Cervical Ectopic Pregnancy: Role of Imaging in Diagnosis and Management
Cervical pregnancy is rare form of ectopic pregnancy with implantation in the endocervical canal and accounts for less than 1% of all ectopic gestation. Ultrasonography has important role both in diagnosis and treatment. Early diagnosis in asymptomatic phase is possible especially in IVF pregnancies as these women are in constant clinical supervision. The transvaginal ultrasonography is safe and helpful in clinching diagnosis. Methotrexate (MTX) is the first line management in hemodynamically stable patient. In cases with presence of cardiac activity, MTX can be combined with ultrasound guided local injection of potassium chloride. Measures like intracervical vasopressin injection, ligation of cervico-vaginal division of uterine artery or use of inflated foley’s bulb can be used prior to conservative surgery like endocervical curettage to reduce chances of bleeding. Interventional radiological procedure like uterine artery embolization (UAE) is another option if available, before curettage to minimise bleeding.
Introduction
Ectopic gestation which contributes to 2% of all pregnancies is one of the substantial reasons of maternal mortality and morbidity during first trimester of pregnancy [1]. Cervical ectopic is an uncommon variety of ectopic gestation. Here, the embryo gets implanted in the endocervical canal below the level of internal os. There is high possibility of haemorrhagic complication necessitating emergency hysterectomy. Therefore early diagnosis and treatment is the key to prevent morbid situation. The modality of Ultrasonography has emerged as a very important tool in diagnosis as well as management of this life threatening condition. The rarity of this condition has limited evidence for optimal management coming mainly from case series and other observational studies.
Review of Literature
Cervical ectopic constitutes to less than 1% of all ectopic pregnancies [2, 3]. The incidence varies from one in 1000 to one in 95000 pregnancies [4, 5, 6]. It is seen more commonly among Assisted Reproductive Techniques (ART) conceptions accounting for 0.1% of all In-vitro Fertilisation (IVF) pregnancies and 3.7% of all IVF ectopic gestations [7]. There is implantation of embryo in the endocervical canal which may be due to damaged endocervical lining as a result of some operative procedures on uterus like dilatation and curettage (69%) and previous caesarean section (35%) [6, 7, 8]. Other risk factors are intrauterine adhesions, Asherman’s syndrome, intra-uterine devices, tumours and Mullerian anomalies. Recently it is being increasingly reported with ART [6, 9, 10, 11, 12, 13].
Vaginal bleeding is the most common presenting feature followed by lower abdominal pain [14]. They usually present in the first trimester at a mean age of seven to eight weeks [9, 15]. About 10% of the cases are asymptomatic and diagnosed on routine early pregnancy scan [15]. However, in some cases routine dating scan can diagnose this condition at an early asymptomatic stage [6, 12, 16]. A per speculum examination showing a bluish-purplish, hyperaemic, bulging oedematous and congested cervix is suggestive of cervical ectopic. However in few cases, the purple or bluish fetal tissue may be seen through the open external os. Rarely, cervical stromal invasion with trophoblastic tissue is seen as a cystic lesion on cervical lip. A Per vaginal examination shows a soft enlarged barrel shaped cervix which is disproportionately enlarged in comparison to uterus, referred to as an “hour- glass shaped uterus” with partially closed external os in most of the cases. However, in case of suspected cervical ectopic, a bimanual examination and especially digital examination of endocervical canal must not be done to avoid torrential haemorrhage.
Women with cervical ectopic pregnancy often present with intractable haemorrhage following period of amenorrhea not responding to conservative methods, often leading to hysterectomy. The actual diagnosis is revealed after hysterectomy after histopathological examination of the specimen. The author had a case which presented with haemorrhagic shock with torrential bleeding not responding to conservative methods and reported as a degenerated cervical fibroid on ultrasound report where patient ultimately underwent hysterectomy and the histopathology report revealed the presence of cervical pregnancy [17] (Figure 1).
