Immunization against Invasive Candidiasis is the Exigency of the Decade
Fungal infections by Candida spp. have emerged as one of the major concerns of high mortality in immunocompromised patients. It is one of the kingpins of the critical priority group of WHO fungal priority pathogens list 2022. Modern medicine has made its way for the better treatment of diseases and bacterial infections. But with drug-resistance in bacteria causing millions of deaths and to add on the trouble, invasive fungal infections which remains unnoticed is culminating into a challenge among the immunocompromised patients. A proper understanding of the host-pathogen interaction and the detailed immunology against fungal pathogens provides a better insight. This helps in development of efficient strategies for new generation antifungals and vaccination. In this review invasive fungal infections or fungemia caused by Candida species will be the heart. According to WHO fungal priority pathogens list (WHO FPPL 2022) for this group of fungus no commercial vaccine is available and it has become the need of this decade. The current efforts and preventive strategies studied against this infection will help in the up growth of vaccination against Invasive Candidiasis (IC).
Introduction
Fungi are eukaryotic members containing membrane- bound organelles, including species of mycelia, yeasts, and molds. The basic characteristic that makes fungi unique as a separate kingdom is the presence of chitin in its cell wall [1]. Some fungi are edible like for example some species of mushrooms, Agaricus bisporus, Letinula edodes etc. They provide nutritional benefits. But most are commensal and when they multiply in the host cell, it becomes pathogenic and can cause diseases with high mortality rates. Communicable or infectious disease has different types of causative organisms. Among them fungal infections and diseases came into limelight after pandemic with various types of secondary infections like mucormycosis, aspergillosis and candidemia (WHO FPPL). These are not just limited to skin and hair but proceed to infect the entire body known as comorbid invasive fungal infections, having high mortality rate. WHO after its successful bacterial priority pathogen list (WHO BPPL) in 2017 has now published it first fungal priority pathogen list (WHO FPPL) in October 2022. According to the list Aspergillus, Candida, and Cryptococcus are ranked in the critical priority group that cause severe illnesses and infections to humans. Followed by Mucorales, Histoplasma, Fusarium, Eumycetoma and Candida species are in high priority group. Our focus will be only on critical and high priority group (the details of the species from WHO FPPL is in (Table 1). The major drawback in treating of fungal infection is that since they are eukaryotes, the antifungal drugs show detrimental effect even to the host cell. Due to this, a new approach to develop vaccine should be taken where the host cell can fight its own battle. Such a systemic fungal invasion of pathogens that destroy essential organs causes extensive lethality in human hosts. The group of high-risk people whose immune system is weakened, fungal infection like candidiasis is generally diagnosed in young infants, elderly people, and immunosuppressed individuals with conditions like diabetes, HIV/AIDS, steroid treatment, and of course, extensive cancer treatments like chemotherapy and radiation therapy and succumb to the infection as proper medication cannot be prescribed [2].
| Critical Priority Group | High Priority Group |
|---|---|
| Cryptococcus neoformans | Histoplasma spp. |
| Candida auris | Candida tropicalis |
| Aspergillus fumigatus | Fusarium spp. |
| Candida albicans | Eumycetoma & Mucorales |
Table 1: The two groups which this review focuses on from the WHO FPPL 2022 has divided the fungal species in according to the cr
Infection caused by fungal organisms came in to the limelight of research since 1990s as a predominant infection which can cause mortality and to be considered for medical research. But with time the number of such diseases has kept increasing since then [2]. With fungal infections spreading to blood makes it life threatening and it is termed as Invasive Fungal Infections (IFIs) or fungemia. The most prevalent species that are responsible for IFIs are Cryptococcus spp., Aspergillus spp. and Candida spp. Candida species are quotidian carriers for causing Invasive Candidiasis (IC). In human beings they are ranking in the top of the list in of WHO FPPL, for being life-threatening causative agents. Having high mortality and delayed recovery rates of nosocomial bloodstream infections in hospital environment. When Candida causes systemic fungal infections, it is known as Invasive Candidiasis. When IC occurs in blood it is known as Candidemia. One such Candida species that is a source of candidemia is the new ‘Superbug ‘Candida auris. That prevails in hospital setups (ICUs & OT) infecting immune compromised patients [3]. Immunocompromised patients are those who cannot defend themselves from opportunistic pathogenic infections due to their weak immune systems. Once C. auris circulates in the bloodstream, its diagnosis, treatment, and prevention becomes even more laborious [4].This highlights an increasing urge to develop an effective and preventive measure to cease the havoc caused by these fungus. The barrier which is preventing the protection of the patients with opportunistic fungal infections that have escalated to a systemic level is that they are impotent to launch protective responses due to their weakened immune systems. Hence, due to the rising resistance against the antifungals, which is making the existing ones ineffective and also have toxic effect on the weaken host makes us question about the treatment. A more appropriate line of prevention would be to help the body’s natural defense measures to fight their own battles. As a result, the gravity to develop a constructive vaccine which can be the only hope in this darkness to successfully immunize impuissant patients against fungal infections is the need of the hour. Immunization through vaccines helps protect the body from catching an infectious disease. The triumph in effective vaccine development has become an important aid to better healthcare for society. From the discovery of first vaccine by Dr. Jenner for cowpox, followed by development of rabies, polio and the recent COVID-19 pandemic, most of these diseases are prevented by their respective vaccines and have saved mankind [5]. Most vaccines are made of an attenuated or weakened immunogenic antigen joined with adjuvants administered to the human body for our immune system to provide innate protection or a memory against that antigen. Hence, if and when the same antigen happens to infect the host, it triggers an instinctive immune response within the body with a detailed memory of battle with that specific antigenic molecule from the pathogen. This will result in a very low spread of the disease and will decrease the risk of life of the patient. Owing to the aforementioned, the route of immunization through effective vaccines serves as a template to strengthen the host’s immune system to combat invasive fungal infections, including C. auris and other fungal pathogens causing invasive candidiasis, when they are incapable of doing so naturally. This in turn not only protects and saves people from infections but also economizes billions of dollars in healthcare industries [5]. The review focuses generally on to these fungal pathogens that are detrimental to human host and the roadmap for development of a commercial vaccine.
Immunosuppressed patients, such as the ones undergoing treatment for hematologic malignancies like leukemia, lymphoma and other cancer conditions develop an increased mortality rate of 35% due to fungal infections [6, 7, 8, 9]. On the other hand, high-risk patients suffering from Human Immunodeficiency Virus (HIV) are at a high rate of being susceptible to opportunistic fungal pathogens like Candida albicans and Cryptococcus neoformans. It culminates to roughly 47% of deaths per year despite antiretroviral (ARV) therapy [9, 10, 11, 12].
By virtue of these facts, it has become a necessity to generate vaccines that can protect such immunosuppressed and immunocompromised patients to develop a long - term memory using both innate and adaptive immunity.
We will ponder the updates on the advancement in vaccine development in correlation with invasive fungal infections [12, 13, 14].
