Torsion of Giant (3 Kg) Non - Gravid Myomatous Uterus with Congenital Cervical Agenesis with Absence of Right Side Ovary and Fallopian Tube: Extremely Rare Case
Uterine torsion is defined as rotation of the uterus around its longitudinal access by more than 45 degrees. Uterine torsion is supposed to be a rare entity with a combination of diagnostic as well as management challenges. The uterine torsion is mostly associated with uterine anomalies and torsion is common in a gravid urus rather than a non-gravid uterus. Till date, less than fifty such cases have been reported. Here we report a case report of gynaecology uterine torsion over its axis, which was an incidental finding and was managed with great surgical expertise and during the times of COVID pandemic.
Introduction
Uterine torsion encountered in a non-gravid uterus is extremely rare [1, 2]. A literature search reveals less than 50 reported cases of uterine torsion in a non-gravid uterus. Uterine torsion is a rare entity. Among the pelvic masses, ovarian torsions are commonly encountered in a clinical practice. Any torsion is associated with ischemic and gangrenous changes presenting as acute abdomen and is characterized by decreased blood flow on doppler studies. However, uterine torsion do no present in the same way and are often diagnosed intra operatively. It is considered as a “once in a lifetime” opportunity for the gynecologist. Hence we present this case for its rarity.
Case Report
A 43 years old, unmarried, nulligravida, diagnosed case of pott’s spine operated for thoracic corpectomy with lower limb paralysis with bed sores, referred from neurosurgery department in view of uterine fibroid.
Patient gave history of tubercular meningitis? Tuberculosis cervical spine 22 years ago for which she was admitted at hospital and took treatment for 3 years for MDR-TB. Post-meningitis, patient had bilateral lower limb paralysis for a year, after which she regained bilateral lower limb power. Three years ago, patient again developed weakness in lower limbs and had fever spikes .She was diagnosis of tubercular spondylodiscitis of D8 and D9 and underwent thoracic corpectomy.
Post operatively, patient had persistent abdominal pain for which Computed Tomography was advised 6/9/19 Computed Tomography was suggestive of intramural uterine fibroid with cystic changes measuring 15.5 x 20.3 x 22.5 cm arising from posterior uterine wall.
(12/3/2020) Ultrasound was suggestive of Bilateral polycystic kidney with liver cysts Tumor markers were sent - CA 125-18.4; AFP 13.4; BHCG
-2.61; LDH -231; CEA - 0.94
Patient lost follow up due to the COVID -19 pandemic and presented to Grant Government Medical College, Mumbai with complaints of pain in abdomen and weakness of lower limbs.
She had attained menopause 2 years back On clinical examination, general condition was fair, afebrile.
Pulse: 90/min; blood pressure: 120/80 mmhg, SpO2: 99% at RA, on systemic examination, Cardiovascular and respiratory examination was normal. On per abdomen examination solid mass of 30 weeks of gestation , occupying umbilicus, left hypogastric, left lumbar region, regular margins, mobile, firm in consistency. Superficial skin was normal.
On local examination, -3x2 x3 cm bed sore seen in right greater trochanter region -3 x5 x 0/5 cm bed sore seen bilateral over natal cleft region with heavy granulation seen. On per rectal examination: rectal mucosa free; lower border of pelvic mass felt. Margins were regular
12/2/2021: Covid 19 swabs RT PCR reported negative. 12/2/2021: gene xpert: MTB not detected.
14/2/2021: plastic surgery reference done i/v/o bed sores. Advised wound culture sensitivity and frequent change of positions jellonet dressing.
23/2/2021 computed tomography abdomen + pelvis was suggestive of multiple hepatic and bilateral renal cysts, suggestive of autosomal dominant polycystic kidney disease mild hepatomegaly (18 cm), large hypodense solid lesion of 11x13x14cm arising from the left ovary with torsion of the ovary? dysgerminoma.
Fitness for surgery was obtained from neurosurgery, nephrology and plastic surgery.
Patient underwent: exploratory laparotomy with? mixed mesodermal uterine ovarian mass excision with left salphingectomy with omentectomy under General anesthesia after pre anesthetic fitness.
