Challenge and Prospect of Pre Implantation Genetic Diagnosis-A Mini Review
Pre-implantation genetic diagnosis (PIGD) is the genetic profiling of the embryos prior to implantation and sometimes even of oocytes prior to fertilization. PGD is considered in a similar fashion to prenatal diagnosis. Initially offered for diagnosis in couples at risk for single gene genetic disorders, such as cystic fibrosis, spinal muscular atrophy and Huntington’s disease, preimplantation genetic diagnosis (PGD) has most frequently been employed in assisted reproduction for detection of chromosome aneuploidy from advancing maternal age or structural chromosome rearrangements. Major improvements have been seen in PGD analysis with movement away from older, less effective technologies, such as fluorescence in situ hybridization (FISH), to newer molecular tools, such as DNA microarrays and next generation sequencing. Discussions regarding the scientific, ethical, legal and social issues surrounding the use of sequence data from embryo biopsy have begun and must continue to avoid concern regarding eugenic or inappropriate use of this technology.
Introduction
The world’s first PGD was performed in 1990 by Handyside, Kontogianni and Winston at the Hammersmith Hospital in London [1]. The term Preimplantation genetic screening (PGS) refers to set of techniques for testing whether the embryos obtained through In Vitro Fertilization (IVF)/ Intra Cytoplasmic Sperm Insemination (ICSI) has abnormal chromosomes number. The PGD allows studying the DNA of eggs or embryos to select those that carry certain mutation for genetic diseases. It is useful when there are previous chromosomal or genetic disorders in the family and within the context of IVF program [2]. Here a concise review was done on PGD/ PGS regarding its current status, both domestically and globally, as well as its future challenges.
Historical Aspect
Pre-implantation genetic diagnosis (PIGD) was first introduced in 1990 by selecting female embryos in order to prevent the birth of male patients affected with X-Linked
recessive disorders [3].
Applications
It is well recognized by the clinical community that it is indicated in preventing monogenic inherited disorders with severe morbidity and mortality [4]. PGD may also be used to increase chances of successful pregnancy, to match a sibling in Human leukocyte antigen (HLA) type in order to be a donor, to have less cancer pre-deposition, and for sex selection.
Used in Monogenic Disorders
Monogenic disorders that is, disorders due to a single gene only (autosomal recessive, autosomal dominant or Xlinked) or of chromosomal structural aberrations (such as balanced translocation). The most frequently diagnosed autosomal recessive disorders are cystic fibrosis, beta- thalassemia, sickle cell disease and spinal muscular atrophy type-1. The most common dominant diseases are myotonic dystrophy, Huntington’s disease and CharcotMarie-Tooth disease and in the case of X-linked diseases, most of the cycles are performed for Fragile X syndrome, haemophilia A and Duchenne muscular dystrophy.
HLA Matching and Cancer Predisposition
Human leukocyte antigen (HLA) typing of embryos, so that the child’s HLA matches a sick sibling, availing for cord-blood stem cell donation [5]. The child is in this sense a “Savior sibling” for the recipient child. HLA typing has meanwhile become an important PGD indication in those countries where the law permits it [6]. A more recent application of PGD is to diagnose Late-onset diseases and cancer predisposition syndromes. Since affected individuals remain healthy until the onset of the disease, frequently in the fourth decade of life, there is debate on whether or not PGD is appropriate in these cases.
Sex Discernment
Pre-implantation genetic diagnosis provides a method of prenatal sex discernment even before implantation, and may therefore be termed pre-implantation sex discernment. It is also necessary to perform a biopsy on these embryos in order to obtain material on which to perform the diagnosis. Generally, PCR-based methods are used for monogenic disorders and FISH for chromosomal abnormalities and for sexing those cases in which no PCR protocol is available for X-linked disease. Most clinics perform it only for “family balancing”, which is where a couple with two or more children of one sex desire a child of the other, but half do not restrict sex selection to family balancing. In India, this practice has been used to select only male embryos although this is illegal [7].