The Plague of Candidiasis
Candida usually thrives in warm, moist environments like the mouth, diaper regions of babies, and in women, they can also be found in the vagina. There are approximately 200 species of Candida, out of which more than 20 are causative agents of diseases in humans. Important ones that are pathogenic are Candida albicans, Candida krusei, Candida auris, Candida parapsilosis, and Candida tropicalis [15]. Candida is typically labeled as an ‘opportunistic microbe’, dependent on the number of cells present in the body and the surrounding residual environment. At minimum cell count and growth, these cells are generally harmless. On the other hand, during immunocompromised state of the host, the immune system is down which allows the over growth of Candida cells and start invade other tissues, which leads to the cause of the disease [16]. C. albicans, the most studied microbe, has dimorphic phenotypes having contrasting protein profile expressions and giving different functional properties. Candida in yeast form is harmless; it just transposes them from one cell to another. Whereas in filamentous form, Candida cells are better at invading tissues and causing infection [16]. According to the Center of Disease Control and Prevention (CDC), the most widespread thrush can be seen as a vaginal yeast infection, oral thrush, and cutaneous candidiasis. Hence, being dimorphic, Candida albicans is considered not only a commensal organism but also an opportunistic pathogen that can gradually promote IC depending on the capability of immune defense lines [16, 17]. There are various options for treating candidiasis, but the mainstay remains to be antifungal agents against the causative organism like Fluconazole and others [13]. But another complexity arises when the patient is already having certain comorbidity and these anti-fungal agents while eliminating the pathogen also harms the already weaken host stated prior. Even sometimes these antifungals are ineffective as the organism have developed resistance or become persistent to it.
The modernization of healthcare facilities has paved the way for improved clinical diagnosis and treatment options which was once baffling to a content. While this is true, modernization can have various consequences, even to the patients who are making use of them [18]. One key example of such a consequence is the development of Bloodstream Nosocomial Infections in human immunocompromised primates. Over time, fungi and yeast have evolved from being justs superficial to causing serious Bloodstream Infections (BSIs). BSIs are infections that are caused due to the presence of viable pathogenic microorganisms in the blood that disseminate to other parts of the body serious enough to elicit an immune response [19, 20].
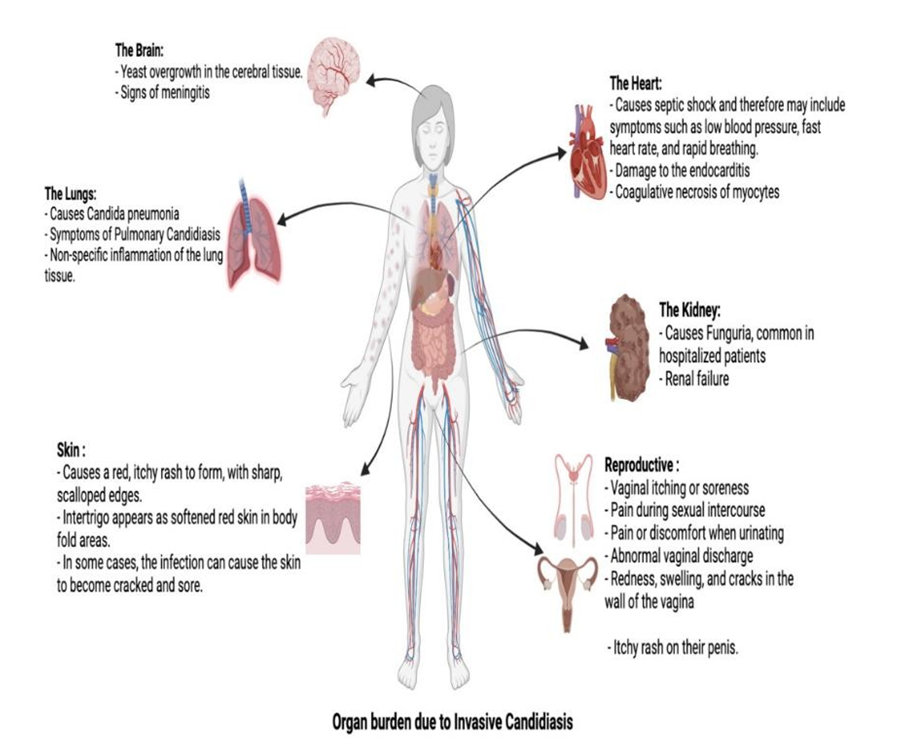
The major victims of the invasive fungal attack the skin, heart, brain, and respiratory organs [21, 22]. Candida spp. are the major causative agents of IFIs in healthcare settings, with Aspergillus spp. coming up second. Superficial infections are quite common for fungus and they are characterized by rough and cracked skin having sore rash over the infected area. With the risk of spreading, there are several ointments and topical creams given for their prevention. The brain and the heart are important and vital organs for the proper functioning of the body. Any infection to such organs would certainly be life threatening. This being said, an infected heart is generally characterized myocardial cell damage with or without the detection by a contraction band necrosis. In addition to that, large necrotic areas are seen with evidence of blastoconidia and budding yeast cells in the arterioles of myocardium and pericardium detected in the later stage of the infection. They are observed in the capillaries rather than the common cerebral tissues. An infected kidney can cause severe damage due to heavy necrotized areas with focal distribution of tubuli and multi- focal infiltration with yeast cells within the parenchyma tissue (Figure 1).
BSIs have been considered as one of the top seven causes of death by North American, Asian and European countries, amalgamated with a 13% to 20% mortality rate with 2 million episodes and around 250,000 deaths around the world [19]. The general research and literature synopsis of BSIs is more inclined towards bacterial infections like sepsis, meningitis, and bacteremia instead of Invasive bloodstream fungal infections. In general, even though fungal BSIs account for 71% of the total mortality rate data, fungal diseases receive less attention due to their epidemiological suppression compared to bacterial diseases [2, 13, 23]. Bloodstream infections specifically caused by Candida species account for 90% of all the fungal BSIs together with 53% mortality rate (WHO FPPL). To top that, a study revealed that the hospital and healthcare costs reach up to 563 million Australian Dollars (AUD), with $24 billion/year in the US alone [13, 24, 25, 26, 27, 28].
