APLA Syndrome in Pregnancy and its Outcome: A Case Report
Antiphospholipid antibody syndrome is a heterogenous autoantibody mediated acquired thrombophilia, which is associated with severe life threatening complications during pregnancy and most important treatable cause of recurrent pregnancy loss. It was described in 1980s by E Nigel Harris and Aziz Gharavi. It is also called as Hughes syndrome. Clinician should have high index of suspicion of APLA in patient with history of recurrent abortions, Intra uterine death with unexplained cause. We are presenting a case of 27yr old G2A1 with 38 wks. of POG with history of pulmonary thromboembolism and pulmonary hypertension and deep vein thrombosis 2 years ago, she was diagnosed with APLA syndrome. Patient was followed up to term and she was asymptomatic throughout the pregnancy. She had full term normal delivery. Both mother and baby were stable and healthy. She was asymptomatic in her postpartum period.
Introduction
Antiphospholipid Syndrome (APS) is an autoimmune disorder of hypercoagulable state that is marked by the presence of antibodies that attack phospholipid-binding proteins, characterized by vascular thrombosis and pregnancy complications especially recurrent spontaneous miscarriages and, less frequently, maternal thrombosis (Table 1). A modified Sapporo criterion is used to diagnose APLA syndrome [1, 2, 3, 4].
| Clinical criteria | Lab criteria |
|---|---|
| 1. ≥1unexplained deaths of morphologically normal foetus ≥ 10wks | 1. Lupus Anticoagulant |
| 2. Severe preeclampsia& delivery ≤34wks | 2. Medium/High IgG/IgM anticardiolipin anti- bodies |
| 3. ≥3 unexplained consecutive spontaneous abortions before 10 wks | 3.Anti β 2 gylcoprotein antibodies |
| 4. ≥ 1 episodes of arterial, venous/small vessel thrombosis in any tissue / organ |
Case Report
A 27 year old, G2A1 with 38weeks of POG gives H/o polycystic ovarian syndrome treated with OCPs for 3 months, which triggered pulmonary embolism. She had syncopal attacks 2 years ago, 2D ECHO showed pulmonary hypertension and CT pulmonary angiogram done and diagnosed to have pulmonary thromboembolism, started on Tab. Acitrom for 1 year. Next year she developed right lower limb DVT On further evaluation she was found to be having APLA syndrome, Hyperhomocysteinemia, Protein C and S deficiency and continued anticoagulant therapy. Patient had spontaneous abortion at 2MOA 1year ago. Pre conception counselling done. Patient presented with pregnancy test positive in first trimester and followed up till term. Patient was asymptomatic throughout the present pregnancy. She was on Tab. Ecosprin 75mcg and Inj Dalteparin 5000IU OD daily from first trimester. 2DECHO, Lower limb Doppler were normal. PT, APTT, INR were monitored. Patient was admitted at 38 weeks with h/o decreased fetal movements and oligohydramnios. After taking cardiology opinion and Preanesthetic evaluation, LMH was changed into unfractionated heparin 5000IU IV tid and it was stopped 12 hours before planning for delivery. Induction of labour done with dienoprostone gel, patient had an uneventful full term vaginal delivery of female baby of 2.9kg. Both mother and baby were healthy. Inj Heparin 5000IU IV and Tab Acitrom
2mg OD were restarted after 24hours of delivery for 5days, serial coagulation profile monitored. After five days Inj Heparin stopped and Patient discharged with Tab Acitrom 2mg OD. With PT 11, APTT 26, INR 0.9.
Discussion
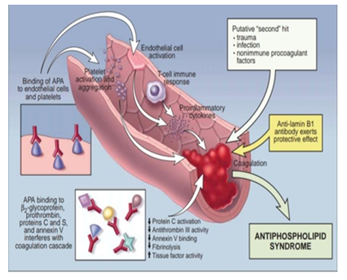
APLA is defined by presence of thromboembolic complications and pregnancy morbidity in the presence of increased titer of antiphospholipid antibodies. APLA syndrome without any underlying disease is termed as primary APLA syndrome and secondary antiphospholipid antibody syndrome is associated with SLE. Antiphospholipid reduce hCG release and inhibit trophoblast invasion which may explain miscarriages and fetal loss in the second trimester is associated with severe growth restriction, oligohydramnios and early onset preeclampsia possibly due to abnormal placentation related to thrombosis (Figure 1). Abnormalities in decidual spiral arteries like narrowing, intimal thickening, acute arthrosis and fibrinoid necrosis may be the immediate cause of fetal loss. Some authors state that antiphospholipid activates endothelial cells and complement system and hence cause pregnancy loss. Glycoprotien-1 triggers coagulation and inhibits ant thrombin 3 and fibrinolysis leading to thrombosis [5, 6].
