A Rare Case of Vaginal Agglutination in Reproductive Age Group
Labia minora partial or total adhesion is known as labial agglutination. It commonly occurs in postmenopausal or prepubertal women and is accompanied by low oestrogen levels. Due to the high levels of oestrogen in women in the reproductive age group, labial agglutination is uncommon. Due to its uncommon presentation and a unique approach to treatment in this age group, where the patient has been suffering from infancy, we are presenting a case of labial agglutination in a female who is 22 years old. After a comprehensive clinical examination, extensive history-taking and all necessary laboratory and imaging tests, we were able to make the right diagnosis, which was then treated with expert surgery. Her abnormal vestibular structure was treated with this method without any complications. Patient was treated by surgery i.e. labial adhesiolysis under vaginoscopic approach using our standard hysteroscope light and camera. Labial adhesion can be treated both medically and surgically however treatment is individualized in every case ranging from medical treatment to minimally invasive surgery or invasive skillful surgery.
Case Report
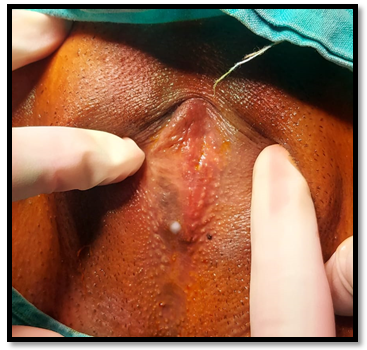
A 22 years old, sexually inactive girl was presented with the chief complaint of post micturition dribbling of urine and dysmenorrhea for the last 3 years. She noticed that the vaginal opening was not visible and she passed urine through small opening. Since menarche, she had experienced regular menstrual periods. At 12 years of age, she attained menarche. She also had history of chronic kidney disease stage 5. She had no history of any genital trauma or sexual assault or chronic vulval infection. On examination she had B4 stage of breast development P4 stage of pubic hair development and A3 stage of axillary hair development. She was found to have well-developed labia majora on the local examination. There seemed to be no dermatological disorder of vulva and no signs of local infection or trauma. Between the clitoris and the posterior vestibule, there was thick adhesion that connected the two labia minora in the middle. There was complete fusion of labia minora with obliteration of the vaginal introitus and urethral meatus with a pin hole opening for urine and menstrual blood flow (Figure 1) and anal opening was in normal position. Infection was not detected in urine microscopic examination or in culture sensitivity. Pelvic transabdominal ultrasonography and MRI was suggestive of normal size and shape of uterus and ovaries as well as normal urinary tract. Clinical diagnosis of labial agglutination was made. General anaesthesia was planned for the procedure.
After proper preoperative preparation and after obtaining anesthesia and medical clearance patient was taken up for examination under anesthesia with guardian consent. Patient in dorsal lithotomy position. A small opening noted in the midline about 3cms below clitoris. Artery forceps introduced and opening dilated (Figure 2), then 2.7mm hysteroscope introduced through the dilated opening to enter vaginal canal and proceeded to hysteroscopy which showed normal findings. After confirming with the hysteroscopy findings labial adhesiolysis done manually with artery forceps. Anatomy was restored (Figure 3).

After surgery, vagina, vaginal canal and urethral opening were absolutely normal. Post-procedure cystoscopy was done which showed normal findings. Post operative period was uneventful. Estrogen cream for local application thrice a day for 3 months given.

After a week, a month and a year, the patient was checked in on. Her labia majora and minora, introitus, and urethral opening were all normal at the time of the checkup, and she had no urinary problems or recurrence of the labial adhesion.
Discussion
Labial fusion is a state of partial or complete adhesion of the labia minora generally occurring in young girls or post-menopausal women, but is extremely rare in females after attaining puberty because of abundance of estrogen and normal working ovaries [1]. Up to 2% of prepubertal girls may develop labial adhesions, and the average age at which they first manifest is two years old. When females of reproductive age do get labial adhesions, they typically have a history of genital trauma or genital irritability. Genital trauma can take many different forms, such as childbirth, sexual abuse, and genitourinary surgery. Treatment for these patients typically involves topical oestrogen cream application and adhesion lysis. The postmenopausal period, which likewise has low oestrogen levels, may also have labial adhesions. Due to the low oestrogen levels in this period, the vaginal region is more prone to irritation and inflammation, which could result in adhesion. When a patient in this age range has a history of diabetes mellitus, lichen sclerosis, or reduced sex, the chance of fusion rises. The cloacal tube, which is closed at the seventh week, forms as the embryo grows and becomes narrower as it connects the two portions of the cloaca. If embryonic development stops before the seventh week, different degrees of cloacal malformation can form, which may present as a current thin septum between the urethra and vagina [2]. The female sinus ridge can descend more slowly after exposure to androgen, which is also enough to bind the vagina to the urethra and stop the vulva from opening [3].
Therefore, excessive androgen or abnormal activation of androgen receptors by unknown factors may be the etiology of congenital labia minor fusion, and further genetic testing is needed [3]. The relative hypoestrogenic environment is suggested as the main predisposing factor of this condition in prepubertal girls [4]. Only the symptoms like recurrent urinary tract infection and other symptoms like poor personal hygiene, genital trauma, vulvovaginal infections demand need for aggressive treatment in labial agglutination. In the present case low estrogen status was excluded to be the cause of her labial agglutination because patient had history of regular menses, normal ovaries in ultrasound and fully developed secondary sexual character. Neither genital injury nor sexual assault had ever occurred to her. In literature search, only few cases of labial fusion has been reported in reproductive age women [5]. Topical estrogen application becomes the first line management in minor cases. In addition, manual separation of adhesions with care and maintenance of local hygiene have also been reported to resolve pediatric labial adhesions [6]. Surgical adhesiolysis is the treatment of choice in our case and local estrogen application post operatively is proven to be beneficial in our case. So, we opted for vaginoscopic approach followed by adhesiolysis due to adhesion.
References
-
Tsujita Y, Asakuma J, Kanbara T, Yoshii T, Azuma R, et al. (2010) A case of labial adhesion in a reproductive woman. Hinyokika Kiyo 56(8): 463-465.
-
Roly ZY, Backhouse B, Cutting A, Tan TY, Sinclair AH, et al. (2018) The cell biology and molecular genetics of Müllerian duct development. Wiley Interdiscip Rev Dev Biol 7(3): e310.
-
Larkins CE, Enriquez AB, Cohn MJ (2016) Spatiotemporal dynamics of androgen signaling underlie sexual differentiation and congenital malformations of the urethra and vagina. Proc Natl Acad Sci USA 113(47): 7510-7517.
-
Mayoglou L, Dulabon L, Alguacil NM, Pfaff D, Schober J (2009) Success of treatment modalities for labial fusion: A retrospective evaluation of topical and surgical treatments. J Pediatr Adolesc Gynecol 22(4): 247-250.
-
Kumar RK, Sonika A, Charu C, Sunesh K, Neena M (2006) Labial adhesions in pubertal girls. Arch Gynecol Obstet 273(4): 243-245.
-
Watanabe T, Matsubara S, Fujinaga Y, Asada K, Ohmaru T, et al. (2010) Manual separation followed by local cleanliness for paediatric labial adhesion. J Obstet Gynaecol Res 36(3): 667-670.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’