Despite the high mortality rate among the entire fungal community, there haven’t been much statistics found and collected after 2017. An additional challenge is the widespread epidemiology and sudden pathogenic emergence of new Candida strains. Several population- based studies have been demonstrated that reveal the distribution of C. albicans to non-albicans species varies by region clade. The non-albicans species discussed in this review are C. glabrata, C. tropicalis, and C. auris. Out of these, C. glabrata are generally found in Central and Northern Europe, whereas C. tropicalis is generally distributed in the Asia-Pacific region [29, 30]. C. auris on the other hand, is globally widespread with five clades spreading from India, Pakistan, South Africa, South America, North America, and many parts of Europe. There are other non-albican species that are distributed globally and available, but not discussed. This suggests that more work needs to be done concerning the statistical epidemiology of Candida species that cause BSIs in human beings. Out of these, a few studies are worth mentioning; a healthcare-based study done [31]. revealed the dispersion and incidence of these species from January 1997 to December 2000 showing the most prevalent species as C. albicans with 54%, descending with other non-albican species with C. glabrata at 16%, C. parapsilosis at 15%, C. tropicalis at 10% and the lowest of C. krusei at 2%.Another study released data ranging from 2010 to 2014, and the results were analogous to the previous study revealing the highest prevalence of C. albicans (48%), followed by C. parapsilosis (30%), C. tropicalis (10%), C. glabrata (9%), and lastly C. krusei (0.8%) [32]. A similar study showed the highest prevalence of C. albicans (37%), then C. parapsilosis (19.8%), C. tropicalis (14.9%), C. glabrata (7.4%), and lastly C. krusei (4.1%) [33]. Next study showed a compiled data from January 2006 to December 2017 revealed opposing lineage starting from the highest C. glabrata (30%), C. albicans (23.5%), C. parapsilosis (19.4%), C. tropicalis (17.9%), and then C. krusei (3.1%) [34]. this is the only study that shows a higher incidence of C. glabrata instead of C. albicans. Lastly, a study [35], showed similar results, giving C. albicans (47.4%) of highest incidence and episodes, and then subsequently C. parapsilosis (26.6%), C. tropicalis (9.6%), and the least with C. glabrata (7.6%) incidence.
Immunology of Fungal Infections
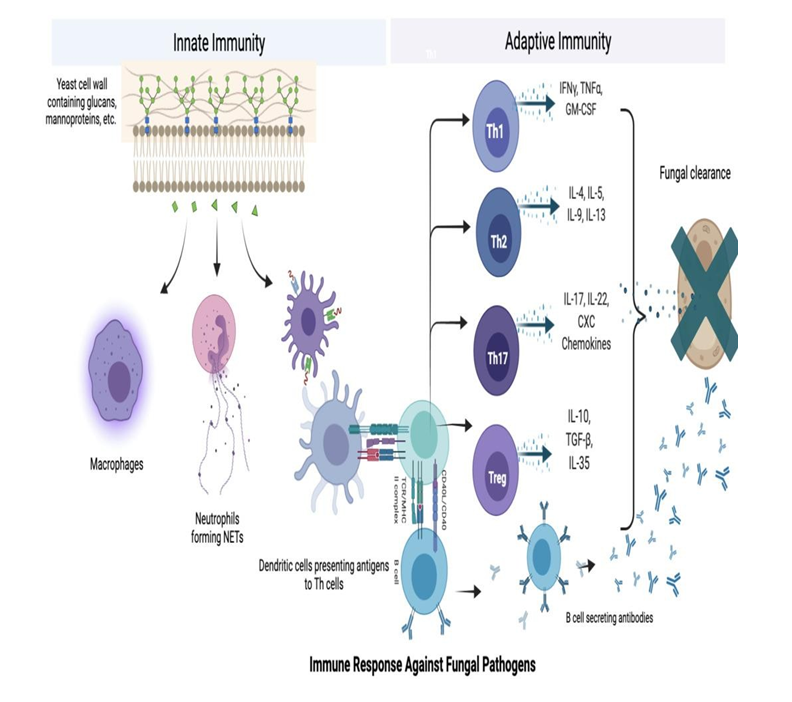
Humans tend to develop fungal infection or diseases when their cipher increases or immune system of the individual is compromised. Fungi are infamous among other infectious agents like bacteria and viruses; however, they possess elaborate and intricate tie-ups with the human and other vertebrate immune defense systems [36]. Exposure to fungal microbes having viable pathogenic activity induces a synchronized innate and adaptive immune response for proper eradication and functional effect of memory B cells of the encounter [36, 37]. Fungal organisms can affect various vital organs and causes cutaneous infections by Candida, respiratory infections by Aspergillus, and others. The primary antifungal response against fungal pathogens is dependent on innate immune cells like macrophages, dendritic cells, and neutrophils [36, 37, 38, 39]. The first and the most critical step is the recognition of foreign fungal antigens that invade the immune system, hence initiating an immune response. Fungal particles are either recognized or opsonized i.e., bind to opsonins in advance of binding [38]. Recognition is done by the innate cells - macrophages and dendritic cells and is facilitated by Pattern Recognition Receptors (PRR) of Pathogen- Associated Molecular Patterns (PAMPs) and opsonic receptors [37, 38]. Some examples of opsonic receptors are Complement receptors like CR3, Toll-like receptors (TLRs) like TLR4, TLR2, mannose receptors ,Dendritic Cell-Specific Intercellular adhesion molecule-3-Grabbing Non-integrin (DC-SIGN),glucan receptors, CD14, and Fc receptors of an immunoglobulin. Glucans, glycoproteins, and mannosylated proteins are some of the major components of the fungal and yeast cell wall which are key for PAMP recognition [1, 36, 37, 38, 39].
Binding of fungal particles to PRR leads to activation of intracellular signaling pathways, setting in motion the MAPK pathway hence activating MAP kinases [38, 40]. With this, NFKBs are translocated to the nucleus, where the genes for cytokines and chemokines are transcribed [38, 39, 40]. Cytokines such as Interleukin-1⍺ (IL-1⍺), IL-1β, IL-10, and TNF-⍺ are synthesized and released from cells, such that these cells are recruited to the site of infection and inflammation where they work their magic. Hence, macrophages are prime immune cells that are responsible to recognize fungal antigens and regulate responses like phagocytosis, antigen presentation to humoral cells, and secretion of immune modulators to defend against fungal infections [39, 41]. In case of IC neutrophils are the key blood cells that are activated and recruited to the site of infection. Their main mode of action involves phagocytosis, activation of Neutrophil Extracellular Trap (NET) formation, and the delivery of antimicrobial contents through them [42, 43].
The switch from our body’s defense lines to become adaptive from innate during fungal infections is primarily done by dendritic cells and macrophages [14, 43, 44]. These cells are phagocytes and are called Antigen-Presenting Cells (APCs), which then introduce the fungal antigen, to Major Histocompatibility Complex (MHC) II - bound Th cells. CD8 T cells or TCYT are also activated by dendritic cells after binding that fungal antigen to MHC I molecule [39, 44, 45]. With this, the commitment to effector Th subsets commences. These Th subsets are Th1, Th2, Th17, and Treg cells that help in various effector functions. All of these T helper subsets secrete their respective cytokines and chemokines that orchestrate an antimicrobial response against fungal pathogens invading the body [46]. The Th1 subset is critical in the immune response against fungi and its significance has been well recognized in many in vivo experiments involving murine models and human infection [46, 47]. Dendritic cells and macrophages recruited against fungi secrete IL-2 which is essential for Th1 lineage, following which the IL-2 pathway is established [47]. This cytokine pathway has been proven to be of great significance with many fungal diseases like Candidiasis, Cryptococcus, and Coccidioidomycosis. [1, 45].