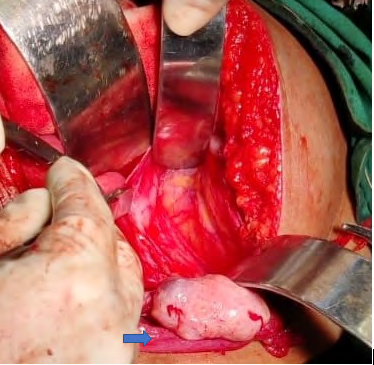
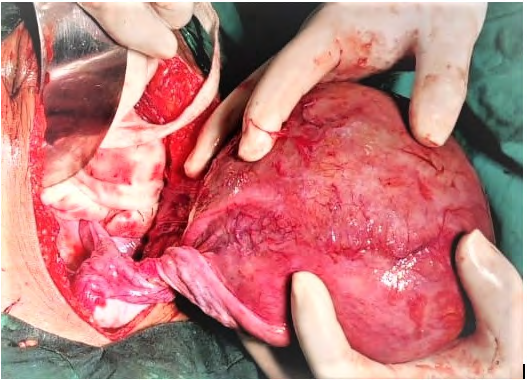
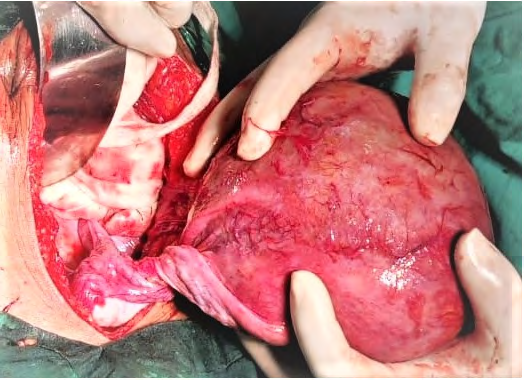
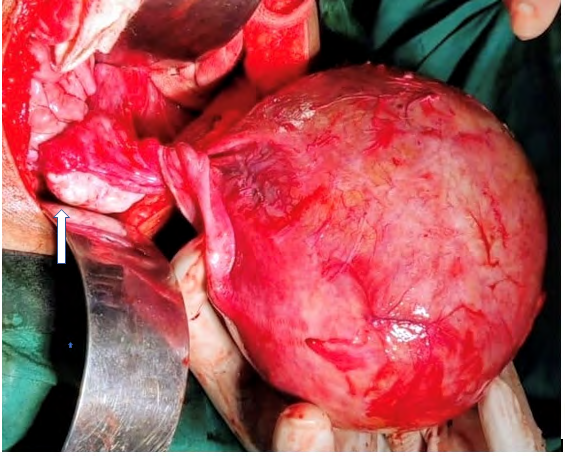
in situ-large mass of 30cm*25cm*20cm extending from the lower abdomen and reaching upto the xyphisternum superiorly with fullness of flanks with solid consistency, the mass has hemorrhagic surface, dilated vessels seen on surface of mass. Mass was adherent to left anterior abdominal wall, blood supply from vessels extending from left anterior abdominal wall, all the ashesions separated systematically with achieving haemostasis.
Anteriorly, mass was adherent to large intestine, posteriorly was reaching upto iliac vessels using harmonic scalpel and bipolar cautery, all the bleeders were systematically cauterized. Anterior abdominal wall, all the ashesions separated systematically with achieving haemostasis. Fine dissection and done with hemostatic control and mass was delivered out .In situ we have found that The mass has undergone with the axial rotation of 360 degree with 4-5 rotating rings seen at the pedicle. Pedicle of the mass contains major vessels, part of fallopian tube, infundibulopelvic ligament. Uterus was not seen and must have developed in tumor remnants of ovarian tissue. The cervix was absent and the Right sided Fallopian tube and Right sided ovary was absent congenitally.
Ureters were pulled up, ureteric dissection done and ureter pulled down. bilateral ureters traced in their course completely-> intact and not injured. Urinary bladder was pulled up with dilated vessels over the surface.
10/3/2021: Histopathological report suggestive of proliferative phase endometrium with leiomyoma; fallopian tube stump unremarkable and left fallopian tube had normal histology. Patient was discharged later on.
Discussion
Uterine torsion is defined as the rotation of the uterus more than 45 degrees on its long axis, and mostly reported at the junction between the cervix and the uterine corpus [3].
Rotation of the gravid uterus around 45 degrees is physiological and is due to the recto-sigmoid colon on the posteriorlateral aspect of the uterus [4]. Dextro – rotation is more commonly encountered (around two thirds of the patient) rather than the levo-rotation reported in the rest [5, 6, 7]. The pathogenesis is attributable to the wakening of the uterine supports and parametrium following the post- menopausal status [8, 9].
Torsion is usually secondary to the uterine pathology like uterine leiomyoma, gravid state or the uterine anomalies.
Piot, et al. has reported the most common factor associated with uterine torsion to be leiomyoma [10].
The symptoms with which the patients present include asymptomatic presentation, very rarely pain in abdomen and fetal malpresentation in a gravid uterus. Till date around 200 cases have been reported. The failure to be diagnosed on imaging modality is a major challenge.
Intra operatively, the diagnosis can be confirmed by palpating the two round ligaments. If the symmetry is distorted then the diagnosis of uterine torsion is confirmed. In our case it was complete 360 degrees torsion.
