Combined Surgical Approach in a Late Case of Orbital Cellulitis
Introduction
Orbital cellulitis is a potentially life-threatening but uncommon ophthalmic emergency characterised by infection of the soft tissues behind the orbital septum [1]. As such, rapid diagnosis and prompt initiation of therapy, medical and/or surgical, are important in order to minimize complications and optimize outcomes. Mucocele is a chronic, expanding, mucosa-lined lesion of the paranasal sinus characterized by mucous retention that can become infected forming a mucopyocele [2]. A mucopyocele when extends into the orbit, can present as acute orbital cellulitis, as was the case in our patient [3]. The management of orbital cellulitis is primarily medical with prompt initiation of intravenous antibiotics. Surgical intervention should be considered in patients who fail to respond or deteriorate on medical therapy, display worsening visual function/pupillary changes, or develop an orbital abscess, particularly in those cases in which the primary cause requires surgery too. However it is recommended that the treatment approach should be case based [4]. We describe a case of late presentation of acute orbital cellulitis subsequent to a frontoethmoidal mucopyocele extending into the orbit treated with a combined conventional external orbitotomy and newer endoscopic approach.
Case report
A 12-year-old female patient presented with progressive left eyelids swelling since 1 week. There was associated acute pain, redness along with downward and outward protrusion of the left eyeball. Patient complained of diplopia and mild diminution of vision in the left eye. Also there was history of fever with chills since 10 days and intermittent frontal headache since last 2 years. There was no history of projectile vomiting, nasal discharge or toothache. On local examination, there was fluctuant, erythematous, non-pulsatile, tender swelling in the upper eyelid of the left eye along with ptosis. The left eyeball was pushed inferiorly and laterally causing a proptosis of 26mm (Figure 1).

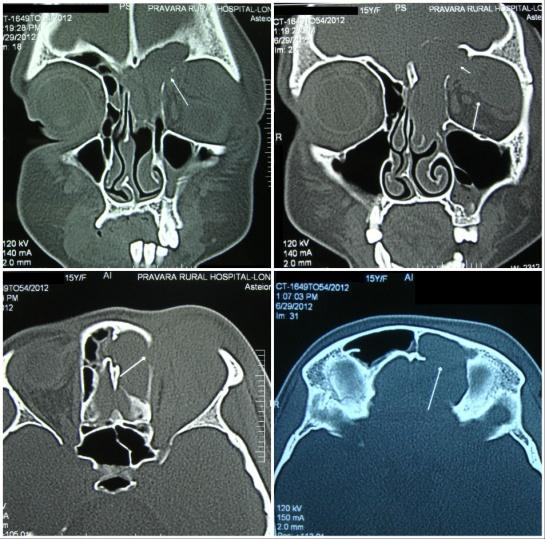
Vision was 6/12 in the left eye and ocular movements were painful and restricted in all gazes. On fundus examination, there was blurring of disc margins along with venous dilatation and tortuosity in the left eye. All the findings in the right eye were within normal limits. There was history of left sided endoscopic frontal sinus surgery 3 months back. A clinical diagnosis of acute orbital cellulitis was made. On contrast-enhanced CT scan, there was a large, expansile, cystic lesion arising from the left frontal and ethmoid air cells extending into left retrobulbar space destroying the lamina papyracea, posterior wall of frontal sinus and eroding the floor of the anterior cranial fossa (Figure 2).
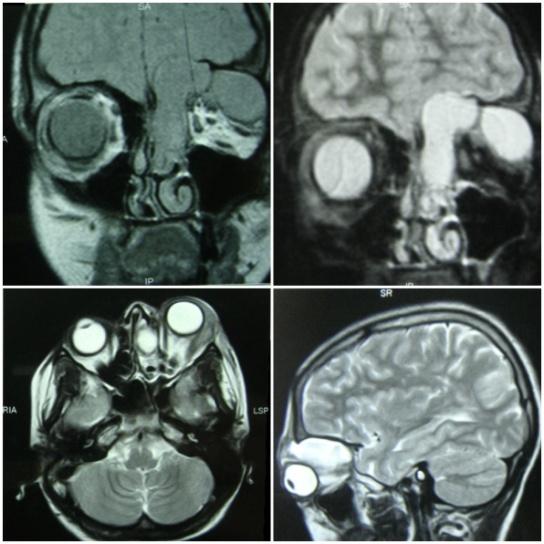
MRI scan suggested that the lesion was bi-loculated, the medial one in close proximity with the left frontal lobe of the brain and the lateral loculus extending into the orbit causing proptosis of the left eyeball (Figure-3).
We started the patient on intravenous amoxicillin and clavulanate potassium combination, amikacin and metronidazole along with anti-inflammatory and pain killers. In spite of starting the patient on intravenous antibiotics and anti-inflammatory, her visual acuity deteriorated to 6/36 in the left eye and there was colour vision defect on testing with Ishihara’s charts. There was worsening of proptosis to Hertel value of 30mm. Fundoscopy revealed choroidal folds and indentation of the superior hemisphere of the retina. The patient was planned for surgery. Firstly, endoscopic drainage of the medial loculus of the mucocoele was done along with marsupialization by the axillary flap technique. Subsequently, the external orbitotomy was done using the Benedict incision for complete drainage and removal of the lateral orbital loculus along with the mucosa. A Rains frontal sinus stent was used for stenting the frontal sinus during marsupialization and silicon drains were placed in the external orbitotomy incision. Both were removed subsequently after 12 weeks and 1 week respectively. Postoperatively, the patient received intravenous antibiotics to which she responded very well with steady decrease in proptosis, swelling and fever over the next seven days. Eyelid edema subsided fully after two weeks of treatment (Figure 4) with free and full movement of eyeball in all directions of gaze and normal colour vision along with normal visual acuity in the left eye. There were no choroidal folds on fundoscopy.