The main cytokines released by Th1 subsets are IFN-γ, TNF-α, and GM-CSF [46, 48]. Out of these, the signature pro- inflammatory cytokine is IFN-γ which is responsible for exhibiting pleiotropic effects on immune cells during an infection, followed by the induction of classical activation of APCs that are important in arresting the growth and proliferation of fungal pathogens. On the other hand, the Th2 subset immune responses involve the secretion of IL-4, IL- 5, and IL-13, and exhibit calamitous effects on the host. The defense mechanisms carried out by Th2 secreted cytokines are multifarious, wherein both IL-4 and IL-13 induce alternative activation of APCs which are affiliated with rampant fungal growth. Th 17, conversely, is another subset of CD4 T helper cells, but are distinctly different from both Th1 and Th2 cells [41, 42, 43, 44, 45, 46, 47, 48]. Th 17 lineage is differentiated quite uniquely, and requires certain cytokines and transcription factors for their specific expression, mainly of which are IL-17A, IL-17F, and IL-22. TGF-β and IL-6 are the prime factors of differentiation that sets Th 17 exclusive from Th1 and Th2 [46, 48]. There are two dedicated mechanisms that the Th17 cells use to potent antimicrobial activity against fungal pathogens. First, these cells recruit neutrophils by the release of CXC chemokines, which in turn exhibit specific anti-Candida activity and inhibit that pathogen. Secondly, Th17 cells signal the release of antimicrobial peptides (AMPs) like S100A proteins, β-defensins, and histatins from epithelial cells and keratinocytes that display direct specific killing mechanisms. The last subset of T helper cells, i.e. Treg cells are significant in limiting the collateral damage in the body due to the extensive battle between the host and pathogen [46]. They dampen the responses via the secretion of cytokines like IL-10, TGF-β, or IL-35, and by many more inhibiting mechanisms.CD8 cytotoxic T cells are vital for potent activity against viruses and tumors, but their participation against fungal pathogens is not yet comprehensive and proven [45, 48, 49]. Owing to this, the activity of CD8 T cells against fungal pathogenesis needs to be confirmatory evaluated. In comparison to the process of antigen presentation and activation of T cells, the activity of B cells is more direct with its action against fungal antigens with the help of secretion of immunoglobulins under the influence of the fungal infection [50]. In general, immunoglobulin’s or antibodies elicit their defense responses by targeting dominant antigens of the pathogen like the fungal cell wall containing β-glucan, mannoproteins, agglutinin-like sequences (ALS),glucuronoxylomannan, and heat shock protein 60/90. These mechanisms are vaguely divided as either direct or indirect - based on their mode of action [50], [51]. By strict definition, the direct mechanism contributes to the direct binding of the Igs to the pathogen resulting in arrest, inhibition of growth, or microbiocidal activity. The indirect mechanism involves the activation of immunoglobulin- mediated pathways like ADCC. ADCC induces the destruction of fungal cells with the help of antibodies secreted by B cells, triggering innate responses like phagocytosis, and apoptosis [50, 51, 52]. The diagrammatic representation of the same has been represented in (Figure 2).
Immunization Against Candida: Vaccines
Over the last decades, there are various studies in the field of medical mycology that focus on the development of new immunization practices against invading fungal pathogens. Several apropos articles and papers have been published giving insight on new strategies, challenges, and necessity to the development of invasive antifungal vaccines [53, 54, 55, 56, 57, 58, 59, 60, 61, 62]. But not even one vaccine is present for the strains of Candida spp. This sudden increase in interest is because of the rise in mortality rates by lethal systemic fungal infections, especially in immunocompromised patients, premature infants, cancer patients and those with invasive treatments for long periods in hospital settings, which are known as high-risk groups [9, 63]. For such infections, standard antifungals have been issued and approved by the FDA that impart efficacy in almost successfully inhibiting the infection. Such treatments improve patient’s survival rates to a high point, but also affect the innate barrier of the host, even highly impacting the strength of the immune system, leading to high chance of acquiring infections caused by these pathogenic fungal strains [9, 64].
Hence, the development of new treatments by antifungal drugs, especially those that are affected by, and affect aggressive immunosuppressive therapies will continue to rise and increase the rate of deaths due to invasive fungal infections [9, 63]. The surfacing crisis of Invasive Fungal infections (IFI), especially those with Candida species has created the growing need to clarify defense strategies against fungi with the ultimate goal of therapeutic intervention [2, 5, 9, 23, 65]. Immunization methods against fungi are severely under-researched compared to bacterial and viral diseases. Due to its uncommonness and available treatment, fungal diseases are generally neglected and major vaccination priorities are shifted to other pathogenic microbes [2]. However, sufficient antifungal elements are not available in the market, and among them also most of them are not 100% accurate and efficient due to the fungi and yeast’s ability to resist its mode of action and still continuously replicating both in vitro and in vivo. The main goal of an efficient antifungal vaccine is to evoke a strong immune response that leads to immunological memory and consecutive protection against a recurrent exposure to those fungal pathogens [9, 61, 66, 67]. Fungal pathogens dwell on the surface of the host for months before showing any sign of infection. Even some accumulate inside various tissues of the host to evade the immune system and cause serious invasive infection. A tabular representation of the current targets for vaccination against Candida species is discussed in (Table 2).
| Candida species | Vaccine | Antigen Used | Adjuvant | Phase | Outcome | References |
|---|---|---|---|---|---|---|
| C. auris | NDV-3A | Recombinant Als3p protein | Alum | Pre-clinical Phase | Vaccine injected mice generated high titre anti-Als3p Abs that recognized Candida auris. Induced robust cross-reactive antibodies. Induced CD4+ T helper cells activation and immune response, biased with higher Th2 and Th17 subset activity. | [68-71] |
| In silico multivalent epitope- based vaccine | Als3p | RS09,Flagellin | Immuno- informatics | Vaccine construct predicted to be stable, soluble, highly antigenic, non-toxic, and non-allergenic. | [62,68,69] | |
| C. albicans | NDV-3A | Recombinant Als3p protein | Aluminum hydroxide in PBS | Pre-Clinical Phase+ Phase 1a/1b | Pre-clinical phase showed effective protection from oropharyngeal, vaginal and intravenous infection of Candida albicans. Human trials revealed generation of Anti-Als3p IgG and IgA at high peaks. Seroconversion seen in all vaccinated human subjects. Induced the production of Peripheral Blood Mononuclear Cells (PBMCS) OF IFN-γ and IL-17A. Induced T cell immune response in all subjects. Reduced frequency of Recurrent Vulvovaginal Candidiasis (RVVC) | [9,67,68] |
| PEV7 | Truncated recombinant secreted aspartic protease 2 (SAP2) | rSap2p plus virosome adjuvant | Phase 1 | Phase 1 showed evidence of strong immune response detected in vaginal and cervical samples. Volunteering patients showed a mucosal immune response with constant high titers across the chosen group. Effective in clearing the infection without any adverse effects. The results were more specific and robust with high dosage than those yielded with low dosage of the vaccine. | [62,69] | |
| C. glabrata | Immuno- informatic epitope- based vaccine | Fba1 (Fructose biphosphate aldolase protein) | No adjuvant used | Pre analytical Phase + Analytical Phase + Post- analytical Phase | Immunoinformatic revealed 11 effective epitopes for B cells. Predicted that the peptides QTSNGGAAY and LFSSHMLDL are the best Candidates for designing epitope-based vaccine against C. glabrata. Result had high specificity, safe, less time consuming, non-toxic, less allergic, and more antigenic. | [62,69,72] |
| Peptide- based Dendritic Cell vaccine | Peptide from C. tropicalis cell wall protein - Met6 | No adjuvant used | Pre-clinical Phase | DC vaccination induced substantial immunity in immunosuppressed mice. Substantial reduction of fungal burden (CFU count) in kidney and brain as compared to normal controls. | [73] | |
| C. tropicalis | Peptide- based Dendritic Cell vaccine | Cell surface protein – 5 methyltetra hydropter oyltriglutamate | No adjuvant used | Pre-clinical Phase | DC vaccination induced substantial immunity in immunosuppressed mice. Substantial reduction of fungal burden (CFU count) in kidney and brain as compared to normal controls. | [73] |
Table 2: Targets for vaccination against Candida species for immunization against Invasive Candidiasis.