Recent Perspective on Sampling Approaches
In PGD/PGS, there are three major biopsy methods: blastocyst biopsy, blastomere biopsy, and polar body (PB) biopsy. Blastocyst biopsy has been more widely used than PB biopsy and blastomere biopsy, especially in the past 5 years, due to its low misdiagnosis rate [8, 9] and cost-effectiveness [10, 11]. Compared to the conventional biopsy methods, the newly developed non-invasive sampling methods have many advantages with regard to the ethical, legal, and economic issues.
Advanced Techniques of Genetic Analysis in PGD
Polymerase chain reaction (PCR), methods detect many genetic abnormalities such as single-gene mutations chromosomal imbalances [12], and mitochondrial mutations [13]. Fluorescence in-situ hybridization (FISH) had been performed to screen aneuploidy and chromosomal translocation for many years [14]. However, these two methods become obsolete due to their limitations, e.g., incapability of detecting de-novo genetic mutations, contamination, and sensitivity issues that lead to the false positive or negative. New diagnosis methods, such as array-comparative genomic hybridization (aCGH), single- nucleotide polymorphism (SNP) microarray, multiplex quantitative PCR (qPCR), karyomapping, and next generation screening (NGS) are developed to improve clinical efficiency and outcomes [15, 16, 17] (Figure 1).
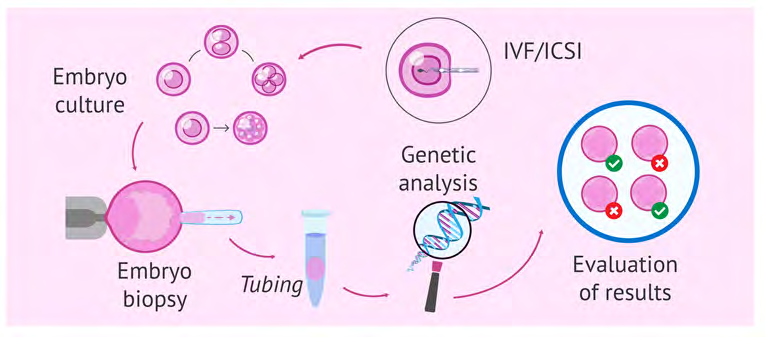
Technical Aspect
PGD is a form of genetic diagnosis performed prior to implantation. This implies that the patient’s oocytes should be fertilized in-vitro and the embryos kept in culture until the diagnosis is established. It is also necessary to perform a biopsy on these embryos in order to obtain material on which to perform the diagnosis. Generally, PCR-based methods are used for monogenic disorders and FISH for chromosomal abnormalities and for sexing those cases in which no PCR protocol is available for X-linked disease (Figure 2).
Ethical Issues
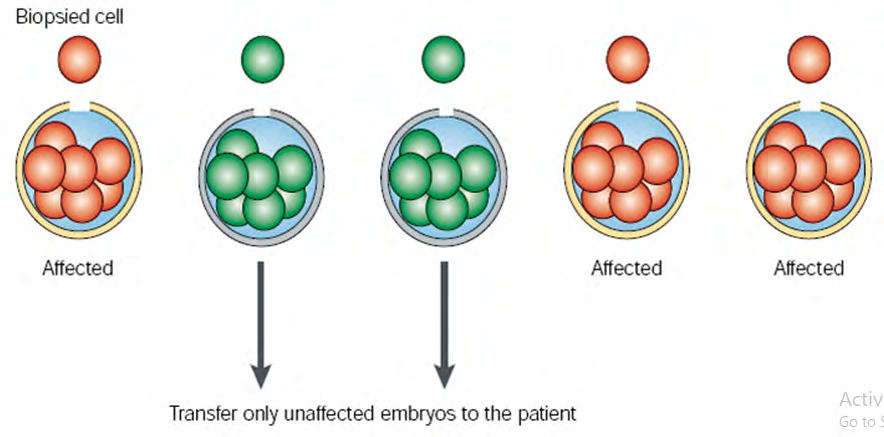
PGD has raised ethical issues, although this approach could reduce reliance on fetal deselection during pregnancy. The technique can be used for prenatal sex discernment of the embryo, and thus potentially can be used to select embryos of one sex in preference of the other in the context of “Family balancing”. It may be possible to make other “social selection” choices in future that introduce socioeconomic concerns. Only unaffected embryos are implanted in a women’s uterus, those that are affected are either discarded or donated to science [18]. The concept of a “designer baby” is closely related to the PGD technique, creating a fear that increasing frequency of genetic screening will move toward a modern eugenics movement [19].