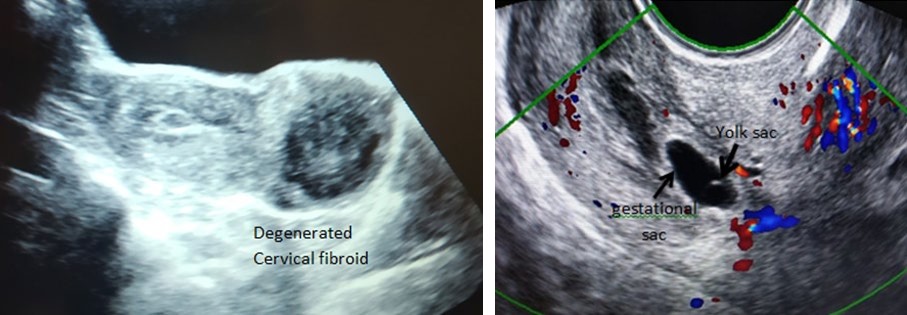
The report given was that of a degenerated cervical fibroid.Hysterectomy was done and histopathology revealed cervical ectopic gestation in this woman. There have been few reports of heterotopic pregnancy after Artifical reproductive techniques (ART) with one cervical and other intrauterine gestation [18, 19, 20, 21]. As the patients who conceive after ART [In-vitro fertilisation and Embryo transfer, (IVF-ET)] are under constant supervision so they can be detected in early asymptomatic stages. This early diagnosis can prevent life- threatening complications with a conservative approach. Use of superb diagnostic modalities, like transvaginal ultrasonography and serum beta-HCG determination, can help in early diagnosis and treatment.
Long back in 1969 and later 1978, cervical ectopic pregnancy was diagnosed using ultrasonography [22, 23]. In 1993 Sonographic diagnostic criteria was proposed by Timor-Tritsch, et al. [6]. Accordingly, the placental tissue, entire chorionic sac with live gestation should be below the level of internal os along with dilated and barrel shaped cervical canal. Still later in 1997, Ushakov suggested few more Ultrasonographic diagnostic points, as described earlier [6]. To summarise Ultrasonographic diagnostic criteria are
- Empty endometrial cavity with thickened endometrium
- Closed internal os.
- Presence of gestational sac or trophoblastic/placental tissue below the level of internal os. (Figure 2a,2b,2c,2d)
- Intact cervical canal between endometrium and gestational sac.
- Negative sliding sign. (Sliding sign-movement of the cervical contents with the pressure of the probe.)
- Increased peri-trophoblastic flow on color Doppler. (Figure 2a,2b)
- Gestational sac below the level of uterine artery
- Hourglass configuration of the uterus.
(a)
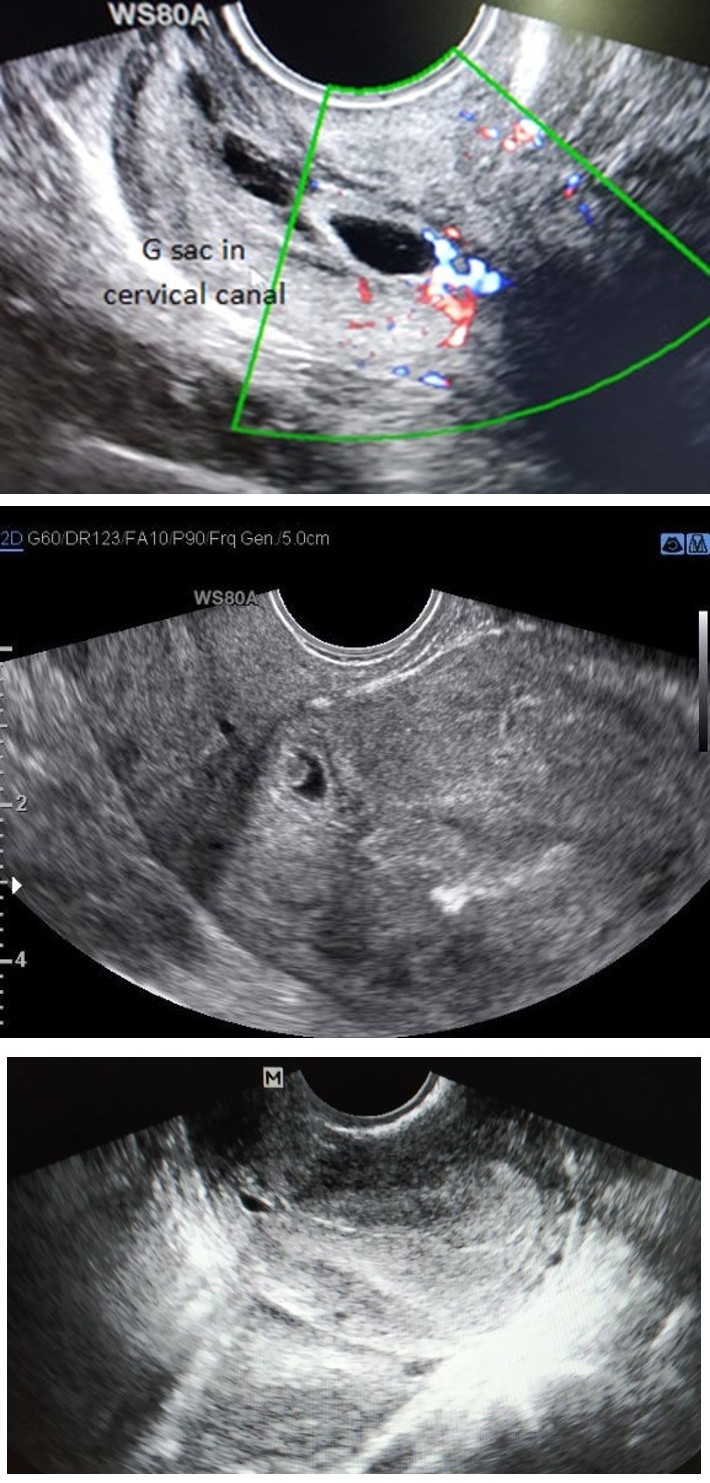
(b) Figure 2 ( a & b): Transvaginal ultrasonographic image of the patient with IVF pregnancy showing a well-defined gestational sac (corresponding to 5 week 1 day) in the cervical canal. It has a yolk sac but no embryonic pole. Sliding sign was negative. On color doppler, increase flow was seen.
Figure 2c: Transvaginal ultrasonographic image showing thick endometrium with gestational sac (corresponding to 4 weeks 6 days) in cervical canal.