Candida albicans
C. albicans being the most studied causative agent for IC. It is one of the Candida sp which gets placed in the critical priority group of WHO. It has a few current strategies for its effective suppression through vaccinations. The current known inhibition strategy involves the suppression of lanosterol 4-α-demethylase, further inhibiting ergo sterol synthesis in the endoplasmic reticulum [62]. Agglutinin-like sequence (Als) proteins are cell surface proteins that help in inhibition of Candida species by blocking fungal cell adhesion to biotic and abiotic surfaces for further invasion, and biofilm formation. Several Als proteins such as Als1, Als2, Als3, Als7 have been studied for treatment of fungal infections. One study involving the recombinant Als1 protein revealed a 50–57% increased survival rate in immunocompromised and immunosuppressed mice models [63]. This vaccine, given via intraperitoneal and subcutaneous routes both gave successful results of effective inhibition of C. albicans disseminated infection in mice models. Another study of 2019 [67], used the rAls3 N-terminus protein conjoint with aluminum hydroxide, and showed evidence of generation of anti-Als3p antibodies against C. albicans. Additionally, a new vaccine developed by Pevion Biotech is a virosomal vaccine that gives evidence of a strong response in vaginal and cervical samples added to a strong mucosal immune response as well [68, 69, 70].
Candida auris
Since the last decade, C. auris is gradually becoming a notorious superbug that has also achieved its position in the critical priority group of WHO FPPL 2022. After its detection from a Japanese patient’s ear canal in 2009, C. auris has traveled around the world, spreading and causing life- threatening infection in immunocompromised patients in clinical and hospital settings [74, 75, 76]. C. auris can be easily transmitted within hospitals; its patients and the persistence of this yeast on both abiotic surfaces like catheter tubes, hospital beds, curtains, etc. and also on biotic surfaces like epithelial tissues of skin and organs make this pathogen as deadly as any other bacterial nosocomial organism like Staphylococcus aureus [77, 78, 79, 80]. Owing to this, C. auris spreads to prime organs of the body through the bloodstream, causing IC [75, 76, 81]. The mortality rate at the beginning was said to be around 33%, but the extensive prevalence has raised the stakes to 55-60% [74, 75, 76, 81, 82, 83, 84, 85, 86]. WHO mentions mortality rate of IC caused by C. auris ranges from 29-53%. Even the hospital stays of patient infected increases from 68 days to 140 days. In the past decade, Candida auris isolates have been differentiated into four distinct clades based on pathogenicity and distribution across the globe- Clade I (South Asian), Clade II (East Asian), CladeIII (South African), and Clade IV (South American) [74, 84, 85]. There has also been speculation and discussion for a fifth clade containing isolates of Iran as well. C. auris is shown to be resistant to nearly all classes of antifungal classes- azoles, polyenes, and Echinocandins; and extreme efforts are being made for battling this problem. To date, there has been some published research regarding the immunology of C. auris done in animal models like Galleria mellonella, mammals and murine models [87, 88, 89].
Several ideas and experiments have been put forward to treat IC caused by Candida auris. One study carries forward the results of the NDV vaccine against C. albicans to check whether Als3p is effective in immunocompetent mice with Candida auris infection. The NDV-3A vaccine against C. auris proved to be efficient in inhibiting C. auris infection and increasing the survival rates to up to 40% by day 7 [71]. A bioinformatics approach with the same Als3p was apprehended with flagellin, which in turn demonstrated to be non-toxic and safe to use [68].
Candida Glabrata
C. glabrata is not a polymorphic microbe, but like other non-albican species, it causes life-threatening invasive infections in the human body and for that reason it has taken the position inhigh priority group with mortality rate ranging from 20 -50%. It grows as a yeast, and love macrophages as their main cell to attack. C. glabrata is known to infect and attack macrophages by modifying its phagosomal compartment, avoiding full maturation and acidification, hence preventing the phagosomal environment formation. The most common treatment used against C. glabrata are Echinocandins that inhibit beta - glucan synthetize, hence inhibiting cell wall synthesis [90]. Mannoproteins present in C. glabrata and C. albicans are evident to be homologous in great aspects, giving it an opportunity for greater thought and extra attention. One such yeast cell wall protein present in both species is called Fba1 which is an important enzyme for the glycolytic pathway. An epitope-based peptide vaccine has been developed using this enzyme as the potential antifungal target [72]. There have been several vaccines that used Fba1 as an immunogenic protein against pathogens like Salmonella spp, S. pneumonia, and M. bovis as well.
Discussion
Infectious disease which mainly focuses on bacterial infection, the main cause is considered to be antimicrobial resistance. But in the past decade and during the Covid-19 pandemic the prevalence of deadly Invasive Fungal Infections (IFIs) has drastically augmented with doubts regarding its efficient treatment, developing resistance against antifungal which is nearly 38% of the total fungal infection (WHO FPPL). These complications have raised the urgency to develop new therapeutics through effective immunization [3, 4]. With WHO publishing its first fungal pathogen priority list and mentioning the need of a vaccine against Candida sp. This permutes the main focus on immunosuppression therapies.
The prime idea of therapy is believed to give immunization by vaccinations for proper protection of immune memory in advance [91]. The existing antifungals like Echinocandins, azoles, fluconazole, amphotericin B, Voriconazole, itraconazole, flucytosineare generally used against Candida spp. But they show a higher MICs and even some are ineffective against some. All these antifungal agents come with tremendous after effect on the host. Research on fungal diseases is being acutely submerged under the influence of other bacterial and viral diseases; this review puts further pressure on the gravity of this topic. Nevertheless, much of the knowledge used for research on such bacterial and viral diseases has been transferred for its appropriate use against fungal infections. There has been vast progress in our comprehension of immunology to fungal pathogens, and the generation of strategies for successful fungal immunization [21].