Discussion
Pre-implantation genetic diagnosis (PGD) is a form of prenatal diagnosis that is performed on early embryos created by in vitro fertilization (IVF). In comparison to other established methods of prenatal diagnosis, such as chorionic villus sampling and amniocentesis, PGD is not performed on an outgoing intrauterine pregnancy in the late first or early second trimester, but on embryos developing in the IVF laboratory prior to transfer to the uterus. Despite some misconception to the contrary, PGD is not a therapeutic procedure for embryo; there are no change to the DNA or any other genetic-related structures. It is solely a diagnostic procedure that can identify whether a specific embryo carries a single gene disorder for which the couple is at- risk or a chromosomal abnormality that could lead to failed implantation, subsequent miscarriage or the birth of a child with physical and/or developmental disability.
Fetal cells and free fetal DNA are also present in the circulation of the pregnant mother and provided a potential source for “non-invasive” fetal sampling, but reliable protocols have yet to be established for clinical application [20, 21]. As data have accumulated from chromosomal analysis of human pre-implantation embryos, it has become apparent that there is higher rate of chromosomal abnormalities in cleavage stage embryos and blastocyst detected by FISH [22, 23]. Reported pregnancy rates vary, but rarely surpass about one third of all cycles initiated [24, 25]. The safety of PGD for children born is a major concern, but initial evaluation of about 250 babies born worldwide after PGD indicated that the procedure had no adverse consequence on early development [26, 27]. There is also public concern about the use of PGD to prevent the birth of children with the severe genetic disorders, there are few countries which has begun to offer PGD for “social” sexing. Thus, it is imperative to establish appropriate ethical guidelines and legislation as soon as possible.
Conclusion
PGD remains a technically challenging, multistep, labour intensive procedure which requires the close collaboration of a team of specialists. Efforts continue to ameliorate and simplify protocols, particularly for genetic analysis and to develop methods for more disorders, but present technologies still limit wider application.
References
-
Handyside AH, Kontogianni EH, Hardy K, Winston RM (1990) Pregnancies from biopsied human preimplantation embryo sexed by specific DNA amplification. Nature 344 (6268): 768-770.
-
Latham SR (2009) The once and future debate on human embryonic stem cell research. Yale J Health Policy Law Ethics 9: S483-S494.
-
Kuliev A, Rechitsky S (2017) Preimplantation genetic testing: current challenges and future prospects. Expert Rev Mol Diagn 17(12): 1071-1088.
-
Geraedts JPM, Wert GMWRD (2009) Preimplantation genetic diagnosis. Clin Genet 76(4): 315-325.
-
Verlinsky Y, Rechitsky S, Schoolcraft W, Strom C, Kuliev A (2001) Preimplantation diagnosis for Fanconi anemia combined with HLA matching. JAMA 285(24): 3130- 3133.
-
Baruch S, Kaufman D, Hudson KL (2008) Genetic testing of embryos: practices and perspectives of US in vitro fertilization clinics. Fertil Steril 89(5): 1053-1058.
-
Fragouli E, Wells D (2018) Current status and future prospects of noninvasive pre-implantation genetic testing for aneuploidy. Fertil Steril 110(3): 408-409.
-
Munne S, Weier HU, Grifo J, Cohen J (1994) Chromosome mosaicism in human embryos. Biol Reprod 51(3): 373- 379.
-
Novik V, Moulton EB, Sisson ME, Shrestha SL, Tran KD, et al. (2014) The accuracy of chromosomal microarray testing for identification of embryonic mosaicism in human blastocysts. Mol Cytogenet 7(1): 18.
-
Schoolcraft WB, Fragouli E, Stevens J, Munne S, Jaffe MGK, et al. (2010) Clinical application of comprehensive chromosomal screening at the blastocyst stage. Fertil Steril 94(5): 1700-1706.