Although all aetiologies of bleeding in early pregnancy can be included in differential diagnosis of cervical pregnancy however, most often the condition which presents in similar fashion and with similar clinical findings on examination is incomplete abortion. The condition can be differentiated by doing ultrasonographic examination. The sliding sign i.e., movement of the products of conception on gentle ultrasound probe movement will be positive in cervical abortion or ongoing abortion [24]. Moreover there will negative peri- sac flow on doppler. The sliding sign will remain negative in cervical pregnancy. When in doubt about the diagnosis and the patient is hemodynamically stable, ultrasonographic examination performed on next day will confirm the diagnosis of cervical pregnancy as the position of the cervical ectopic will remain static, while in incomplete abortion there will be a shift in the position of the sac. On ultrasound the above mentioned characteristic features point towards the diagnosis of cervical pregnancy, however there are some conditions which give similar picture radiographically. Cesarean scar pregnancy can also be included in the list of differential diagnosis if ultrasound shows the gestation sac in the anterior lower uterine segment along with empty uterine cavity and endocervical canal. But the proximity of sac to the scar site clinches the diagnosis (Figure 3).
A cervical pregnancy may give a picture similar to a degenerated cervical fibroid e.g. bulky or barrel shaped cervix and/or hour glass contour of uterus and cervix (Figure 1). The differentiating feature is a negative history of amenorrhea. The cervical pregnancy has been dealt as cervical fibroid due to its presentation, later on the final diagnosis revealed by histopathology [17]. Cervical cysts or Nabothian cysts may also give similar ultrasonographic picture [25]. The presence of yolk sac, embryonic pole, lack of decidual reaction and presence of color flow on doppler may distinguish the condition from cervical pregnancy. In rare cases, Magnetic Resonance Imaging (MRI) may be used to guide the management and in cases where the diagnosis is uncertain [26]. MRI characteristics are lobulated solid mass with heterogenous signal intensity of varying stages of haemorrhage along with enhancing, papillary, internal projection of products of conception in the cervix.
Management
As discussed above, diagnosis of cervical pregnancy is based on transvaginal ultrasound findings with positive pregnancy test with no intrauterine pregnancy [6]. However even the cases of heterotopic pregnancy with both cervical and intrauterine pregnancy has also been reported [18]. Histopathologic diagnosis can only be done if the patient undergoes hysterectomy [17]. The diagnostic criteria given by Rubin based on histologic criteria [27].