The differential diagnosis of ovarian torsion, broad ligament fibroid should be kept in mind. Broad ligament fibroids of huge size might cause displacement and distorsion of anatomy to make the case more difficult [11].
The ovarian torsion with benign masses like teratoma may obscure the peritoneal space and distort the abdominal anatomy mimicking uterine torsion. Clinical diagnosis may be difficult and hence the possibility of the same should be borne in mind [12].
The congenital absence of cervix a very rare disorder with its incidence being only 1 in 80,000 [13]. It is considered as 1B classification of Müllerian anomaly [14, 15].
The surgical importance of round ligament is well establishes in such cases as it helps in delineating the pelvis anatomical structures precisely [16]. Uterine torsion encountered in a non-gravid uterus is extremely rare [1, 2]. A literature search reveals less than 50 reported cases of uterine torsion in a non-gravid uterus.
The patient was managed with a high surgical safety index and a great surgical expertise. The patient and relatives were satisfied with the management and gave the consent for publication of this case report.
Conclusion
This case is reported for its rarity and its diagnostic and management challenges that were associated. Diagnosing a malformed uterine torsion is difficult on imaging modalities as well as intra operatively. Its a very rare entity but sometime can become Emergency with torsion and its consequances. The treatment is always surgical and it depend on the degree of torsion and damage occurred. Need of Fertility sparing surgery to be considered in young woman who wanted to preserve uterus for the fertility. if older women then go for the Hysterectomy. Best clinical Acumen to Diagnose and a great surgical expertise required to treat the condition.
Conflict of Interest
The author declares that they have no conflict of interest regarding the publication of this case report.
Funding
No funding from an external source supported the publication of this case report.
Patient Consent
Obtained
Acknowledgments
Dr Shreya Chinchoriya, Senior Resident
References
-
Luk SY, Leung JLY, Cheung ML, So S, Fung SH, et al. (2010) Torsion of a Nongravid Myomatous Uterus: Radiological Features and Literature Review. Hong Kong Med J 16(4): 304–306.
-
Grover S, Sharma Y, Mittal S (2009) Uterine Torsion: A Missed Diagnosis in Young Girls? Journal of Pediatric and Adolescent Gynecology 22(1): e5–8.
-
Moores KL, Wood MG, Foon RP (2014) A rare obstetric emergency: acute uterine torsion in a 32-week pregnancy. BMJ Case Rep 2014: bcr2013202974.
-
Ahmed FU, Ambreen A, Zubair S, Kiran N (2016) Torsion of a Term Uterus. J Coll Physicians Surg Pak 26(6): S50- 51.
-
Dua A, Fishwick K, Deverashetty B (2005) Uterine torsion in pregnancy: a review. Int J Obstet. Gynecol 6(1): 1-3.
-
Corr J (1943) Axial torsion of the gravid uterus in two successive pregnancies. Ameican Journal Obstetrics and Gynecology 46(5): 749-752.
-
Collinet P, Narducci F, Stien L (2001) Torsion of a nongravid uterus: an unexpected complication of an ovarian cyst. Eur J Obstet Gynecol Reprod Biol 98(2): 256-257.
-
Havaldar N, Ashok K (2014) Torsion of non-gravid uterus with ovarian cyst - an extremely rare case. Pan. Afr. Med. J 18: 95.
-
Sharma D, Usha M (2013) Torsion of a non-gravid uterus: a rare cause of acute abdomen. Int J Reprod Contracept Obstet Gynecol 2(2): 234-236.
-
Piot D, Gluck M, Oxorn H (1973) Torsion of the gravid uterus. Can. Med. Assoc. J 109(10): 1010-1011.
-
Katke RD (2017) Huge (9 Kg) broad ligament fibroid mimicking sarcoma of uterus: A case report and review of literature. Journal of mid-life health 8(4): 191-193.
-
RD. Torsion of huge cystic teratoma of ovary with multiple fibroids uterus: a case report and review of literature. Int J Reprod Contracept Obstet Gynecol 3(3): 793-795.
-
Suganuma N, Furuhashi M, Moriwaki T, Tsukahara S, Ando T, et al. (2002) Management of missed abortion in a patient with congenital cervical atresia. Fertil Steril 77(5): 1071-1073
-
Saravelos SH, Cocksedge KA, Chiu Li T (2008) Prevalence and diagnosis of congenital uterine anomalies in women with reproductive failure: a critical appraisal. Hum Reprod Update 14(5): 415-429.
-
Azinar AD, Annas JY, Primariawan RY, Hardianto G (1999) Treatment of cervical agenesis with minimally invasive therapy: Case report. Gynecol Minim Invasive Ther 6(4): 202-204.
-
Sheth SS, Sonkawde R (1999) Surgical importance of round ligament. J Gynecol Surg 15(3): 163-167.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’