Contact Lens Induced Papillary Conjunctivitis-Review and A Case Report from Nepal
Aim: To study a case of contact lens complication in the form of Contact lens induced papillary conjunctivitis. Methods: This was a case of a young contact lens user, using contact lenses in the department of Ophthalmology, Dhulikhel Hospital. A detail evaluation was carried out including personal details, chief complaints, vision screening, anterior segment evaluation and contact lens examination. Results: The patient was found to have Contact lens induced papillary conjunctivitis (CLPC). Conclusion: Unhygienic, mishandling and unawareness about contact lens wear may lead to vision threating complications.
Introduction
In 1974, Spring reported Contact lens papillary conjunctivitis (CLPC) for the first time and is explained as a reversible, inflammatory reaction of the upper palpebral conjunctiva (UPC) [1]. It is characterized by enlarged papillae >0.3 mm, palpebral hyperemia and mucus secretion [2, 3]. If the size of papillae is greater than 1.0 mm, then it is termed Giant papillary conjunctivitis (GPC). This condition is an inflammatory condition commonly seen in soft contact lens wearers, patients using ocular prosthesis and with exposed sutures after surgery. Though, CLPC is a reversible non-sight threatening condition, symptom like itching and ocular discomfort can lead to contact lens (CL) intolerance and discontinuation [4].
Literatures have shown variable incidence of CLPC and has been reported as between 1.5 and 47.5% [5]. This reported incidence has varied widely (0.4%–47.5%), depending on lens materials, lens type, wearing schedule, and lens care solutions used in each study [5, 6]. Boswell, et al. reported higher incidence of GPC in patients using extended conventional lenses (35%) than patients using extended disposable lenses (5%).
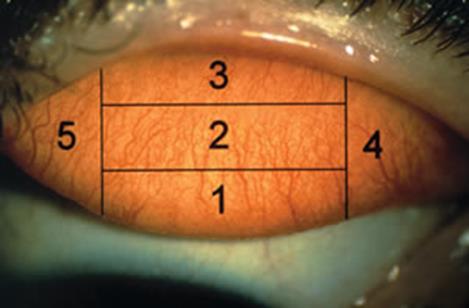
Two different presentations of CLPC have been reported. Allan smith, et al. separated the palpebral conjunctival area into 5 distinct zones (Figure 1) [2]. Secondly, the distribution of the papillae can be described in accordance with Holden et al. who suggested to separate CLPC into two different presentations; either ‘local’ or ‘general’. ‘Local CLPC’ is defined if papillae are confined to one or two areas of the upper palpebral conjunctiva and ‘general CLPC’ if papillae are scattered across three or more areas [7].
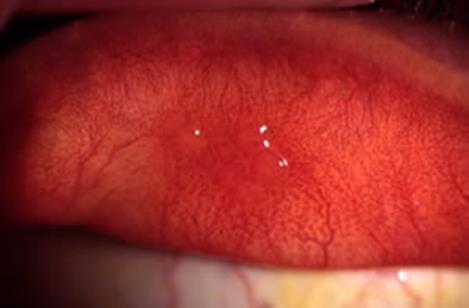
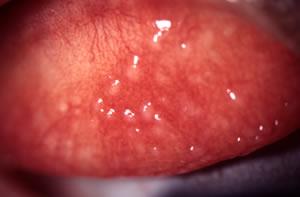
The enlarged papillae and hyperemia manifest most commonly in zones 2 and 3 of the UPC in local cases of CLPC (Figure 2), whereas, in general CLPC, the majority are observed in zones 1,2 and 3 and sometimes in zones 4 and 5 (Figure 3). The incidence of local CLPC (3.4%) is on higher range than general CLPC (1.2%) [8].
Etiology
The exact cause is not fully understood yet. It has multifactorial etiologies.
- Type I immediate hypersensitivity reaction (mediated by IgE ) • The probable antigens might be: - Altered host protein on contact lens/prosthesis/suture surface - Bacterial cell wall constituents - Other lens deposits/contaminants • Hypersensitivity reaction causes degranulation of mast cells • the products of degranulation stimulate recruitment of basophils and eosinophil to conjunctival epithelium
- Type IV delayed hypersensitivity reaction (mediated by T-cells) • It increases the inflammatory response
- Release of neutrophil chemotactic factor due to tarsal conjunctival surface trauma • Sources of trauma might be contact lenses, ocular prostheses, elevated corneal deposits
Predisposing Factors
- CLPC is more common in soft contact lens users compared to rigid lens users. o Reported in silicone hydrogel, as well as hydrogel, lens wearers
- Contact lens deposits, lens edges (thick or poorly designed or manufactured)
- Atopy
- Meibomian gland dysfunction (MGD)
Patient’s Particulars
Name: XYZ 24 years / Male Presenting VA (OU): 20/20 with contact lens Chief Complaints: Irritation/discomfort in the left eye which increased in intensity after lens removal since 1 month or so.
