Case Series on Labial Fusion in Perimenopausal and Postmenopausal Woman
Labial fusion or agglutination is a diagnosis of exclusion we come across in perimenopausal and postmenopausal women and sometimes also in young females. Here we highlight a series of cases which had presented with urinary disturbances and turned out to be labial fusion. Labial fusion can be managed conservatively or might require surgical interference which is also quite simple. Hence vaginal examination is a must for women presenting with urinary disturbance to rule out this condition.
Rajeshwari Reddy T, Kamjula P* and Vasu R
Care hospitals, India *Corresponding author: Pragna Kamjula, Care Hospitals, India; Email: pragna.kamjula01@ gmail.com
Introduction
Labial fusion or agglutination is a rare entity we come across in Perimenopausal and postmenopausal women.
It is a diagnosis of exclusion wherein its management is easy. Hence we present the following cases and its methodology of management.
Essence
A patient presenting with urinary disturbance (incomplete voiding / dribbling urine) should have a local examination to look for the urinary orifice and vaginal orifice. In case of labial adhesion, counsel the patient regarding the options of medical management and surgical management. In case of failed medical management, there is always the option of surgical management including with vaginoplasty (i/c/o need for sexual activity).
Why this Matters
The diagnosis of labial fusion is always neglected as it is a rare phenomenon. When a patient presents with complaints of dribbling of urine or frequent vaginal discharge or itching in the vagina, vaginal examination is a must to help us give insight into the actual ongoing pathology and come to a conclusion for further plan of management. The treatment of labial fusion is not complicated as there is provision for even medical management along with surgical methods. The recovery is also satisfactory. There are no long-term implications when it occurs in young girls. It doesn’t affect her sex life or fertility. Hence we discuss the methodology of a treatment plan for labial fusion.
Case Scenario
We had come across 3 women who presented with complaints of labial fusion and difficulty in passing urine. Hereby discussing a 48-year-old woman who presented with dysmenorrhoea and complaints of labial fusion and difficulty in passing urine and used to take a long time to empty her bladder. Similarly, the other 2 patients included also had urinary tract infections and were treated accordingly.
- On Inspection of her external genitalia showed that her clitoris was normal, however, the urethral meatus and vaginal orifice were not seen on careful inspection of her vulva.
- On palpation of her external genitalia, there was a pinhole opening at the midpoint between her clitoris and anus.
Hence sent for higher imaging. Mri pelvis showed large fibroid uterus of 9 x9 cm in the fundoanterior wall of uterus with normal ovaries with normal vaginal cavity with thin membrane over the external genitalia. Dilatation was performed under local anaesthesia but failed. Hence patient was counselled for hysterectomy with vaginoplasty i/v/o requirement of sexual activity later on.
Intraoperatively, after Blunt dissection of the vulval area, raw area was noted extending from cervix anteriorly for 3 cm below on the anterior aspect of vagina. Another raw area extending from 3 to 7’0 clock position in lower third of vagina in posterior wall. There was irregular laceration on vulva at 11’0 clock position. Mc Indoe vaginoplasty was done Wounds debrided. Partial thickness graft harvested from left high and fixed over raw area with 4-0 vicryl (Figure 1).

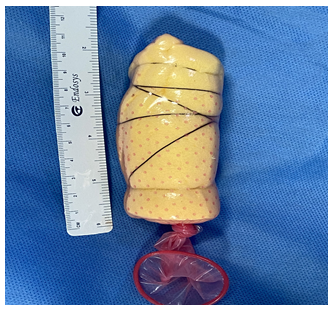
Vaginal cavity maintained and spacer created with condom and foam (Figure 2,3).

Similarly 45-year-old Perimenopausal woman came with complaints of difficulty in passing urine and on examination revealed labial fusion hence advised estrogen cream for local application following which after thinning of the membrane, blunt dissection was done and fusion released. Also a 62-year-old postmenopausal woman came with complaints of dribbling urine continuously after passing urine, on examination revealed labial fusion with a thick membrane with a small opening in the center. The patient was counselled regarding the need for a dilatation procedure, hence surgically adhesion was released, and advised continuous follow-ups and hygiene. Clinically, none of the patients had malignancy or lichen in the pathology specimens. At the three-week postoperative evaluation, an uneventful healing process was noted for all patients, and there were no complications and no recurrence of the labial agglutination.
Discussion
Labial adhesion is also called synechiae of the vulva, vulvar fusion, agglutination or conglutination of the labia minora, and adhesion of the labia minora. Labial fusion, or labial adhesion, is termed when the inner lips (labia minora) around the vagina become sealed together. In some cases, this can completely seal the vaginal opening, leaving a very small gap at the front that urine passes through. It is most commonly seen in girls under 7 years old and is usually nothing to worry about. It is rarely seen in adults or postmenopausal women. The exact incidence of labial fusion is unknown. In 1993, beck N, et al. [1] reported an incidence rate of 0.6% to 1.4% in children. However, the incidence in the elderly has to be elucidated. The etiology of labial adhesion is not so clear, although vulvovaginitis and mechanical irritation have been implicated as causative risk factors [2]. In addition, chronic inflammation is thought to cause denudation of surface epithelium, thereby allowing the labia to adhere to each other and result in the obstruction of the introitus [3]. Also causes of labial fusion in reproductive-aged women include poor hygiene, dermatitis, trauma, female circumcision, and lichen sclerosis [4, 5]. Other rare causes are Mucous membrane pemphigoid, Bechet syndrome, Stevens-Johnson syndrome, Vulval cancer, Female circumcision operation (which is illegal in many countries), and complications from vulvectomy.
