The Neoplastic Nonage-Dysgerminoma Ovary
Dysgerminoma is a commonly discerned, malignant, primitive germ cell ovarian neoplasm devoid of specific differentiation. Dysgerminoma may frequently emerge as a gestational neoplasm. Exceptionally, dysgerminoma may be associated with gonadal dysgenesis or anomalies of chromosome Y. Dysgerminoma is a low grade neoplasm which occurs in young subjects wherein surgical intervention is an optimal treatment strategy, thus tumefaction exemplifies a favorable outcome.
Editorial
Dysgerminoma is a commonly discerned, malignant, primitive germ cell ovarian neoplasm devoid of specific differentiation. Dysgerminoma may frequently emerge as a gestational neoplasm. Exceptionally, dysgerminoma may be associated with gonadal dysgenesis or anomalies of chromosome Y. Dysgerminoma is a low grade neoplasm which occurs in young subjects wherein surgical intervention is an optimal treatment strategy, thus tumefaction exemplifies a favorable outcome. Ovarian tumefaction commonly arises from primordial germ cells. Alternatively, tumour may arise from gonadoblastoma. Bilateral ovaries can be incriminated wherein contralateral ovary exhibits microscopic deposits. Extra-ovarian tumour dissemination may be observed. Exceptionally, tumefaction is confined to extra-ovarian sites as abdominal cavity, fallopian tube or uterus [1, 2]. Majority (~80%) of dysgerminomas exhibit isochromosome 12p. KIT genetic mutations within exon 17 codon 816 or KIT amplification is associated with advanced disease at initial representation. Majority of neoplasms at preliminary tumour discernment are stage I lesions. Tumour can represent as ‘pure’ form or may configure a component of malignant, mixed germ cell tumour. Tumefaction is frequent in children and young females [1, 2]. Clinically, abdominal pain or distension is observed. Oestrogenic manifestations can be infrequently discerned. Fallopian tubes appear attenuated [1, 2]. Upon gross examination, tumefaction is solid, lobulated and > 10 centimetre magnitude. Cut surface is fleshy, tan-white with focal haemorrhage, necrosis or cystic degeneration. Focal calcification may indicate a component of gonadoblastoma [1, 2]. Frozen section appears suggestive of a high-grade, malignant, germ cell tumour, malignant epithelioid neoplasm, and large cell lymphoma with enlarged, neoplastic nuclei and infiltrating, reactive lymphocytes, small cell carcinoma with paraneoplastic hypercalcemia constituted of tumour cells with scanty cytoplasm or an admixed small and non-small cell carcinoma. Tumour cells with clear cytoplasm or distinct cellular membranes may be unappreciable.
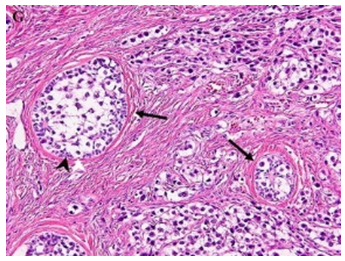
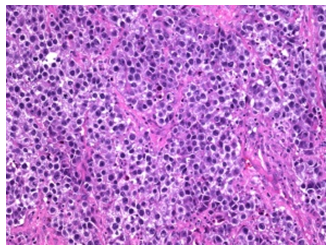
Dysgerminoma exhibits tumour cells incorporated with moderately abundant cytoplasm, ‘squared-off’ nuclei and intervening fibrous septa [1, 2]. Cytological evaluation exhibits a uniform population of dis-cohesive, medium or enlarged tumour cells with scanty, eosinophilic cytoplasm, centric, hyperchromatic, spherical, elliptical or angulated, ‘squared- off’ nuclei, vesicular, finely granular or coarse nuclear chromatin and prominent, singular or multiple nucleoli [1, 2]. Upon microscopy, characteristic tumour cell nests composed of enlarged, uniform, polygonal cells incorporated with clear or eosinophilic cytoplasm and distinct cellular membranes are observed, configuring the ‘alveolar pattern ’ [1, 2]. Tumefaction is composed of sheets or nests of uniform cells imbued with clear to eosinophilic cytoplasm, distinct cellular membrane, and spherical nuclei with angulated, ‘squared-off’ edges and intervening fibrous tissue septa infiltrated by cytotoxic T cells and epithelioid histiocytes. Additionally, neoplasm may configure sheets, cords, macro-nodules, insular tumour pattern, micro-cysts, tubules, pseudo-glandular spaces or trabeculae (Table 1). A pseudo-papillary or macro-follicular tumour articulation is exceptional [1, 2]. Tumefaction is traversed by fibrous septa infiltrated by cytotoxic T lymphocytes and epithelioid histiocytes wherein inflammatory exudate may expand into tumour parenchyma. Additionally, plasma cells, eosinophils, Langhans giant cells, syncytiotrophoblasts, non-caseating granulomas or definitive lymphoid follicles with germinal centres may be observed. Mitotic activity is significant [1, 2]. Circumscribing stroma is loose and delicate although hyalinised, myxoid or luteinized stromal configuration may be enunciated [1, 2]. Infrequently, singular or aggregates of syncytiotrophoblastic cells devoid of admixed cytotrophoblastic tissue can be discerned, instances where choriocarcinoma requires an exclusion [1, 2]. Extensive, focal haemorrhage, necrosis and dystrophic calcification may be exemplified. Expansive dystrophic calcification in the absence of necrosis requires exclusion of a gonadoblastoma (Figure 1 & 2).