Contact Lens History/ General History
The patient had been evaluated in general eye OPD for routine eye exams since 2010. He was using Daily Wear conventional hydrogel contact lenses for 6 months (OU> BC- 8.60 mms / BVP= - 4.00 Ds / Diameter= 14.00 mms). He had a good compliance and followed proper care and maintenance regimen for his lenses and never slept with lens on. The patient was using lenses about 8-10 hours/day. His ocular and medical history was negative and he was not using any medications nor had any allergies.
Symptoms: The symptoms in this case were only with his left eye.
- Ropy/stringy discharge
- Severe itching after lens removal
- Foreign Body sensation/Discomfort under the upper lid
- Lens awareness due to increased lens movement
- Lens intolerance
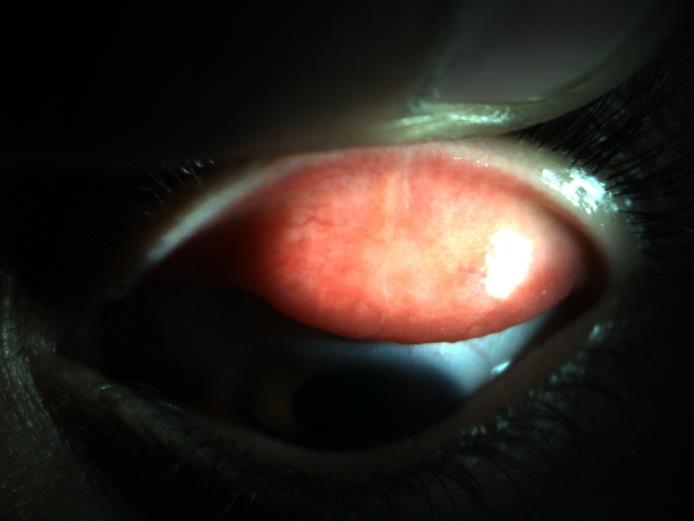
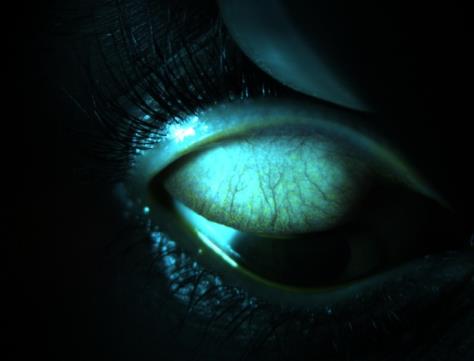
Signs: His right eye was perfectly fine. However in his left eye the signs observed were:
- Enlarged papillae (macropapillae)-apices stained with fluorescence in Zone 2
- Rough appearance of upper tarsal conjunctiva in Zone 2 & 3.
- Conjunctival hyperemia more at the superior region
- Mild swelling around upper lids
- Strands of mucus at inner canthus and underneath the upper palpebral conjunctiva underneath the lids
Examination of Contact Lens
While examining his contact lenses under high magnification with the slit lamp, his right lens was in good condition with no deposits and regular edge with no defects. His left lenses were also free of deposits but had a fine edge defect.
Management
CLPC, though is a reversible non-sight threatening condition, has capacity to limit the ability to tolerate contact lens wear in the longer term. Once CLPC it is seen in a CL user, CL wear must be ceased until the eye’s inflammatory condition has resolved. Depending upon the severity of the condition, management of CLPC can be initiated as non-pharmacological and/or pharmacological. In early cases, management is aimed on reducing ocular symptoms. In more severe cases management should be guided to prevent ocular tissue damage, caused by inflammation.
Non-Pharmacological
- Removal of lens deposits early.
- Replacement of soft lenses more frequently
- improve hygiene – more rigorous surfactant cleaning, more frequent enzyme use
- Polishing of RGP lenses and replacement in time
- Reduce exposure time
- abandon extended wear
- reduce daily wearing time to least possible
- Optimize lens fit, material and wearing regime
- rigid lens: alter overall diameter (repositions lens edge relative to tarsus), reduce edge clearance and edge thickness
- change soft lens material to one with improved deposit resistance
- change to daily disposable soft lenses
- Optimize lens care and maintenance
- Patient education and counseling
Pharmacological
- Topical mast cell stabilizers (gtt. sodium cromoglycate 2%, gtt. lodoxamide 0.1%, gtt. nedocromil sodium 2%):
- preserved drops should not be instilled with soft lenses in situ
- nedocromil sodium is yellow and may discolor soft lenses
- Topical combined anti-histamine/mast cell stabilizer e.g. gtt. olopatadine 0.1%
- In cases that do not respond to other treatment, consider a two-week trial of a ‘non-penetrating’ topical steroid such as gtt. fluoromethelone 0.1% (taper the dose)
- IOP monitoring is a must (at beginning and end of trial) In this case he was advised eye medications in the following manner along with lens removal from the left eye completely and cold compression.
