Photo Essay
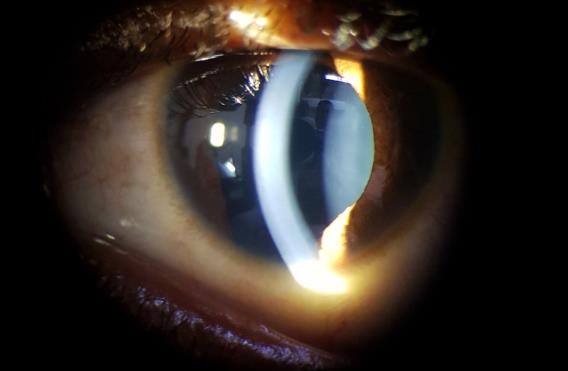
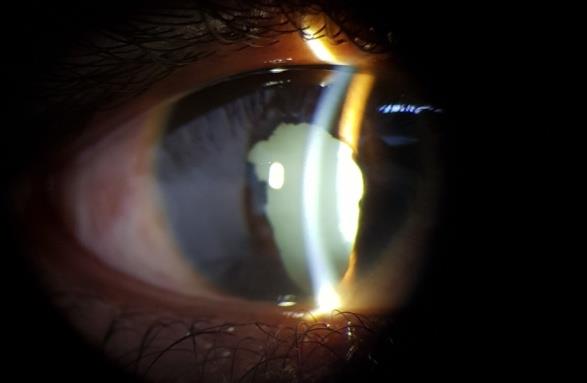
A case of tuberous sclerosis with B/L Iris coloboma, Right Eye Total cataract with Sensory exotropia. Left Eye Astrocytic hamartoma with Adenoma sebaceum and Shagreen patch as systemic associations.
Introduction
A 16-year-old boy presented to our OPD with complaint of decreased vision in right eye since early childhood. On examination, visual acuity in R/E was HMCF, PR accurate and in L/E was 20/200. Slit lamp examination showed iris coloboma with total cataractous lens in R/E (Figure 1 ) while L/E had iris coloboma only (Figure 2). Fundus was not visible in R/E but L/E fundus showed retinal astrocytic hamartoma superonasal to disc. There was R/E exotropia of 30⁰. Systemic examination revealed adenoma sebaceum over the face and shagreen patch over the back. These findings confirmed the diagnosis of tuberous sclerosis. Anterior segment findings like iris coloboma with cataract and non paralytic strabismus are not common presentations in patient with tuberous sclerosis in addition Astrocytic Hamartoma in this patient makes this case unique.


Discussion
Tuberous sclerosis complex (TSC) is a hamartomatous multisystem disorder involving nearly every organ of the body but primarily involving eye,skin and brain. TSC was initially described by Bourneville in 1880 and in 1908, the classic triad of epilepsy, mental retardation, and adenoma sebaceum was detailed by VOGT [1, 2]. Clinical manifestations show a vast diversity. Major and minor diagnostic criteria for TSC have been established by the Tuberous Sclerosis Consensus Conference in 1998 (Table 1). Diagnosis of tuberous sclerosis is categorized according to presence of major and minor criteria (Table 2) [3].
| Major Criteria | Minor Criteria | |||||
| Angiofibromas (3 or more) or forehead plaque | Dental enamel pits (more than 3) | |||||
| Hypomelanotic macules (3 or more) | Intraoral fibromas (2 or more) | |||||
| Ungual fibromas (2 or more) | Nonrenal hamartomas | |||||
| Shagreen patch or multiple collagenomas | Retinal achromic patch | |||||
| Multiple retinal hamartomas | “Confetti” skin lesions | |||||
| Cortical dysplasia’s (more than 3). This includes tubers and cerebral white matter radial migration lines. | Multiple renal cysts | |||||
| Subependymal nodule(s) | ||||||
| Subependymal giant cell astrocytoma(s) | ||||||
| Cardiac rhabdomyoma | ||||||
| Lymphangioleiomyomatosis (LAM) | ||||||
| Angiomyolipomas (2 or more) |
Table 1: Diagnostic Criteria of Tuberous Sclerosis.
| Definite TSC | 2 major criteria or 1 major plus 2 minor criteria |
| Probable TSC | 1 major and 1 minor criteria |
| Possible TSC | Either 1 major criteria or 2 or more minor criteria's |
Table 2: Major and Minor Criteria. Ophthalmic manifestations associated with TSC can be categorized into retinal and non-retinal.
Table 2: Major and Minor Criteria. Ophthalmic manifestations associated with TSC can be categorized into retinal and non-retinal. The retinal lesions of TSC were initially termed as ‘phakomas’ by Van der Hoeve in 1921 and concept of phakomatosis was introduced following this. These retinal lesions are now known as astrocytic hamartomas which is the most common retinal finding [4, 5]. Non-retinal findings include strabismus, poliosis of eyelashes, angiofibromas of the eyelids, coloboma of the iris, lens and choroid, papilloedema, and sector iris depigmentation [6, 7]. The prevalence of TSC associated retinal astrocytic hamartomas varies though largest reported series from the Mayo Clinic gives an overall prevalence of 49% [8, 9].
Prevalence of the non-retinal findings has been reported in a very few case series. Angiofibromas of the eyelids were the most common non-retinal finding (39%). Prevalence of non-paralytic strabismus and coloboma were only 5% and 3% [10]. Thus the presence of these very rare non-retinal findings like non- paralytic squint, B/L iris coloboma and cataract make our case exclusive.
References
-
Bourneville DM (1924) Sclerose tubereuse der circonvolutions cerebrales: idiotie et epilepsie hemiplegique. Arch Neurol (Paris) 1: 81-91.
-
Vogt H. Zur diagnostik der tuberosen sclerose. Z Erforsch Benhandl Jugendl Schwachsinns 2: 1-16.
-
Roach ES, Gomez MR, Northrup H (1998) Tuberous sclerosis complex consensus conference: revised clinical diagnostic criteria. J Child Neurol 13(12): 624- 628.
-
Van der Hoeve J. Augengeschwultse bei der tuberosen Hirnsklerose (Bourneville). Albrecht von Graefes Arch Klin Ophthalmol 105: 880-898.
-
Kinder RSL (1972) The ocular pathology of tuberous sclerosis. Journal of Pediatric Ophthalmology and Strabismus 9(2):106-107.
-
Nyboer JH, Robertson DM, Gomez MR (1976) Retinal Lesions in Tuberous Sclerosis. Arch Ophthalmol 94(8): 1277-1280.
-
Robertson DM (1991) Ophthalmic Manifestations of Tuberous Sclerosis. Ann NY Acad Sci 615: 17-25.
-
Lucchese NJ, Goldberg MF (1981) Iris and fundus pigmentary changes in tuberous sclerosis. J Paediatr Ophthalmol Strabismus 18(6): 45-46.
-
Gomez MR, Robertson DM. Ophthalmic findings. In: T uberous sclerosis complex. 3rd (Edn.), Oxford University Press, New York, pp: 145-159.
-
Rowley S, O'Callaghan F, Osborne J (2001) Ophthalmi c manifestations of tuberous sclerosis: a population based study. Br J Ophthalmol 85(4): 420-423.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report