Candida albicans is the most common species of the genus, and there have been many immunization efforts against this pathogen, both locally and systemically, including the PEV7 vaccine that showed effective immunization and protection against vulvovaginitis (VVC) in pregnant women in the study, and NDV-3A which revealed safe immunization of subjects and substantial decrease of the fungal burden of Candida species. Even with this, the incidence and prevalence of C. albicans is ample and constantly rising. Commercialization and further human trials should be supported for the availability of the vaccine to common public to curb the infection down. On the same line, C. auris is an emerging Multi-drug Resistant (MDR) pathogen that affects immunosuppressed patients and it has become resistant to most of the available groups of antifungal drugs. Hence, immunization through vaccinations for invasive fungal infections is in great demand and appropriate. Candida auris has been studied for vaccine development, and a preclinical study with mice has been done that showed a successful decrease in yeast cell growth, inhibition of replication, and induction of effective T and B cell immune response against the pathogen. To sum up, a great deal of effort should be continued to be made in response to invasive fungal disease treatment and powerful immune response guarantee through vaccinations.
When Candida albicans causes localized infections, antifungals are sufficient. Vaccination against C. auris is inadequate and needs more focus, and the effort is being made by several researchers. In vitro activities and experiments are ample, and the main anchor of research should be in vivo experiments recording real-time observations of the mammalian body. Clinical trials of the current vaccinations of Candida species are limited, and further phases and experiments should be continued with safe and effective doses with proper FDA approval. To date, there have been no fungal vaccines cleared for prescription use; however, several experimental models exist. In short, more effort needs to be put forward into giving fungal infections its correct attention.
Acknowledgments
We thank My lab Discovery Solutions for providing the necessary facilities and the opportunity for Carrying out this review.
References
-
Garcia Rubio R, Oliveira HC, Rivera J, Trevijano Contador N (2020) The Fungal Cell Wall: Candida, Cryptococcus, and Aspergillus Species. Front Microbiol 10: 2993.
-
F Bongomin, S Gago, R Oladele, D Denning (2017) Global and Multi-National Prevalence of Fungal Diseases Estimate Precision. Journal of Fungi 3(4,): 57.
-
Borgio JF, Rasdan AS, Sonbol B, Alhamid G, Almandil NB, et al. (2021) Emerging Status of Multidrug-Resistant Bacteria and Fungi in the Arabian Peninsula. Biology Basel 10(11): 1144.
-
Chowdhary A, Sharma C, Meis JF (2017) Candida auris: A rapidly emerging cause of hospital-acquired multidrug- resistant fungal infections globally. PLoS Pathog 13(5): e1006290.
-
Sallusto F, Lanzavecchia A, Araki K, Ahmed R (2010) From Vaccines to Memory and Back. Immunity 33(4): 451-463.
-
Wasylyshyn AI, Linder KA, Kauffman CA, Richards BJ, Maurer SM, et al. (2021) Invasive Fungal Disease in Patients with Newly Diagnosed Acute Myeloid Leukemia. Journal of Fungi 7(9): 761.
-
Marques L, Araujo O, Silva A, Bourguignon DS, Carlesse F, et al. (2020) A survival analysis of invasive fungal diseases in children with cancer. J Pediatr Infect Dis 16(5): 237-241.
-
Bhatt VR, Viola GM, Ferrajoli A (2011) Invasive fungal infections in acute leukemia. Therapeutic Advances in Hematology 2(4): 231-247.
-
Medici NP, Poeta MD (2015) New insights on the development of fungal vaccines: from immunity to recent challenges. Mem Inst Oswaldo Cruz 110(8): 966-973.
-
Aranda-Audelo M, Rivera-Martínez NE, Corzo-León DE (2018) Characteristics of invasive fungal infections among hiv individuals from an indigenous origin in Mexico. Journal of Fungi 4(3): 109.
-
Armstrong-James D, Meintjes G, Brown GD (2014) A neglected epidemic: fungal infections in HIV/AIDS. Trends Microbiol 22(3): 120-127.
-
Del Poeta M, Casadevall A (2012) Ten Challenges on Cryptococcus and Cryptococcosis,” Mycopathologia 173(5-6): 303-310.
-
J Perlroth, B Choi, B Spellberg (2007) Nosocomial fungal infections: Epidemiology, diagnosis, and treatment. Medical Mycology 45(4): 321-346.
-
R M Roy, B S Klein (2012) Dendritic Cells in Antifungal Immunity and Vaccine Design. Cell Host Microbe 11(5): 436446.
-
C Spampinato, D Leonardi (2013) Candida infections, causes, targets, and resistance mechanisms: Traditional and alternative antifungal agents. BioMed Research International 1-13.
-
Pfaller MA, Diekema DJ (2007) Epidemiology of Invasive Candidiasis: a Persistent Public Health Problem. Clin Microbiol Rev 20(1): 133-163.
-
F L Mayer, D Wilson, B Hube (2013) Candida albicans pathogenicity mechanisms. Virulence 4(2): 119-128.
-
L Pagano, S Mayor (2018) Invasive fungal infections in high-risk patients: report from TIMM-8 2017. Future Sci OA 4(6): FSO307.
-
N Alkharashi, Aljohani S, Layqah L,Masuadi E, Baharoon W, et al. (2019) Candida Bloodstream Infection: Changing Pattern of Occurrence and Antifungal Susceptibility over 10 Years in a Tertiary Care Saudi Hospital. Can J Infect Dis Med Microbiol 1-9.
-
D H Van Thiel, M George, C M Moore (2012) Fungal Infections: Their Diagnosis and Treatment in Transplant Recipients. Int J Hepatol 1-19.
-
M C Fisher, Sarah J Gurr, Christina A Cuomo, David S Blehert, Hailing Jin, et al. (2020) Threats Posed by the Fungal Kingdom to Humans, Wildlife, and Agriculture. MBio 11(3).
-
E Klaile, Mario M Müller, Cristina Zubiria Barrera, Saskia Brehme, Tilman E Klassert, et al. (2019) Unaltered Fungal Burden and Lethality in Human CEACAM1 Transgenic Mice During Candida albicans Dissemination and Systemic Infection. Front Microbiol10: 02703.
-
Ben E de Pauw (2011) what are fungal infections? Mediterr J Hematol Infect Dis 3(1): e2011001.
-
F C Kotey, N T Dayie, P B Tetteh-Uarcoo, E S Donkor (2021) Candida Bloodstream Infections: Changesin Epidemiology and Increase in Drug Resistance. Infectious Diseases: Research and Treatment 14.
-
M A Pfaller, D J Diekema (2007) Epidemiology of invasive candidiasis: A persistent public health
-
Problem. Clinical Microbiology Reviews 20(1): 133-163.
-
M Slavin, J Fastenau, I Sukarom, P M avros, S Crowley, et al. (2004) Burden of hospitalization of patients with Candida and Aspergillus infections in Australia. International Journal of Infectious Diseases 8(2): 111- 120.
-
C Moran, C A Grussemeyer, J R Spalding, D K Benjamin, S D Reed (2010) Comparison of costs, length of stay, and mortality associated with Candida glabrata and Candida albicans bloodstream infections. Am J Infect Control 38(1): 78-80.