Discussion
Orbital cellulitis describes infections that involve the tissues posterior to the orbital septum within the bony orbit [5]. Orbital cellulitis affects all age groups but is more common in the adolescent population. The most frequent cause of orbital cellulitis is secondary extension of infection from the paranasal sinuses, particularly from the ethmoid sinus given the thin medial orbital wall. Other notable causes of orbital cellulitis include trauma with associated orbital fracture or foreign body, dacryocystitis, dental infections, and untreated preseptal cellulitis [6]. Mucoceles of the paranasal sinus are slowly expanding lesions which consist of accumulation of mucus and epithelial debris in the mucosa of the sinus subsequent to obstruction of the ostium of the sinus. They affect most commonly the frontal sinus. If there is acute infection of mucocele, leading to mucopyocele, there is higher likelihood of complications mainly orbital or intracranial [7]. In our case the frontoethmoidal mucopyocele had extended into the orbit causing acute orbital cellulitis and abscess formation. The globe itself was compressed superomedially, resulting in the development of chorioretinal striae. A progressive optic neuropathy from compression of the orbital portion of the optic nerve occurred as the mucocele expanded posteriorly to compress posterior orbital structures [8]. Given the potential for significant complications, intravenous antibiotics should be started promptly for all cases of orbital cellulitis [9]. Surgical drainage is considered in case of non-response to medical treatment, subperiosteal or orbital abscess formation, or presence of signs of optic neuropathy. The surgical drainage can be endoscopic alone, open drainage or combination of open and endoscopic drainage [10]. In our case, there were two abscess cavities with one abscess extending medially upwards towards the roof of the orbit and the other one spreading laterally and posteriorly into the retrobulbar space. Also there was history of previous sinus surgery. Because of the failure to medical therapy, worsening visual function, and presence of two large orbital abscesses, surgical intervention was done in our patient. We used the combined external and endoscopic approach to get a wide drainage of marsupialization of the medial abscess via the transnasal endoscopic approach and adequate excision of the lateral abscess via the external orbitotomy approach. The combined approach gave us an added advantage of treating the sinus pathology along with the abscess drainage, thus reducing the chances of recurrence. Ours is a case of very late presentation of acute orbital cellulitis having two separate orbital abscesses subsequent to frontoethmoidal mucopyocele. The nasal abscess was easily accessible through the nasal endoscopic method but the temporal one could not be drained through that route as it was a thick encapsulated loculus which was beyond the reach of the endoscopic approach. The uniqueness of this case is very late presentation, two separate abscess loculi which were treated successfully with two simultaneous different surgical approaches- transnasal endoscopic and external orbitotomy, resulting in complete recovery. In spite of being a relatively uncommon late presentation of frontoethmoidal mucopyocele, orbital cellulitis remains a potentially sight and life threatening infection that requires careful examination and prompt treatment. Through this article, we are laying emphasis on the fact that orbital abscess can have varied presentations depending upon the extent and complexity of the lesion, and hence, conventional preferred surgical approaches cannot be applied in all such cases. An individualized therapeutic approach should be undertaken for each case.
References
-
Chaudhry IA, Shamsi FA, Elzaridi E, Al-Rashed W, Al- Amri A, et al. (2007) Outcome of treated orbital cellulitis in a tertiary eye care center in the middle East. Ophthalmology 114(2): 345-354.
-
Suri A, Mahapatra AK, Gaikwad S, Sarkar C (2004) Giant mucoceles of the frontal sinus: a series and review. J Clin Neurosci 11(2): 214-218.
-
Giletto JB, Scherr SA, Mikaelian DO (1981) Orbital complications of acute sinusitis in children. Trans Pa Acad Ophthalmol Otolaryngol 34(1): 60-64.
-
Potter NJ, Brown CL, McNab AA, Ting SY (2011) Orbital Cellulitis: Medical and Surgical Management. J Clinic Experiment Ophthalmol S2:001.
-
Bergin DJ, Wright JE (1986) Orbital cellulitis. Br J Ophthalmol 70(3): 174-178.
-
Babar TF, Zaman M, Khan MN, Khan MD (2009) Risk factors of preseptal and orbital cellulitis. J Coll Physicians Surg Pak 19(1): 39-42.
-
Lund VJ, Rolfe ME (1989) Ophthalmic considerations in fronto-ethmoidal mucoceles. J Laryngol Otol 103: 667-669.
-
Fujitani T, Takahashi T, Asai T (1984) Optic nerve disturbance caused by frontal and fronto-ethmoidal mucopyoceles. Arch Otolaryngol 110: 267-269.
-
Suneetha N, Battu RR, Thomas RK, Bosco A (2000) Orbital abscess: Management and outcome. Indian J Ophthalmol 48(2): 129-134.
-
Aggarwal SK, Bhavana K, Keshri A, Kumar R, Srivastava A (2012) Frontal sinus mucocele with orbital complications: Management by varied surgical approaches. Asian J Neurosurg 7(3): 135-140.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report