-
Greco E, Biricik A, Cotarelo RP, Iammarone E, Rubino P, et al. (2015) Successful implantation and live birth of a healthy boy after triple biopsy and double vitrification of oocyte-embryo-blastocyst. Springerplus 4: 22.
-
Fiorentino F, Kokkali G, Biricik A, Stavrou D, Ismailoglu B, et al. (2010) Polymerase chain reaction-based detection of chromosomal imbalances on embryos: the evolution of preimplantation genetic diagnosis for chromosomal translocations. Fertil Steril 94(6): 2001-2011.
-
Sallevelt SCEH, Dreesen JCFM, Drüsedau M, Spierts S, Coonen E, et al. (2013) Preimplantation genetic diagnosis in mitochondrial DNA disorders: challenge and success. J Med Genet 50(2): 125-132.
-
Griffin DK, Handyside AH, Penketh RJ, Winston RM, Delhanty JD (1991) Fluorescent in-situ hybridization to interphase nuclei of human preimplantation embryos with X and Y chromosome specific probes. Hum Reprod 6(1): 101-105.
-
Keltz MD, Vega M, Sirota I, Lederman M, Moshier EL, et al. (2013) Preimplantation genetic screening (PGS) with comparative genomic hybridization (CGH) following day 3 single cell blastomere biopsy markedly improves IVF outcomes while lowering multiple pregnancies and miscarriages. J Assist Reprod Genet 30(10): 1333-1339.
-
Treff NR, Su J, Tao X, Northrop LE, Scott RT (2011) Single- cell whole-genome amplification technique impacts the accuracy of SNP microarray-based genotyping and copy number analyses. Mol Hum Reprod 17(6): 335-343.
-
Forman EJ, Upham KM, Cheng M, Zhao T, Hong KH, et al. (2013) Comprehensive chromosome screening alters traditional morphology-based embryo selection: a prospective study of 100 consecutive cycles of planned fresh euploid blastocyst transfer. Fertil Steril 100(3): 718-724.
-
Braude P, Pickering S, Flinter F, Ogilvie CM (2002) Preimplantation Genetic Diagnosis. Nat Rev Genet 3(12): 941-953.
-
Savulescu J (2001) Procreative beneficence: why we should select the best children. Bioethics 15(5-6): 413- 426.
-
Cheung LP (2000) Patient selection for assisted reproductive technology treatments. Hong Kong Med J 6(2): 177-183.
-
Rutherford AJ, Sharpe RJS, Dawson KJ, Margara RA, Franks S, et al. (1988) Improvement of invitro fertilization after treatment with buserelin, an agonist of luteinising hormone releasing hormone. Br Med J (Clin Res Ed) 296(6639): 1765-1768.
-
Ray PF, Ao A, Taylor DM, Winston RM, Handyside AH (1998) Assessment of the reliability of single blastomere analysis for preimplantation diagnosis of the delta F508 deletion causing cystic fibrosis in clinical practice. Prenat Diagn 18(13): 1402-1412.
-
Rechitsky S, Strom C, Verlinsky O, Amet T, Ivakhnenko V, et al. (1998) Allele drop out in polar bodies and blastomeres. J Assist Reprod Genet 15(5): 253-257.
-
Cieslak J, Ivakhnenko V, Wolf G, Sheleg S, Verlinsky Y (1999) Three-dimensional partial zona dissection for preimplantation genetic diagnosis and assisted hatching. Fertil Steril 71(2): 308-313.
-
Sermon K, Lissens W, Messiaen L, Bonduelle M, Vandervorst M, et al. (1999) Preimplantation genetic diagnosis of Marfan syndrome with the use of fluorescent polymerase chain reaction and the automated laser fluorescence DNA sequencer. Fertil Steril 71(1): 163- 166.
-
Strom CM, Levin R, Strom S, Masciangelo C, Kuliev A, et al. (2000) Neonatal outcome of preimplantation genetic diagnosis by polar body removal: the first 109 infants. Pediatrics 106(4): 650-653.
-
Eldar-Geva T, Srebnik N, Altarescu G, Varshaver I, Brooks B, et al. (2014) Neonatal outcome after preimplantation genetic diagnosis. Fertil Steril 102(4): 1016-1021.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’