| Stage | Extent of Disease |
|---|---|
| Stage I | Tumour excised with intact capsule, malignant cells absent in peritoneal cytology, peritoneal sur- faces, omentum & lymph nodes <1cm |
| Stage II | Tumour excised with pre-operative biopsy, disrupted capsule in situ with capsular penetration, tumour>10cm laproscopically excised, tumour morcellated, tumour cells absent in peritoneal cytol- ogy, peritoneal surface, omentum, lymph nodes |
| Stage III | Lymph nodes ≥2cm,tumour or specimen excised with gross residual, tumour cells in peritoneal fluid, lymph nodes or peritoneal or liver surface implants |
| Stage IV | Distant metastasis to liver, lung, brain, bone or extra-peritoneal viscera, tumour cells in pleural fluid |
| Stage III- (stage Ior II along with) | Lack of peritoneal cytology, lymph node biopsy>1cm, abnormal peritoneum, omentum or delayed staging at second surgery |
Table 1: Staging of Ovarian Germ Cell Tumour (Children Oncology Group).
Tumour cells are immune reactive to SALL4, OCT3/4, D2-40, CD117, NANOG or PLAP. Focal immune reactivity to keratin, CAM5.2, AE1/AE3 or CK7 is observed [3, 4]. Immune reactivity to HCG, inhibin, glypican or CK7 is associated with discernible syncytiotrophoblastic giant cells [3, 4]. Dysgerminoma is immune non-reactive to EMA, CEA, HCG, CD30, glypican3, AFP or SOX2 [3, 4]. Dysgerminoma requires segregation from mixed germ cell tumours as embryonal carcinoma, yolk sac tumour, clear cell carcinoma, lymphoma or hypercalcaemic variant of small cell carcinoma [3, 4]. Dysgerminoma can be appropriately discerned with comprehensive clinical history, age of incriminated subject, elevated LDH, PLAP, minimally enhanced β-HCG with syncytiotroblastic giant cells in the absence of cytotrophoblastic tissue, paraneoplastic hypercalcemia and histological assessment of neoplasm [3, 4]. Ultrasonography exhibits an enlarged, solid, lobulated, extensively vascular, adnexal tumefaction with an irregular, intrinsic echogenicity. Enhancing fibrous tissue septa are observed. Necrosis and haemorrhage appear as focal cystic alterations. Calcification can manifest a speckled pattern [3, 4]. Dysgerminoma is a radiosensitive tumefaction [3, 4]. Cogent treatment with cisplatin-based chemotherapy is associated with superior prognostic outcome wherein overall survival is > 90%. On account of KIT genomic mutation implicating exon 17, aforesaid neoplasm is therapeutically unresponsive to KIT receptor inhibitors [3, 4]. Surgical intervention with fertility-sparing surgery in ‘pure’ ovarian dysgerminoma with additional surgical intervention adopted for staging procedures along with retroperitoneal lymph node dissection employed to determine stage IA neoplasms which are exempt from adjuvant chemotherapy, is a recommended strategy [3, 4]. Tumour reoccurrence is minimal [5, 6].
References
-
Hara N, Suwanai H, Abe H, Yakou F, Ishikawa T, et al. (2022) Hypercalcemia associated with dysgerminoma and elevation of calcitriol: A case report and review of the literature. SAGE Open Med Case Rep 10: 2050313X211068562.
-
Raafey MA, Abdulwaasey M, Fatima SS, Uddin Z, Tariq MU (2020) Bilateral Gonadoblastoma with Dysgerminoma in a Phenotypically Normal Female with 46XX Karyotype: Report of a Rare Case and Literature Review. Cureus 12(7): e8990.
-
Roth LM, Davis MM, Czernobilsky B (2019) “Classic and “Dissecting” Gonadoblastoma in a Phenotypic Girl with a 46, XX Peripheral Karyotype and No Evidence of a Disorder of Sex Development. Int J Gynecol Pathol 38(6): 581-587.
-
Alam S, Boro H, Goyal A, Khadgawat R (2020) 46, XY complete gonadal dysgenesis with pubertal virilisation due to dysgerminoma/gonadoblastoma. BMJ Case Rep 13(7): e235501.
-
Image 1 Courtesy: Springer link.
-
Image 2 Courtesy.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’