The modality of management depends on the clinical presentation and timely diagnosis, which can be conservative or radical [2]. The diagnosis and treatment of cervical pregnancy has changed radically over last two decades with widespread use of transvaginal ultrasonography and systemic and local Methotrexate (MTX) treatment. The conventional and traditional treatment of these patients had been hysterectomy, but reports about MTX use and other methodologies, have shown less aggressive and conservative ways to deal with these cases [28]. However taking into account the rare nature of this condition, there are no established criteria for medical versus surgical treatment for this condition as we have for tubal ectopic pregnancies. There are no specific management guidelines for this condition. The condition is known majorly by observational studies.
Medical Treatment
Methotrexate (MTX) remains the first line drug which can be given in hemodynamically stable women. But in case of hemodynamic instability, surgical treatment should be resorted to as we do in acute tubal ectopic patients [29]. In patients with continued bleeding after MTX therapy, there are options of uterine artery embolization (UAE) or Dilatation and endocervical curettage. Hysterectomy remains the option when all other measures fail.
Methotrexate Therapy
Evidence of methotrexate therapy use is limited to small case series sand reports [13, 30, 31]. Apart from hemodynamic instability, there are no optimal criteria to avoid medical therapy initiation in cervical pregnancy. The presence of fetal cardiac activity is a poor prognostic factor for MTX success in tubal pregnancy. But whether this is so for cervical ectopic as well, is not known. It is to be noted that fetal cardiac activity is present in 60% of cervical pregnancies in comparison to 10% of tubal ectopics [6]. Moreover whether to go for conservative surgical treatment of cervical pregnancy should be judged with caution as surgical option carries risk of haemorrhage and likely hysterectomy in contrast to surgical management of tubal ectopic. The success rate of MTX alone has been reported to be to the tune of 81.3%, while the success rate increased to 90% when MTX is combined with additional conservative methods [32]. According to Hung et al, failure of single MTX chemotherapy is likely if the gestational age is ≥9 weeks, fetal viability is documented, serum HCG titer is ≥10,000 milli-International Units/mL, or fetal CRL is greater than 10mm [33]. Different therapies in the form of ultrasound guided local or systemic, single or multidose systemic MTX, local MTX or Potassium chloride (KCl) or combination of these therapies have been described. The route of injection is either intra-amniotic or intra-fetal. The most commonly reported medications are MTX and KCl [9, 34, 35, 36]. Administration of intraamniotic prostaglandins F2α have also been described by Spitzer, et al. [37] and Vega, et al. [38] Jurkovic, et al. [23], in his review of 83 cases of cervical pregnancy concluded that the initial treatment should be medical, keeping the surgical treatment for chemotherapy treatment failures as patients who were initially treated with conservative surgery had increased risk of haemorrhage and requirement of hysterectomy than those treated medically. MTX can be used alone systemically or in combination with intra-gestational injection especially in cases where beta HCG value is very high [39, 40]. Especially cases with a beta HCG≥10,000 U, gestational age ≥9 weeks, presence of cardiac activity and crown rump length more than 10 mm were shown to have high medical treatment failure. Thus combination of treatment (systemic as well as local i.e. ultrasound guided injection) should be given in such cases.
Intra Gestational Sac Potassium Chloride (KCl): This procedure is done via transvaginal ultrasonographic guided Potassium Chloride (KCl) injection into the gestational sac and then fetal thorax using a 20 to 22 gauge needle guide attachment.1 to 5 ml of 20% KCl is injected till cardiac activity disappears. This again can be used alone or with systemic administration of MTX. Mefiprestone administered along with MTX to induce feticide has been reported by some authors [41, 42]. Mifepristone works as a competitive receptor antagonist at the progesterone receptor. It induces decidual autolysis indirectly, leading to trophoblast disruption. This leads to reduced production of HCG from syncytiotrophoblast. It further reduces production of progesterone by the corpus luteum. The combination of Mifepristone with MTX halts the embryonic development and hastens process of embryonic death, thus shortens the treatment time. The advantages of this combination are ease of oral administration, reduction in the dose and failure rate of MTX.