- Gtt. Fluorometholone (0.1%) 1 drop four times daily in the left eye for 1 week
- Then, next week
- Gtt. Winolap Ds (Olopatadine 0.1%) 1 drop twice daily in the left eye for 2 weeks
- Gtt. Refresh Tears (CMC) 1 drop four times daily in the both eyes for 2 weeks
- He was then advised to follow up after 2 weeks
Follow up#1
On the first follow up he was symptomatically better. On examination under the slit lamp his left eye showed significant improvement with decrement in the papillae size and rough appearance of the palpebral conjunctival tissue in zone 2 & 3. He was then advised to use the medications in the following manner but still to cease off the lens wear in his left eye.
- Gtt. Acular LS (Ketorolac) 1 drop four times a day in left eye for 2 weeks
- Gtt. Winolap Ds (Olopatadine 0.2%) 1 drop four times a day in left eye for 2 weeks
- Gtt. Refresh Tears (CMC) 1 drop four times a day in both eyes for 2 weeks
He was asked to follow up after 2 weeks later Follow up #2
On examination at this time, the palpebral tissue had minimal reactions in the zones 2 & 3 in his left eye. His right eye was also fine. He was then refitted with monthly disposables silicone hydrogel contact lenses in his both eyes and was asked to continue Refresh Tears eye drops four times daily for a month more while stopping rest of the medications.
Discussion
Mr. XYZ used contact lenses for his cosmetic concern. He was eager to use contact lenses and hence was advised to wear them. He was counseled to use silicone hydrogels first, but the cost factor made him to stick with conventional hydrogel lenses. He was doing well with the pair. He followed all the instructions as per instructed.
He suffered CLPC due to the fine edge defect in his Contact lens. The lens might have torn due to improper lid closing of lens case or might be due to finger nail while cleaning. He was unaware of the fact and used the lens for some days. This caused trauma to tarsal conjunctiva which in turn released neutrophil chemotactic factor. This was the cause factor for his CLPC. He firstly took the discomfort as a normal adjustment like in first few days of lens wear but it never got easy and his symptoms increased day after day. Finally he visited us in the hospital and hence his current diagnosis was made.
Sharp edge defect induced trauma was the cause of the CLPC and it was managed as per non pharmacological and pharmacological measures. He was asked to discontinue the lenses and prescribed the medications. Later he was fitted with silicone hydrogel lenses and again was instructed on lens handling, hygiene and maintenance.

Contact lens induced papillary conjunctivitis (CLPC) is an inflammatory condition affecting the tarsal conjunctiva.
It is a complex, locally mediated, hypersensitivity and/or traumatic response seen in contact lens and ocular prostheses users, and those with exposed ends of nylon corneal sutures. People having this condition experience ocular irritation leading to contact lens intolerance. The eyes are often red and the palpebral conjunctiva shows cobblestone like elevations. Treatment for CLPC includes improvement of contact lens hygiene and replacement of lenses more frequently. Eye drops such as anti-histamines or mast cell stabilizers are often required to relieve symptoms and improve clinical signs. Steroid eye drops might be required in more severe cases. Early assessment, diagnosis and management are very essential.
References
-
Spring TF (1974) Reaction to hydrophilic lenses. Med J Aust 1(12): 449-450.
-
Allansmith MR, Korb DR, Greiner JV, Henriquez AS, Simon MA, et al. (1977) Giant papillary conjunctivitis in contact lens wearers. Am J Ophthalmol 83(5): 697- 708.
-
Korb DR, Allan smith MR, Greiner JV, Henriquez AS, Richmond PP, et al. (1980) Prevalence of conjunctival changes in wearers of hard contact lenses. Am J Ophthalmol 90(3): 336-341.
-
Allansmith MR, Ross RN (1989) Early stages of giant papillary conjunctivitis. Cont Lens J 17: 109-114.
-
Alemany A, Redal A (1991) Giant papillary conjunctivitis in soft and rigid lens wear. Contactologia 13: 14-17.
-
CarntNA, Evans VE, Naduvilath TJ, Willcox MD, Papas EB, et al. (2009) Contact lens-related adverse events and the silicone hydrogel lenses and daily wear care system used. Arch Ophthalmol 127(12): 1616-1623.
-
Holden BA, Sankaridurg PR, Jalbert I (2000) Adverse events and infections. In: Silicone Hydrogels: The Rebirth of Continuous Wear Contact Lenses, D Sweeney (Ed.), Butterworth Heinemann, Oxford, UK, pp: 150-213.
-
Cheryl S (2007) Contact lens induced papillary conjunctivitis (CLPC) with silicone hydrogel (SiH) contact lenses, at Vision CRC, The University of New South Wales.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report