Clinical Features
- Venous thromboembolism (DVT or PE)
- Arterial thrombosis, infarcts & Stroke
- Recurrent miscarriage
- Severe pre-eclampsia & IUGR
- Placental abruption & Intrauterine demise
- Livedo reticularis (esp with lupus)
- Rare –Thrombocytopenia Haemolytic anaemia
- Catastrophic APS: rapid onset thrombosis, multiorgan dysfunction with a systematic inflammatory response. Death occurs in 50% of patients. Management of APS during pregnancy should be aimed to avoid early pregnancy loss, normalize placental and fetal circulations to prevent early birth from preeclampsia and growth restriction and to prevent maternal vascular thrombosis in pregnancy and postpartum. Using appropriate treatment strategies, the likelihood of successful pregnancy in APS is about 70% (Table 2).
| Management of APS during Pregnancy | ||
|---|---|---|
| 1.Pre pregnancy | Counsel regarding risks of APS | |
| Discuss anticoagulation prophylaxis | ||
| Transition from warfarin to low molecular- weight heparin in patients with thrombosis history | ||
| 2. Antenatal | Provide multidisciplinary care | |
| Prenatal visits every 2-4weeks until 20-24 weeks and every 1-2weeks thereafter | ||
| Initiate fetal surveillance at 32weeks | ||
| Anticoagulation prophylaxis5 | ||
| APS without prior thrombosis | APS with thrombosis | |
| Recurrent pregnancy loss/ fetal death or early delivery <34weeks due to severe preeclampsia : | Low-molecular-weight heparin Eg: enoxaparin 1mg/ kg 12hourly with monitoring of anti-Xa activity | |
| Aspirin (75- 150mg) acts by preventing thrombosis & damage to trophoblast. | ||
| Unfractionated heparin (5000IU BD) subcutaneous | ||
| Low-molecular-weight heparin :Enoxaparin 40 mg sc OD | ||
| Only antibodies + no clinical features : | ||
| Aspirin only | ||
| 3.Labour and delivery | Avoid postdates | |
| Continuous FHR monitoring | ||
| Stop anticoagulation 12-24 hours before planned induction/ caesarean section | ||
| Arrange blood and blood products | ||
| Active management of third stage of labour and follow PPH protocols | ||
| ICU availability | ||
| Compression stockings | ||
| 4. Postnatal | Resume anticoagulation 6hours after vaginal delivery and 12 hours after caesarean section | |
| Continue anticoagulation for 6weeks for women with no prior thrombosis and for lifelong in women with prior thrombosis | ||
| Warfarin is substituted for heparin |
Table 2: Management of APS during pregnancy.
Conclusion
Clinician need to be more vigilant and should have high suspicion of APLA in patient with recurrent abortions. Resources for detection of APLA should be made readily available in resource limited settings. Management of APLA involves improving maternal and fetal outcomes, prevention of thrombosis with close monitoring of patient on anticoagulant could be challenging.
References
-
Hanly JG (2003) Antiphospholipid syndrome: an overview. CMAJ 168(13): 1675-1682.
-
Cunningham FG, Leveno KJ, Bloom SL, Spong CY, Dashe JS, et al. (2018) Williams obstetrics. 24th(Edn.), McGraw- Hill Education Medical, New York, pp: 1-1377.
-
Kaiser J, Branch DW (2016) Recurrent Pregnancy Loss: Generally Accepted Causes and Their Management. Clin Obstet Gynec 59(3): 464-473.
-
Mahajan K, Katyal V, Arya S, Sharma M (2015) Antiphospholipid syndrome in a pregnant female presenting with severe thrombocytopenia and bleeding. Case Rep Med 2015: 234878.
-
Ankur N, Kochar S, Verma A, Suthar N, Sushma (2019) Case Report on a successful Pregnancy outcome of Antiphospholipid antibody syndrome. Int J Sci Res 8(4): 1-2.
-
David J, Philip S, Carl PW, Bernard G, Stephen R (2017) Autoimmune diseases in pregnancy. High risk pregnancy; management options 25th (Edn.), Cambridge university press, pp: 1126-1134.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’