Minimally Invasive Surgical Procedures
The aim is excision of trophoblastic tissue and often is second line treatment if medical therapy fails. These include curettage, aspiration, hysteroscopic endocervical resection and cervical amputation [43] but this approach can cause haemorrhage necessitating additional methods to reduce bleeding during procedure.
Endocervical Curettage
There is a role of endocervical curettage if the patient is hemodynamically unstable at presentation due to haemorrhage or if there is persistent bleeding after the MTX therapy. There are several ways of decreasing the risk of bleeding at the time of curettage especially advocated for those who wish to preserve uterus. These have to be done before the curettage. These procedures are intracervical vasopressin injection, transvaginal ligation of cervico- vaginal branch of uterine artery or tamponade with foleys bulb and laparoscopic uterine artery occlusion [44, 45, 46]. Other methods which can be practised in case of persistent bleeding are bilateral uterine artery or bilateral internal iliac artery ligation. Even Uterine artery embolization (UAE) has been done successfully in these cases prior to curettage to reduce bleeding especially where patients are not desirous of future fertility. Wang, et al. [47] and Hu J, et al. [48] have used this approach and avoided hysterectomy in 16 cases and 19 cervical pregnancies respectively.
Uterine Artery Embolization (UAE)
UAE is taken as the next option after medical therapy and in cases with persistent bleeding after endocervical curettage, as its effects on future fertility and pregnancy outcome are unclear. Use of poly vinyl foam particles obstruct the feeding vessels for 2-6 weeks and allow development of collateral blood flow which starts within hours of the UAE. The endocervical curettage should be done as early as possible after this interventional radiological procedure for the maximum beneficial effect. Thus UAE is a one-stop solution for control of hemorrhage as well as evacuation of products of conception,moreover it improves therapeutic efficacy and leads to a shorter hospital stay and less laboratory and outpatient follow-up [48].
Hysterectomy
As these pregnancy have high potential for haemorrhage, this option is performed when all other measures fail or the patient doesn’t wish future fertility or the patient is hemodynamic unstable at the time of presentation [16, 17, 49]. However as it bears all risks and complications of the major surgery, MTX therapy remains the first line for hemodynamically stable pts.
Conclusion
Cervical pregnancy is rare form of ectopic pregnancy with implantation in the endocervical canal and accounts for less than 1% of all ectopic gestation. Ultrasonography plays an important role not only in diagnosis of the condition but also the management. The diagnosis is possible in asymptomatic phase. The transvaginal ultrasonography is safely done in these patients and help in clinching diagnosis Methotrexate is the first line management in hemodynamically stable patient. It can be given as local or systemically, alone or in combination with other modalities. In cases with presence of cardiac activity, MTX can be combined with ultrasound guided local injection of Potassium chloride. Interventional radiological procedure of uterine artery embolization (UAE) is another options, before curettage to minimise bleeding. Timely diagnosis and appropriate management using appropriate ultrasound modality can reduce the morbidity.
References
-
Agdi M, Tulandi T (2009) Surgical treatment of ectopic pregnancy. Best Pract Res Clin Obstet Gynaecol 23(4): 519-527.
-
Prameela RC, Dev SV (2016) Cervical ectopic pregnancy:10 year experience at tertiary care hospital and current literature review. Int J Reprod Contracept Obstet Gynecol 5(3): 734-742.
-
Bouyer J, Coste J, Fernandez H, Pouly JL, Job-Spira (2002) Sites of ectopic pregnancy: a 10 year population-based study of 1800 cases. Human Reproduction 17(12): 3224-3230.
-
Celik C, Bala A, Acar A, Gezgine K, Akyurek C (2003) Methotrexate for cervical pregnancy. A case report. J Reprod Med 48(2): 130-132.
-
Cepni I, Ocal P, Erkan S, Burcak E (2004) Conservative treatment of cervical ectopic pregnancy with transvaginal ultrasound guided aspiration and single- dose methotrexate. Fertil Steril 81(4): 1130-1132.
-
Ushakov FB, Elchalal U, Aceman PJ, et al. (1997) Cervical pregnancy: Past and future.Obstet Gynecol Surv 52(1): 45-59.
-
Karande VC, Flood JT, Heard N (1991) Analysis of ectopic pregnancies resulting from in-vitro fertilisation and embryo transfer. Hum Reprod 6(3): 446-449.