-
LS Wilson, C M Reyes, M Stolpman, J Speckman, K Allen, et al.(2002)The Direct Cost and Incidence of Systemic Fungal Infections. Value in Health 5(1): 26-34.
-
AL Colombo, J Perfect, M DiNubile, K Bartizal, M Motyl, et al. (2003) Global Distribution and Outcomes for Candida species Causing Invasive Candidiasis: Results from an International Randomized Double-Blind Study of Caspofungin Versus Amphotericin B for the Treatment of Invasive Candidiasis. Eur J Clin Microbiol Infect Dis 22(8): 470-474.
-
J Guinea (2014) Global trends in the distribution of Candida species causing candidemia,” Clinical
-
Microbiology and Infection 20(6): 5-10.
-
MA Pfaller, DJ Diekema, RN Jones, S A Messer, R J Hollis (2002) Trends in Antifungal Susceptibility of Candida spp. Isolated from Pediatric and Adult Patients with Bloodstream Infections: SENTRY Antimicrobial Surveillance Program, 1997 to 2000. J Clin Microbiol 40( 3): 852-856.
-
F Barchiesi, E Orsetti, R Gesuita, E Skrami, E Manso (2016) Epidemiology, clinical characteristics, and outcome of candidemia in a tertiary referral center in Italy from 2010 to 2014. Infection 44(2): 205-213.
-
Z. T. Yang, Lin Wu, Xiao Ying Liu, Min Zhou, Jie Li, et al. (2014) Epidemiology, species distribution and outcome of nosocomial Candida spp. Bloodstream infection in Shanghai. BMC Infect Dis 14(1).
-
N F Aldardeer, Hadiel Albar, Majda Al Attas, Abdelmoneim Eldali, Mohammed Qutub, et al. (2020) Antifungal resistance in patients with Candidaemia: a retrospective cohort study. BMC Infect Dis, 20(1): 55.
-
O DoGan, Aysegul Yesilkaya, sirin Menekse, ozlem Guler, Cagla Karakoc, et al.(2020) Effect of initial antifungal therapy on mortality among patients with bloodstream infections with different Candida species and resistance to antifungal agents: A multicenter observational study by the Turkish Fungal Infections Study Group. Int J Antimicrob Agents 56(1): 105992.
-
M Bedard, R A Drummond (2018) Immune responses to fungal pathogens Category: Pathogens and Disease. British Society for Immunology pp9.
-
L Romani (2004) Immunity to fungal infections. Nat Rev Immunol 4(1): pp. 11-24.
-
Gordon D Brown, M G Netea (2007) Immunology of fungal infections.
-
S Jiang (2016) Immunity against Fungal Infections. Immunol Immunogenet Insights 8.
-
S W Brubaker, K S Bonham, I Zanoni, J C Kagan (2015) Innate immune pattern recognition: A cell biological perspective. Annual Review of Immunology 33(1): 257- 290.
-
B Pathakumari, G Liang, W Liu (2020) Immune defence to invasive fungal infections: A comprehensive review. Biomedicine & Pharmacotherapy 130: 110550.
-
J V Desai, M S Lionakis (2018) the Role of Neutrophils in Host Defense Against Invasive Fungal Infections. Curr Clin Microbiol Rep 5(3): 181-189.
-
MG Netea, LAB Joosten, JWM van der Meer, BJ Kullberg, FL van de Veerdonk (2015) Immune defence against Candida fungal infections. Nat Rev Immunol 15(10): 630-642.
-
M Wüthrich, GS Deepe, B Klein (2012) Adaptive immunity to fungi. Annual Review of Immunology 30(1): 115-148.
-
Kumaresan PR, da Silva TA, Kontoyiannis DP (2018) Methods of Controlling Invasive Fungal Infections Using CD8+ T Cells. Front Immunol 8: 1939.
-
Van De Veerdonk FL, Netea MG (2010) T-cell subsets and antifungal host defenses. Current Fungal Infection Reports 4(4): 238-243.
-
Shoham S, Levitz SM (2005) The immune response to fungal infections. Br J Haematol 129(5): 569-582.
-
Romani L (2008) Cell mediated immunity to fungi: A reassessment. Medical Mycology 46(6): 515-529.
-
Wüthrich M, Filutowicz HI, Warner T, Deepe GS, Klein BS (2003) Vaccine immunity to pathogenic fungi overcomes the requirement for CD4 help in exogenous antigen presentation to CD8+ T cells: Implications for vaccine development in immune-deficient hosts. J Exp Med 197(11): 1405-1416.
-
Diamond RD (1989) Immune Response to Fungal Infection. Rev Infect Dis 11 Suppl 7: S1600-S1604.
-
Khanna N, Stuehler C, Lünemann A, Wójtowicz A, Bochud P, et al. (2016) Host response to fungal infections – how immunology and host genetics could help to identify and treat patients at risk. Swiss Med Wkly 146: w14350.
-
Salazar F, Brown GD (2018) Antifungal Innate Immunity: A Perspective from the Last 10 Years. J Innate Immun 10( 5-6): 373-397.
-
Deepe GS (1997) Prospects for the development of fungal vaccines. Clin Microbiol Rev 10(4): 585-596.
-
Cassone A (2008) Fungal vaccines: real progress from real challenges. Lancet Infect Dis 8(2): 114-124.
-
Assis-Marques MA, Oliveira AF, Ruas LP, dos Reis TF, Roque-Barreira MC, et al. (2015) Saccharomyces cerevisiae Expressing Gp43 Protects Mice against Paracoccidioides brasiliensis Infection. PLoS One 10(3): e0120201.
-
Edwards JE (2012) Fungal cell wall vaccines: An update. Journal of Medical Microbiology 61(Pt 7): 895-903.
-
de Almeida JRF, Kaihami GH, Jannuzzi GP, de Almeida SR (2015) Therapeutic vaccine using a monoclonal antibody against a 70-kDa glycoprotein in mice infected with highly virulent Sporothrix schenckii and Sporothrix brasiliensis. Med Mycol 53(1): 42-50.
-
Torosantucci A, Bromuro C, Chiani P, De Bernardis F, Berti F, et al. (2005) A novel glyco-conjugate vaccine against fungal pathogens. Journal of Experimental Medicine 202(5): 597-606.
-
de Amorim J, Magalhães A, Muñoz JE, Rittner GMG, Nosanchuk JD, et al. (2013) DNA vaccine encoding peptide P10 against experimental paraCoccidioidomycosis induces long-term protection in presence of regulatory T cells. Microbes Infect 15(3): 181-191.
-
Iannitti RG, Carvalho A, Romani L (2012) From memory to antifungal vaccine design,” Trends Immunol 33(9): 467-474.
-
Piccione D, Mirabelli S, Minto N, Bouklas T (2019) Difficult but Not Impossible: in Search of an Anti-Candida Vaccine. Tropical Mycoses 6(2): 42-49.
