. J Periodontology 94(4): 498-508.
-
Hagenfeld D, Harks I, Eickholz P, Lorenz K, Kim S, et al. (2023) Long-term changes in the subgingival microbiota in patients with stage III–IV periodontitis treated by mechanical therapy and adjunctive systemic antibiotics: A secondary analysis of a randomized controlled trial. J Clinical Periodontol 50(8): 1101-1112.
-
Araujo C, Andere N, Castro S, Mathias S, Reis A (2019) Two different antibiotic protocols as adjuncts to one-stage full-mouth ultrasonic debridement to treat generalized aggressive periodontitis: A pilot randomized controlled clinical trial. J Periodontol 90(12): 1431-1440.
-
Cuk K, Povsic K, Milavec S, Seme K, Gaspersic R (2020) Influence of adjunctive azithromycin on microbiological and clinical outcomes in periodontitis patients: 6-month results of randomized controlled clinical trial. BMC Oral Health 20(1): 241.
-
Cuk K, Povsic K, Milavec S, Seme K, Gaspersic R (2021) Systemic azithromycin as an adjunct to scaling and root planing in patients with stage III/IV periodontitis: 12-month results of a randomized controlled clinical trial. Clin Oral Invest 25(10): 5997-6006.
-
Morales A, Contador R, Bravo J, Carvajal P, Silva N, et al. (2021) Clinical effects of probiotic or azithromycin as an adjunct to scaling and root planning in the treatment of stage III periodontitis: a pilot randomized controlled clinical trial. BMC Oral Health 21(1): 12.
-
Ilyes I, Rusu D, Rădulescu V, Vela O, Boariu MI, et al. (2023) A Placebo-Controlled Trial to Evaluate Two Locally Delivered Antibiotic Gels (Piperacillin Plus Tazobactam vs. Doxycycline) in Stage III–IV Periodontitis Patients. Medicina (Kaunas) 59(2): 303.
-
Rapone B, Ferrara E, Santacroce L, Topi S, Gnoni A, et al. (2022) The Gaseous Ozone Therapy as a Promising Antiseptic Adjuvant of Periodontal Treatment: A Randomized Controlled Clinical Trial. Int J Environ Res Public Health 19(2): 985.
-
Taalab MR, Mahmoud SA, Moslemany RME, Abdelaziz DM (2021) Intrapocket application of tea tree oil gel in the treatment of stage 2 periodontitis. BMC Oral Health 21(1): 239.
-
Teles FRF, Lynch MC, Patel M, Trresyap G, Martin L (2021) Bacterial resistance to minocycline after adjunctive minocycline microspheres during periodontal maintenance: A randomized clinical trial. Journal of Periodontology 92(9): 1222-1231.
-
Gonde NP, Rathod SR, Kolte AP (2022) Comparative evaluation of 1% melatonin gel in the treatment of intrabony defect: A randomized controlled clinical trial. Journal of Periodontology 93(12): 1878-1888.
-
Al-Momani MM (2021) Indocyanine-mediated antimicrobial photodynamic therapy promotes superior clinical effects in stage III and grade C chronic periodontitis among controlled and uncontrolled diabetes mellitus: A randomized controlled clinical trial. Photodiagnosis Photodyn Ther 35: 102379.
-
Costa FO, Lima RPE, Costa AM, Costa AA, Pereira GHM, et al. (2023) Adjunctive effects of photodynamic therapy using indocyanine green in residual pockets during periodontal maintenance therapy: A split-mouth randomized controlled trial. Journal of Periodontology 94(9): 1100-1111.
-
Harmouche L, Courval A, Mathieu A, Petit C, Huck O, et al. (2019) Impact of tooth-related factors on photodynamic therapy effectiveness during active periodontal therapy: A 6-months split-mouth randomized clinical trial. Photodiagnosis Photodyn Ther 27: 167-172.
-
Hill G, Dehn C, Hinze AV, Frentzen M, Meister J (2019) Indocyanine green-based adjunctive antimicrobial photodynamic therapy for treating chronic periodontitis: A randomized clinical trial. Photodiagnosis Photodyn Ther 26: 29-35.
-
Ivanaga CA, Miessi DMJ, Nuernberg MAA, Claudio MM, Garcia VG, et al. (2019) Antimicrobial photodynamic therapy (aPDT) with curcumin and LED, as an enhancement to scaling and root planing in the treatment of residual pockets in diabetic patients: A randomized and controlled split-mouth clinical trial. Photodiagnosis Photodyn Ther 27: 388-395.
-
Katsikanis F, Strakas D, Vouros I (2020) The application of antimicrobial photodynamic therapy (aPDT, 670 nm) and diode laser (940 nm) as adjunctive approach in the conventional cause-related treatment of chronic periodontal disease: a randomized controlled split- mouth clinical trial. Clin Oral Investig 24(5): 1821-1827.
-
Sukumar K, Tadepalli A, Parthasarathy H, Ponnaiyan D (2020) Evaluation of combined efficacy of photodynamic therapy using indocyanine green photosensitizer and non-surgical periodontal therapy on clinical and microbial parameters in the management of chronic periodontitis subjects: A randomized split-mouth design. Photodiagnosis Photodyn Ther 31: 101949.