-
Vela G, Tulandi T (2007) Cervical pregnancy:the importance of early diagnosis and treatment. J Minim Invasive Gynecol 14(4): 481-484.
-
Ferrara L, Belogovkin V, Gandhi M, Litton C, Jacobs A, et al. (2007) Successful management of a consecutive cervical preganancy by sonographically guided transvaginal local injection: case report and review of literature. J Ultrasound Md 26(7): 959-965.
-
Usha Verma (2012) Assisted Reproduction techniques. Challenges and management options. Cervical ectopic pregnancy after IVF, Chap 91, Wiley Blackwell, pp: 391- 395.
-
Corrales Y (2012) Embarazo ectopico bilateral presentation de un caso Y revision de la literature. Medisur 10: 73-79.
-
Tejero C, Ortega M, Royo B, Pilar A, Lapresta M, et al. (2010) Gestacion ectopica cervical tratada mediante puncion ecoguiada intrasacular de methotrexate. Rev Chil Obstet Ginecol 75(5): 325-328.
-
Jeng CJ, Ko ML, Shen J (2007) Transvaginal ultrasound- guided treatment of cervical pregnancy. Obstetrics and Gynecology 109(5): 1076-1082.
-
Alalade AO, Smith FJE, Kendall CE, Odejinmi F (2017) Evidence-based management of non-tubal ectopic pregnancies. J Obstet Gynaecol 37(8): 982-991.
-
Murji A, Garbedian K, Thomas J, Cruickshank B (2015) Conservative Management of Cervical Ectopic Pregnancy. JOGC 37(11): 1016-1020.
-
Genc M, Genik B, Kurt S (2014) A case of cervical ectopic pregnany: Management and review of the literature. American Journal of Medical Case reports 2(1): 9-15.
-
Pandey D, Tripathi BN, Pandey S (2013) Cervical ectopic pregnancy presenting as cervical fibroid. J Basic Clin Reprod Sci 2: 132-134.
-
Tsakos E, Tsagias N, Dafopoulos K (2015) Suggested Method for the Management of Heterotopic Cervical Pregnancy Leading to Term Delivery of the Intrauterine Pregnancy: Case Report and Literature Review. J Minim Invasive Gynecol 22(5): 896-901.
-
Cho JH, Kwon H, Lee KW, Han WB (2007) Cervical heterotopic pregnancy after assisted reproductive technology successfully treated with only simple embryo aspiration: a case report. J Reprod Med 52(3): 250-252.
-
Prorocic M, Vasiljevic M (2007) Treatment of heterotopic cervical pregnancy after in vitro fertilization-embryo transfer by using transvaginal ultrasound-guided aspiration and instillation of hypertonic solution of sodium chloride. Fertil Steril 88(4): 969.e3-969.e5.
-
Chen D, Kligman I, Rosenwaks Z (2001) Heterotopic cervical pregnancy successfully treated with transvaginal ultrasound-guided aspiration and cervical- stay sutures. Fertil Steril 75(5): 1030-1033.
-
Raskin MM (1978) Diagnosis of cervical pregnancy by ultrasound. A case report. Am J Obstet Gynecol 130(2): 234-235.
-
Timor-Tritschl E, Monteagurdo A, Mandeville EO (1994) Successful management of viable cervical pregnancy by local injection of Methotrexate guided by transvaginal ultrasonography. Am J Obstet Gynecol 170(3): 737-739.
-
Jurkovic D, Hacket E, Campbell S (1996) Diagnosis and treatment of early cervical pregnancy: a review and a report of two cases treated conservatively. Ultrasound Obstet Gynecol 8(6): 373-380.
-
Dibble EH, Lourenco AP (2016) Imaging Unusual Pregnancy Implantations: Rare Ectopic Pregnancies and More. AJR 207(6): 1380-1392.
-
Jung SE, Byun JY, Lee JM, et al. (2001) Characteristic MR findings of cervical pregnancy. J Magn Reson Imaging 13(6): 918.
-
Rubin IC (1911) Cervical pregncncy. Surg Gynecol Obstet 13: 625.
-
Marston, Dotters D, Katz V (1996) Methotrexate and angiographic embolization for conservative treatment of cervical pregnancy. South Med J 89(2): 246-248.