-
Spellberg BJ, Ibrahim AS, Avenissian V, Filler SG, Myers CL, et al. (2005) the anti-Candida albicans vaccine composed of the recombinant N terminus of Als1p reduces fungal burden and improves survival in both immunocompetent and immunocompromised mice. Infect Immun 73(9): 6191-6193.
-
Paramythiotou E, Frantzeskaki F, Flevari A, Armaganidis A, Dimopoulos G (2014) Invasive Fungal Infections in the ICU: How to Approach, How to Treat. Molecules 19(1): 1085-1119.
-
Naglik JR (2014) Candida Immunity. New Journal of Science 2014: 1-27.
-
Nanjappa SG, Klein BS (2014) Vaccine immunity against fungal infections. Curr Opin Immunol 28(1): 27-33.
-
Alqarihi A, Singh S, Edwards JE, Ibrahim AS, Uppuluri P (2019 )NDV-3A vaccination prevents C. albicans colonization of jugular vein catheters in mice. scientific reports 9(1): 6194.
-
Tso GHW, Reales-Calderon JA, Pavelka N (2018) The Elusive Anti-Candida Vaccine: Lessons From the Past and Opportunities for the Future. Front Immunol 9: 897.
-
Wang XJ, Sui X, Yan L, Wang Y, Cao YB, et al. (2015) Vaccines in the treatment of invasive candidiasis. Virulence 6(4): 309-315.
-
Tarang S, Kesherwani V, LaTendresse B, Lindgren L, Rocha-Sanchez SM, et al. (2020) In silico Design of a Multivalent Vaccine Against Candida albicans. Scientific reports 10(1): 1066.
-
Singh S, Uppuluri P, Mamouei Z, Alqarihi A, Elhassan H, et al. The NDV-3A vaccine protects mice from multidrug resistant Candida auris infection. PLoS Pathog 15(8): e1007460.
-
Elamin Elhasan LM, Hassan MB, Elhassan RM, Abdelrhman FA, Salih EA, et al. (2021) Epitope-Based Peptide Vaccine Design against Fructose Bisphosphate Aldolase of Candida glabrata: An Immunoinformatics Approach. J Immunol Res 2021: 8280925.
-
Xin H (2019) Effects of immune suppression in murine models of disseminated Candida glabrata and Candida tropicalis infection and utility of a synthetic peptide vaccine. Med Mycol 57(6): 745-756.
-
Du H, Bing J, Hu T, Ennis CL, Nobile CJ, et al. (2020) Candida auris: Epidemiology, biology, antifungal resistance, and virulence. PLoS Pathog 16(10): e1008921.
-
Osei Sekyere J (2018) Candida auris : A systematic review and meta-an alysis of current updates on an emerging multidrug-resistant pathogen. Microbiologyopen 7(4): e00578.
-
Vila T, Sultan AS, Montelongo-Jauregui D, Jabra-Rizk MA (2020) Candida auris: a fungus with identity crisis. Pathog Dis 78(4): ftaa034.
-
Dranginis AM, Rauceo JM, Coronado JE, Lipke PN (2007) A Biochemical Guide to Yeast Adhesins: Glycoproteins for Social and Antisocial Occasions. Microbiol Mol Biol Rev 71(2): 282-294.
-
Tronchin G, Pihet M, Lopes-Bezerra LM, Bouchara JP (2008) Adherence mechanisms in human pathogenic fungi. Med Mycol 46(8): 749-772.
-
Welsh RM, Bentz ML, Shams A, Houston H, Lyons A, et al. (2017) Survival, Persistence, and Isolation of the Emerging Multidrug-Resistant Pathogenic Yeast Candida auris on a Plastic Health Care Surface. J Clin Microbiol 55(10): 2996-3005.
-
Lockhart SR, Berkow EL, Chow N, Welsh RM (2017) Candida auris for the Clinical Microbiology Laboratory: Not Your Grandfather’s Candida species. Clin Microbiol 39(13): 99-103.
-
L Rossato, A L Colombo (2018) Candida auris: What Have We Learned About Its Mechanisms of Pathogenicity?. Front Microbiol 9: 03081.
-
M Kordalewska, D S Perlin (2019) Identification of Drug Resistant Candida auris. Front Microbiol 10: 01918.
-
R Sabino, C Veríssimo, AA Pereira, F Antunes (2020) Candida auris, An Agent of Hospital-Associated Outbreaks: Which Challenging Issues Do We Need to Have in Mind? Microorganisms 8(2): 181.
-
F Chaabane, A Graf, L Jequier, A T Coste (2019) Review on Antifungal Resistance Mechanisms in the Emerging Pathogen Candida auris. Frontiers in Microbiology 10: 02788.
-
A W de Jong, F Hagen (2019) Attack, Defend and Persist: How the Fungal Pathogen Candida auris was Able to Emerge Globally in Healthcare Environments. Mycopathologia 184(3): 353-365.
-
M A Sayeed, J Farooqi, K Jabeen, S Awan, S F Mahmood (2019) Clinical spectrum and factors impacting outcome of Candida auris: A single center study from Pakistan. BMC Infect Dis 19(1): 384.
-
A Hernando Ortiz, E Mateo, A Perez-Rodriguez, P W J de Groot, G Quindós, et al. (2021) Virulence of Candida auris from different clinical origins in Caenorhabditis elegans and Galleria mellonella host models. Virulence 12(1): 1063-1075.
-
H Xin, F Mohiuddin, J Tran, A Adams, K Eberle (2019) Experimental Mouse Models of Disseminated Candida auris Infection. msphere 4(5).
-
D Romera, Aguilera Correa JJ, GarcIaCoca M, Mahillo FernAndez I, Vinuela Sandova L, et al. (2020) The Galleria mellonella infection model as a system to investigate the virulence of Candida auris strains. Pathog Dis 78(9): 067.
-
D S Perlin (2015) Echinocandin Resistance in Candida. Clinical Infectious Diseases 61(6): S612-S617.
-
A Carvalho, C Duarte Oliveira, SM Goncalves, A Campos, JF Lacerda, C Cunha (2017) Fungal Vaccines and Immunotherapeutics: Current Concepts and Future Challenges. Curr Fungal Infect Rep11 (1): 16-24.
-
A. Carvalho, Cristina Cunha, Rossana G Iannitti, Andrea Casagrande, Francesco Bistoni, et al. (2012) Host defense pathways against fungi: The basis for vaccines and immunotherapy. Frontiers in Microbiology 3: 176.
- Diversity of Candida sp and Antifungal Susceptibility Patterns in Digestive Candidiasis among People Living with HIV in CHU of Libreville, Gabon
- Vulvovaginal candidiasis: Retrospective study (2019- 2021) at the Centre Hospitalier National de Pikine, Suburban Dakar, Senegal
- Identification of Environmental Fungal Species in Clinical Services of University Hospital of Angre, Abidjan (Cote d’Ivoire)
- New Location of some Gasteroid Basidiomycetes in Western Kazakhstan
- Evaluation of Various Extracellular Enzymes of Ectomycorrhizal Mushrooms
- Morphology and Phylogeny of Lactarius Wallichianae sp. nov and Xerula magnispora sp. nov. from India