Additionally, Seehusen, et al reported 9 cases of vaginal or labial adhesions requiring surgical corrections due to minor vaginal distortions occurring after healed intrapartum lacerations [6]. Symptomatic labial fusion often presents with vulval pruritus, and rarely with urinary incontinence, voiding difficulty, urinary retention, and dysuria [7]. Dyspareunia or sometimes this condition is associated with a hypoestrogenic state in the intrauterine and neonatal period. Most of the time there was no history of sexual abuse or trauma. There are as such no complications of labial fusion. It doesn’t affect woman’s future fertility or sexual life. In most cases, a fusion corrects itself during puberty. Rarely, labial fusion can cause infection (such as a urinary tract infection), soreness or pain in the genital area, urine becoming trapped in the vagina, leading to urine leaking between visits to the toilet. On local examination, the genitalia have a flat appearance, wherein labia minora might not be seen separately. Anterior fusion is often associated with disappearance or fusion of clitoral hood (the skin covering the clitoris). Posterior vulval fusion may be due to scarring of the perineum (the tissue between the vagina and anus). Colour changes (white from scarring, red from inflammation, or brown from previous inflammation), Blisters, erosions and ulcers, Patches or lumps.
Treatment of choice for patients with labial fusion includes topical estrogen cream especially in prepubertal girls and postmenopausal woman [8], manual separation [9]
or surgery. However, the most common treatment for cases of adult labial adhesion is adhesiolysis. A lack of estrogen before puberty can cause labial lips to stick to each other, hence application of estrogen cream daily on the central line of fusion for at least 4-6 weeks helps the membrane to dissolve and the labia to eventually separate completely. Once the membranes dissolves the cream should be stopped as to ensure further adhesion, an emollient should be applied [10]. For adult patients, estrogen therapy is not always successful as a first- line treatment, and surgery may be necessary when the fusion is particularly thick and severe or when there’s trapped pee in the vagina, which can dribble out after peeing and cause vulval soreness. Surgical separation is quite easy which can be done through hand after application of local anaesthetic or by blunt dissection. Topical corticosteroids to be applied to control the inflammation, along with regularly stretching the opening using fingers, vaginal dilators or regular sexual intercourse. Additionally, some authors have suggested Fenton procedure to remove the scar tissue. Or Surgery to bring out uninvolved vaginal tissue to the skin surface also known as paraneoplastic. A rare case was reported in an 86- year old woman with complete labial adhesion, the adhesion overlying the vestibule was manually separated and the skin defect was covered with bilateral vulvoperineal flaps. Reconstruction using the vulvoperineal flap enabled to prevent recurrence by covering with normal skin tissue. After surgery, none of the patients had total readhesion. Recurrence is often a problem in the treatment of labial adhesions, and its recurrence rate after surgical or manual procedure is 14%–20% [11]. The main advantage is the report of a series of patients with a rare benign gynaecological condition who had a standardized surgical approach and then a medium- term uniform follow-up regarding complications and recurrence of labial fusion. To conclude, Genital examinations are a basic method of analysis for a woman presenting with such complaints.
Labial fusion should be kept in mind in the differential diagnosis of urinary retention presenting in reproductive aged women without discernible etiological factors. In addition, due to a heavy clinical load and advances in modern medical knowledge and technology, laboratory and imaging studies are often arranged prior to a genital examination. This case report highlights that genital examinations should be a priority for patients with gynaecological or urological symptoms, Otherwise, the diagnosis of labial fusion may be delayed until the reproductive years.
References
-
Norbeck JC, Ritchey MR, Bloom DA (1993) Labial fusion causing upper urinary tract obstruction. Urology 42(2): 209-211.
-
Finlay HV (1965) Adhesions of the labia minora in childhood. Proc R Soc Med 58(11 part 1): 929-931.
-
Pulvino JQ, Flynn MK, Buchsbaum GM (2008) Urinary incontinence secondary to severe labial agglutination. Int Urogynecol J Pelvic Floor Dysfunct 19(2): 253-256.
-
Awang NAB, Viegas C, Viegas OAC (2004) Incomplete bladder emptying due to labial fusion in a pubertal girl: a delayed consequence of female circumcision. Aust N Z J Obstet Gynaecol 44(4): 372-373.
-
Norbeck JC, Ritchey MR, Bloom DA (1993) Labial fusion causing upper urinary tract obstruction. Urology 42(2): 209-211.
-
Seehusen DA, Earwood JS (2007) Postpartum labial adhesions. J Am Board Fam Med 20(4): 408-410.
-
Julia J, Yacoub M, Levy G (2003) Labial fusion causing urinary incontinence in a postmenopausal female: a case report. Int Urogynecol J Pelvic Floor Dysfunct 14(5): 360-361.
-
Dirim A, Hasirci E (2011) Labial fusion causing urinary incontinence and recurrent urinary tract ınfection in a postmenopausal female: a case report. Int Urogynecol J 22(1): 119-120.
-
Watanabe T, Matsubara S, Fujinaga Y, Asada K, Ohmaru T, et al. (2010) Manual separation followed by local cleanliness for pediatric labial adhesion. J Obstet Gynaecol Res 36(3): 667-670.
-
Lazarou G, Maldonado MQ, Mitchell K (2013) Complete labial fusion with vaginal constriction band presenting as incomplete voiding. Female Pelvic Med Reconstr Surg 19(3): 181-183.
-
Schober J, Dulabon L, Alguacil NM, Kow LM, Pfaff D (2006) Significance of topical estrogens to labial fusion and vaginal introital integrity. J Pediatr Adolesc Gynecol 19(5): 337-339.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’