-
American College of Obstetricians and Gynecologists (2018) Medical management of tubal pregnancy. ACOG Practice Bulletin 193. Int J Gynaecol Obstet 131(3): e91-e103.
-
Mesogitis S, Pilalis A, Daskalakis G (2005) Management of early viable cervical preganancy. BJOG 112(4): 409- 411.
-
Kirk E, Condous G, Haider Z , Syed A, Ojha K, et al. (2006) The conservative management of cervical ectopic pregnancies. Ultrasound Obstet Gynecol 27(4): 430-437.
-
Vela G, Tulandi T (2007) Cervical pregnancy: the importance of early diagnosis and treatment. J Minim Invasive Gynecol 14(4): 481-484.
-
Hung TH, Shau WY, Hsieh TT, Hsu JJ, Soong YK, et al. (1998) Prognostic factors for an unsatisfactory primary methotrexate treatment of cervical pregnancy: a quantitative review. Hum Reprod 13(9): 2636-2642.
-
Majumdar A, Gupta SM, Chawla D (2009) Successful management of post invitro fertilization cervical heterotropic pregnancy. J Hum Reprod Sci 2(1): 45-46.
-
Verma U, Goharkhay N (2009) Conservative management of cervical ectopic pregnancy. Fertil Steril 91(3): 671-
-
Sijanovic S, Vidosavljevic D, Tapolovec Z (2014) Management of cervical ectopic pregnancy after unsuccessful methotrexate treatment. Iran J Reprod Med 12(4): 285-288.
-
Spitzer D, Steiner H, Graf A, Zajc M, Staudach A (1997) Conservative treatment of cervical pregnancy by curettage and local prostaglandin injection. Hum Reprod 12(4): 860-866.
-
De La Vega GA, Avery C, Nemiroff R, Marchiano D (2007) Treatment of early cervical pregnancy with cerclage, carboprost, curettage, and balloon tamponade. Obstet Gynecol 109(2): 505-507.
-
Ibghi W, Simon E, Castillon (1997) Medical treatment for cervical pregnancy with methotrexate on-site exclusively. J Gynecol Obstet Biol Reprod 26: 525-528.
-
Pretzsch G, Einenkel J, Baier D, Horn LC, Alexander H (1997) Cervical pregnancy: a case report and review of the literature. Zentralbl Gynakol 119(1): 25-34.
-
Shrestha E, Yang Y, Li X, Zhang Y (2011) Successful conservative management with methotrexate and mifepristone of cervical pregnancy. J Biomed Res 25(1): 71-73.
-
Pathak S, Khalil H, Fastovetsv G (2008) Combined Medical - Surgical Management of Cervical Ectopic Pregnancy - A Case Report. Ultrasound 16(1): 18-20.
-
Parente JT, Chau Su Levy J, Legatt E (1983) Cervical pregnancy analysis. A review and report of five cases. Obstet Gynecol 62(1): 79-82.
-
Kung FT, Lin H, Hsu TY, et al. (2004) Differential diagnosis of suspected cervical pregnancy and conservative treatment with the combination of laparoscopy-assisted uterine artery ligation and hysteroscopic endocervical resection. Fertil Steril 81(6): 1642-1649.
-
Fylstra DL (2014) Cervical pregnancy:13 cases treated with suction curettage and balloon tamponade. Am J Obstet Gynecol 210(6): 581.e1: 581-e5.
-
Hong-Seok Choi, Na-Young Kim, Yong-Il Ji (2015) Laparoscopic uterine artery occlusion before cervical curettage in cervical ectopic pregnancy: Safe and effective for preventing massive bleeding. Obstet Gynecol Sci 58(5): 431-434.
-
Wang Y, Xu B, Dai S, Hang Y, Duan Y, et al. (2011) An efficient conservative treatment modality for cervical pregnancy: angiographic uterine artery embolization followed by immediate curettage. Am J Obstet Gynecol 204(1):31.e1-31.e7.
-
Hu J, Tao X, Yin L, Shi Y (2016) Successful conservative treatment of cervical pregnancy with uterine artery embolization followed by curettage: a report of 19 cases. BJOG 123(S3): S97-S102.
-
Tomov S, Gortchev G, Tantcev L (2015) Cervical ectopic pregnancy with massive bleeding: a case report. International Journal of Surgery and Medicine 1(1): 22- 25.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’