-
Al-Khureif AA, Mohamed BA, Siddiqui AZ, Khan AA, Divakar DD (2020) Repeated application of photodynamic and antibiotic therapy as an adjunct to root surface debridement in patients with grade C and stage III or IV aggressive periodontitis. Photodiagnosis Photodyn Ther 29: 101610.
-
Cláudio MM, Nuernberg MAA, Rodrigues JVS, Belizário LCG, Batista JA, et al. (2021) Effects of multiple sessions of antimicrobial photodynamic therapy (aPDT) in the treatment of periodontitis in patients with uncompensated type 2 diabetes: A randomized controlled clinical study. Photodiagnosis Photodyn Ther 35: 102451.
-
Cláudio MM, Garcia VG, Freitas RM, Rodrigues JVS, Wainwright M, et al. (2024) Association of active oxygen- releasing gel and photodynamic therapy in the treatment of residual periodontal pockets in type 2 diabetic patients: A randomized controlled clinical study. Journal of Periodontology 95(4): 360-371.
-
Niazi FH, Noushad M, Tanvir SB, Ali S, Al-Khalifa KS, et al. (2020) Antimicrobial efficacy of indocyanine green-mediated photodynamic therapy compared with Salvadora persica gel application in the treatment of moderate and deep pockets in periodontitis. Photodiagnosis and Photodynamic Therapy 29: 101665.
-
Schär D, Ramseier CA, Eick S, Mettraux G, Salvi GE, et al. (2020) Transgingival photodynamic therapy (tg-aPDT) adjunctive to subgingival mechanical instrumentation in supportive periodontal therapy. A randomized controlled clinical study. Photodiagnosis Photodyn Ther 32: 101971.
-
Andere NMRB, Santos NCCD, Araújo CF, Paz HES, Shaddox LM, et al. (2022) Open flap debridement compared to repeated applications of photodynamic therapy in the treatment of residual pockets: A randomized clinical trial. Journal of Periodontolog 93(11): 1671-1681.
-
Annunziata M, Donnarumma G, Guida A, Nastri L, Persico G, et al. (2023) Clinical and microbiological efficacy of indocyanine green-based antimicrobial photodynamic therapy as an adjunct to non-surgical treatment of periodontitis: a randomized controlled clinical trial. Clin Oral Invest 27(5): 2385-2394.
-
Silva DNDA, Silva NTD, Sena IADA, Azevedo MLDS, Júnior FLDS, et al. (2020) efficacy of anti microbial photodynamic therapy with chloro-aluminum phthalocyanine on periodontal clinical parameters and salivary GSH and MDA levels in patients with periodontitis. Photodiagnosis and Photodynamic Therapy 31: 101843.
-
(2004) Position Paper: Systemic Antibiotics in Periodontics. Journal of Periodontology 75(11): 1553- 1565.
-
Dyke TEV, Bartold PM, Reynolds EC (2020) The Nexus Between Periodontal Inflammation and Dysbiosis. Front Immunol 11: 511.
-
Kim YC, Ko Y, Hong SD, Kim KY, Lee HY, et al. (2010) Presence of Porphyromonas gingivalis and plasma cell dominance in gingival tissues with periodontitis. Oral Diseases 16(4): 375-381.
-
Haffajee AD, Socransky SS (1994) Microbial etiological agents of destructive periodontal diseases. Periodontology 2000 5(1): 78-111.
-
Haffajee AD, Cugini MA, Tanner A, Pollack RP, Smith C, et al. (1998) Subgingival microbiota in healthy, well- maintained elder and periodontitis subjects. Journal of Clinical Periodontology 25(5): 346-353.
-
Holt SC, Ebersole JL (2005) Porphyromonas gingivalis, Treponema denticola, and Tannerella forsythia: the ‘red complex’, a prototype polybacterial pathogenic consortium in periodontitis. Periodontology 2000 38(1): 72-122.
-
Socransky SS, Haffajee AD, Cugini MA, Smith C, Kent RL (1998) Microbial complexes in subgingival plaque. Journal of Clinical Periodontology 25(2): 134-144.
-
Haubek D, Poulsen K, Westergaard J, Dahlèn G, Kilian M (1996) Highly toxic clone of Actinobacillus actinomycetemcomitans in geographically widespread cases of juvenile periodontitis in adolescents of African origin. J Clin Microbiol 34(6): 1576-1578.
-
Rams TE, Slots J (1996) Local delivery of antimicrobial agents in the periodontal pocket. Periodontology 2000 10(1): 139-159.
-
Walker CB, Godowski KC, Borden L, Lennon J, Nangó S, et al. (2000) The effects of sustained release doxycycline on the anaerobic flora and antibiotic-resistant patterns in subgingival plaque and saliva. J Periodontol 71(5): 768-774.
-
Cortellini P, Prato GP, Tonetti MS (1995) The Modified Papilla Preservation Technique. A New Surgical Approach for Interproximal Regenerative Procedures. Journal of Periodontology 66(4): 261-266.
-
Sanz M, Ceriello A, Buysschaert M, Chapple I, Demmer RT, et al. (2018) Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. Diabetes Research and Clinical Practice 137: 231-241.
-
Christiansen DL, Killeen AC, Ramer‐Tait A, Hattervig RL, Nawshad A, et al. (2023) Local simvastatin and inflammation during periodontal mini-flap wound healing: Exploratory results. Journal of Periodontology 94(4): 467-476.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells