Orbital Foreign Bodies: A Hospital Based Study of 44 Cases
Aim: To evaluate the pattern of injuries caused by orbital foreign bodies, types of orbital foreign bodies and also describe the management outline, including clinical presentation, radiological appearance, and treatment protocol. Material and Method: This observational case series study had been conducted in a tertiary eye hospital in Bangladesh from January 2013 to December 2020. Variables included demographic profile, clinical profile, and pattern of injuries, types of foreign bodies, medical and surgical treatment, and treatment outcome. Results: A total of forty-four (44) patients had been analyzed including male patients (75%) and female patients (25%) of orbital foreign body. Most of the patients (82%) were below the 40 years of age and young male patients. The mean age was 28.26 years and median age was 24 years. The patterns of injuries were Accidental trauma( 47.7%), physical assault (38.6%), iatrogenic (13.6%). The kinds of OFBs included metallic (34%), vegetative/wooden (43.2%), non-organic nonmetallic (22.7%). Orbitotomy (84%) had found as the main approach of the surgery in this study. The improvement of visual acuity after 6 weeks of treatment was highly significant (p value <0.001). Conclusion: Accidental trauma is the leading cause of OFB. Metallic foreign has reported as higher than others OFBs. The young age is preponderance for the injury. Early diagnosis, surgical exploration and extraction, when indicated greatly influence visual prognosis and final outcome.
Introduction
Orbital foreign body (OFB) causes a significant impact on ocular morbidity. It has a great concern in the paediatric and adolescent age group. An intraorbital foreign body can be defined as an object which is located inside the bony orbital wall, but outside the ocular globe [1, 2, 3, 4]. OFB can be classified according to its location and its consisting material. According to its location, it can be extra conal or intra conal [5]. It can be classified as metallic, organic or nonmetallic non-organic according to its material [6]. It is more prevalent in males, children, and young adults. Road traffic injuries, workplace injuries, household injuries, gunshot with high-velocity projection, political and social violence are important cause of intra orbital foreign body. The retained intraorbital foreign body may result in severe structural and functional damage to the eye or orbital content, including vision loss resulting from lesions to the eyeball, optic nerve, or their vasculature [7], from lesions of the sixth and third cranial nerves. It may mimic orbital inflammation, orbital cellulitis, orbital fistula, and orbital compartment syndrome [8]. All of these situations require urgent surgical intervention. However, surgical intervention is planned according to the type, nature, and location of the intraorbital foreign body, location of the foreign body, with or without presence of other injury or foreign body related complications. The approach to this kind of injury should be sequential, and multi-disciplinary with special attention to airways and hemodynamic stabilization followed by neurological, ophthalmological and vascular evaluation [9, 10, 11]. In this study, we attempt to evaluate the pattern of injuries, types of orbital foreign bodies and describe the management strategies, including clinical presentation, radiological appearance, weighing the risk, and treatment outcome.
Materials and Methods
An observational case series study had been carried out at Sheikh Fazilatunnessa Mujib eye hospital and training Institute, National Institute of ophthalmology and hospital, and Bangladesh eye hospital and institute in Bangladesh from January 2013 to December 2020. The study was following the tenets of the declaration of Helsinki. All patients were selected in this study, which gave a history of periocular or ocular trauma with suspected orbital foreign body and attended the Oculoplasty clinic at this time. The study’s primary aim was to manage orbital foreign body either by meticulously planned surgical procedures or by observation and follow-up. The pattern, location and size of the foreign body were the determining factors regarding management plan. Details of ophthalmic history including demographic profile (age, gender), nature of injury, visual status, time of presentation, location of foreign bodies by imaging studies were obtained, preoperative ocular examination, length of follow up period, treatment modalities, surgical procedure, subsequent management, related adverse reactions and or complications were recorded. The most helpful imaging technique is CT scan of the orbit. It also helps in the evaluation of PNS and the cranial cavity. A good axial and coronal imaging with sagittal reconstruction can point out the exact site of OFB. Metallic OFB tends to show significant hyper density with streaking artifact while nonmetallic OFB tends to appear of variable density without streaking. It also helps in identifying the orbital fractures. CT scan is the gold standard imaging technique to detect orbital FB as well as orbital rim and/or wall fracture. CT may give false results if OFB is wooden and also < 0.5 mm in size. Wooden FB is better seen with MRI that is often missed on CT as well as the evaluation of orbital soft tissue. However, MRI is contraindicated if FB is ferromagnetic. Thin axial and coronal CT images at variable window widths are beneficial to detect wooden FB in the orbit. All patients were treated by broad- spectrum antibiotic prior to surgery. Appropriate test of significance was done for the analysis of the study.
Management Strategy of OFB
After ruling out ophthalmic emergency and associated injuries in other parts of the body, the patient was evaluated by meticulous clinical examination and assessed by the CT scan of the orbit to evaluate the pattern, location and size of the OFB and associated orbital infection and inflammation. A broad-spectrum antibiotic had been advised for all patients before surgery and all suspected patients with infected foreign bodies. High dose intravenous steroid followed by oral corticosteroid with tapered doses were administered in the cases of traumatic optic neuropathy (TON). The management protocol is mentioned in a tabulated form (Table 1).
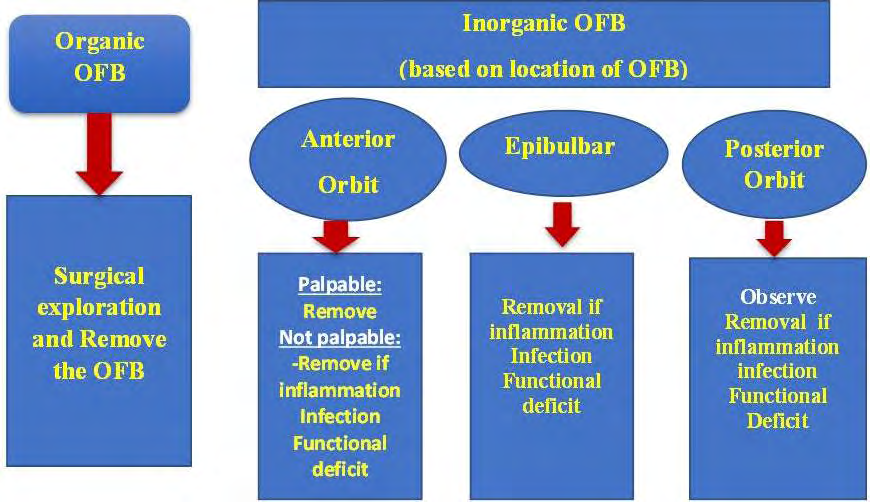
The decision on whether to remove the OFB is based on an assessment of the benefits and the possible risk. As a general rule, we tried to remove any orbital foreign body when we believe the procedure can be done safely and successfully based on the location of the OFB. We removed all anteriorly located OFB and an organic OFB even if it is posteriorly located because of potential risk of infection.
Results
A sum of 44 cases, including 33 males (75%) and 11 females (25%), were evaluated in this study. The range of age of the study was from one to 60 years. 15 (34%) patients were enrolled in 1 year to 20 years age group, 21 (47.7%) patients were in the age group of 21 to 40 years. 36 of 44
(81.8%) was below 40 years of age. Chi-square test had calculated and p-value (<0.05) was statistically significant. The mean was 28.26 years, and the median age was 24 years (Table 2). The types of injuries (Graph 1) had been noted as accidental trauma (47.7%), physical assault (38.6%), and iatrogenic (13.6%). Accidental trauma included road traffic accident, sports related injury, workplace injury, domestic injury and agriculture related injury. The Physical assault included political conflict and social conflict.
| Male | Female | P Value | |
|---|---|---|---|
| 1-20 years | 12 (80%) | 03(20%) | |
| 21-40 years | 17 (81%) | 04 (19%) | <0.005 |
| 41-60 years | 04 (50%) | 04 (50%) | |
| Total | 33 (75%) | 11 (25%) | |
| Mean Age | 28.26 ± 16.43years | ||
| Median Age | 24 years | ||
Table 1: Demographic profile of the study patients.
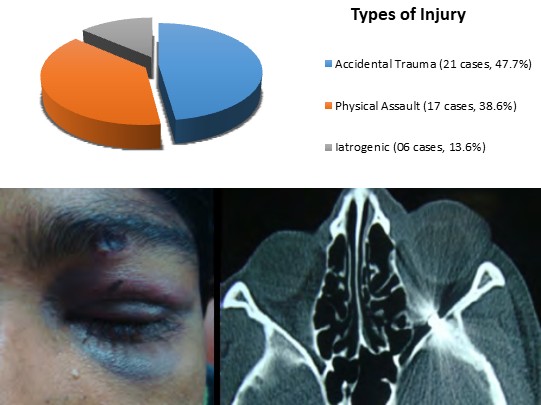
Graph 1: Distribution of types of Injury.
The types of OFB’s (Table 3) included metallic (34%), vegetative/wooden (43.2%), inorganic nonmetallic (22.7%). In metallic OFBs, 8 (53.3%) were pellet (Figure 1) and the rest 7 (46.7%) were other metallic OFBs. Posteriorly located pellet (6.8%) not causing the functional problem were left as they were. All metallic foreign bodies (Figure 2) except pellet were associated with a contaminated wound that required surgical extraction to remove the foreign body.
| No. | % | Pattern of OFB | |
|---|---|---|---|
| Metallic | 15 | 34% | Pellet: 8 (53.3%) |
| Metallic | 15 | 34% | Others: 7 (46.7%) |
| Vegetative | 19 | 43.20% | Bamboo stick: 9 (47.4%) |
| Vegetative | 19 | 43.20% | Wooden piece: 8 (42%) |
| Vegetative | 19 | 43.20% | Thorn: 2 (10.5%) |
| Non organic non metallic | 10 | 22.70% | Silicone material -02 (20%) |
| Non organic non metallic | 10 | 22.70% | Plastic 02 (20%) |
| Non organic non metallic | 10 | 22.70% | Glass particle 02 (20%) |
| Non organic non metallic | 10 | 22.70% | Gauze piece 02 (20%) |
| Non organic non metallic | 10 | 22.70% | others: 02 (20%) |
Table 2: Pattern of intra ocular foreign bodies.
Figure 1: A 22 years old male patient presented with loss of vision in his left eye for the last 7 days. He had also presented with ecchymosis on both eyelids of his left eye and a sealed wound point on the left upper eyelid. A hyperdense round metellic OFB with the artefect had marked in the most posterior part of left orbiton Axial image of the CT scan.

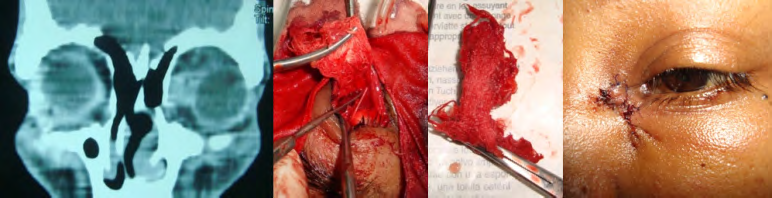
Orbitotomy (39 cases, 88.5%) was the main approach for removing the OFBs in this study. Multiple surgical approaches were needed in two (4.5%) cases of multiple pieces of the organic foreign body that were located in the posterior part of the orbit. In the cases of wooden foreign body and glass particles, the surgical field was meticulous searched to find out residual fragments in orbit. Surgical exploration was done in all cases of wooden OFBs (Figure 3) and all infected cases.

Figure 3: Standard clinical photo showing an 8×10 mm at the medial aspect of the upper eyelid. A hypo-intense mass with surrounding hyper-intense lesion in the right superior orbit on axial image of MRI of the orbit which was suggestive of wooden foreign body. Orbitotomy was made and a cylindrical shaped wooden foreign body was extracted from the orbit.
Among the inorganic non-metallic foreign bodies, Gauze piece was extracted from the orbit in two cases with history of DCR surgery (Figure 4) and Orbitotomy elsewhere. Exenteration was done in one case of severe infection of the orbit. We noticed three cases of intracranial extension of foreign bodies. Neurosurgical intervention in combination with orbital approach was required in four (9%) cases. At presentation, the visual acuity was 6/12 or better in 8 (18.2%) cases, 6/18 to 6/36 in 16 (36.37%) cases, 1/60 to 6/60 in 11 (25%), light perception to hand movement in 06 (13.64% and No light perception in 03 (6.82%) cases. Improvement of VA after 6 weeks was highly significant (p value<0.001) (Table 4). Visual outcome was poor in the cases of posteriorly located wooden orbital foreign body (15.9%), and associated with traumatic optic neuropathy (6.8%), and ruptured globe (9%).
| Visual Acuity | At Presentation | At 6 weeks | X2 Test |
|---|---|---|---|
| P Value | |||
| 6/6 to 6/12 | 8 | 13 | |
| 6/18 to 6/36 | 16 | 18 | 19.667 |
| 6/60 to 1/60 | 11 | 5 | < 0.001 |
| P.L to H.M | 6 | 2 | |
| NPL | 3 | 6 |
Table 3: Distribution of Visual status.
Discussion
Orbital foreign body is one of the important causes of ocular morbidity. It is more common in males and in younger population [4]. In this study, we noticed males (33 cases, 74.3%) were more affected than females (11 cases, 25.6%), similar to other studies. Most of the patients were 40 years and below in 36 (81.8%) compared to above 40 years (8, 18.2%) cases. The mean age was 28.26 years with median age 24 years. Younger males are more affected than females with a history of periocular injury with suspected retained orbital foreign bodies [12, 13].
The extent of structural and functional damage to the eye depends on the size of the foreign body, site of injury and pattern of the foreign body. In our study, we observed 15 (34%) metallic, 19 (43.2%) vegetative and 10 (22.7%) nonorganic nonmetallic foreign bodies that resembles with the study done by Fulcher TP, et al [3]. We found 20 (45.4%) foreign body impacted in the extra conal orbital space, 16 (36.4%) is involving the extra and intra conal space, and rest 8 (18.2%) in the intra conal space. In three cases, foreign body was extended in the intracranial space. Most of OFBs usually remain in extra conal space than intra-conal space [13]. The Extra ocular muscles may be injured during orbital injury. Extra ocular muscles were repaired in 9 (20.4%) cases at primary surgery or a later date. Our study showed that accidental trauma was the prominent cause of injury, 21 cases (41.7%) similar to other studies. A study showed their results correlated with our results. A Study reviewed that the majority of OFB case is associated gunshot injury (74%), physical assault remain the 2nd cause of injury that was 38.6% [14]. We observed 6 (13.6%) iatrogenic cases. These resulted from poor ophthalmic surgeries. Metallic introducer of DCR tube was impacted in the medial orbit in one case, impacted silicone tube was found in medial orbit in two cases, gauze piece was found in situ in two cases, and there was an impacted small surgical needle in one case. Meticulous ophthalmic surgery and follow up of the patient are important not only to prevent OFB but also for managing the patient.
The most common feature was chronic discharging sinus which was recorded in 18 cases (40.9%), mostly in the cases of organic OFBs. Followed by open wound (12 cases, 27.3%), non-healing infection (6 cases, 13.6%), ptosis (11 cases, 25%), impairment of vision (6 cases, 13.6%), proptosis (5 cases, 11.4 %), and periocular ecchymosis (5 cases, 11.4%).
The presence of a discharging sinus with a history of periocular injury should evoke suspicion of an organic foreign body in the orbit, regardless of the time between the presentation and trauma [15, 16]. It is imperative to maintain a high index of suspicion in such cases to avoid misdiagnosis. Orbitotomy was the main approach of surgery in this study for removal of OFB (39, 88.6%). Among Orbitotomy, the superior approach was more common (23 cases, 52.3%). Evisceration was done in 3 cases (6.8 %) due to post- traumatic phthisis bulbi, and exenteration was done in 01 (2.3%) with non-healing severe orbital abscess. Visual acuity improved in 36 (81.8%) patients as orbital inflammation subsided after removal of OFB. The VA is significantly improved in most of the patients in our study. Three cases had NPL VA at presentation. After 6 weeks, 6 (13.6%) cases ultimately lost their vision.
A study reported that final visual outcome correlated to location of foreign body. 85% (11 of 13) of patients with anterior IOFBs retained final visual outcome greater than 6/12, compared to only 30% (3 of 10) of patients with posterior OFBS. Additionally, 3 patients who developed NPL vision all had posterior OFBs. Management of each case depends on location of the OFB. Metallic foreign bodies not readily surgically accessible may be left in situ [13, 14].
Imaging is vital in proper localization of the foreign body, estimation of its consistency, size and evaluation of the response of surrounding orbital tissue; additionally it is useful in determining the integrity of the globe. The choice of imaging modality depends on the pattern of suspected foreign body. Plain X-ray is useful to localize radio-opaque objects. However plain x-ray is not sufficient in demonstrating the object details, their actual location in relation to surrounding structures and tissue response or damage. MRI is contraindicated if the OFB is ferromagnetic metallic due to chance of blindness and potential devastating consequence. Plain X-Ray is a useful technique to rule out any metallic foreign body prior to MRI. MRI is often used for detect of organic material; OFB missed on CT scan, or for evaluation of suspected optic nerve injury [13, 14, 17, 18]. A CT-Scan is the first choice of imaging technique to identify an OFB and associated tissue reaction. CT scan may produce false negative results particularly if the size of the foreign body is less than 0.5mm and especially in the case of wooden objects [19, 20]. A hyperdense OFB on CT imaging may not always be a metallic OFB because a long standing retained organic foreign body appearing as hyperdense [21]. A wooden foreign body tends to change its imaging characteristics with time based on the surrounding environment. We advised for CT scan of the orbit in 31 (70.4%) cases to assess the injury. MRI of the orbit was done in seven (15.9%) cases to assess organic vegetative foreign bodies after ruling out metallic OFB. Three (6.8%) cases have been evaluated by only plain radiograph as the patients could not afford other imaging modalities. OFB were extracted at the time of surgical exploration in 3 (6.8%) cases.
Though diagnosis of organic orbital foreign body is very difficult, but early diagnosis and treatment is very important to prevent severe complications, especially a bamboo stick that may contain large amount of bacteria and fungus and may provide good media for their growth, so organic foreign body like this can cause orbital infection, and panophthalmitis [22, 23, 24] or a chronic discharging sinus [16, 25, 26]. In cases of metallic foreign bodies, they may be left alone if they do not pose any ocular morbidity [27, 28]. It is very important to evaluate the globe and assessment of optic neuropathy for any penetrating injury of foreign bodies. Proper history taking, clinical examination, and imaging study are essential aids in diagnosing the OFB [29]. Timely intervention and skill of the surgeon may improve the prognosis and also reduce morbidity.
Conclusion
Removal of orbital foreign bodies is often challenging. Meticulous evaluation is a must. Detailed history, clinical examination and imaging give a clear picture. Early diagnosis, management and extraction of the foreign body if indicated, greatly influence the final outcome. Surgical removal is indicated for all types of organic IOFBs, anteriorly located metallic OFB, and OFB with the potential risk of infection and fatal outcome. Inorganic inert posteriorly located OFBs can be left alone, unless they are causing significant orbital complication. Every case should be individualized and multidisciplinary approach may be needed.
Conflict of Interest
The authors declare no potential conflicts of interest.
Author Contributions
SMK, SIS- designed the Study, procured the samples and performed the experiments, interpreted the results, SMK, MRM, SMRI- designed and performed the statistical analyses; SIS, RPM- provided critical input; SMK, SIS -wrote the first draft of the manuscript with information from all co-authors; SMK, SIS, RPM, GH- critical appraisal of the manuscript; All authors reviewed and approved the final version of the manuscript before submission.
Funding Support
The authors declared that this study received no financial support.
References
-
Czyz CN, Petrie TP, Harder JD, Cahill KV, Foster JA (2012) Intraorbital foreign body projectile as a consideration for unilateral pupillary defect. Int J Emerg Med 5(1): 14.
-
Jusue TI, Burks SS, Levine CG, Bhatia RG, Casiano R, et al. (2016) Wooden foreign body in the skull base: how did we miss it?. World Neurosurg 92: 580.
-
Fulcher TP, McNab AA, Sullivan TJ (2002) Clinical features and management of intra orbital foreign bodies. Ophthalmology 109(3): 494-500.
-
Al Mujaini A, Al Senawi R, Ganesh A, Al Zuhaibi S, Al Dhuhli H (2008) Intraorbital foreign body: clinical presentation, radiological appearance and management. Sultan Qaboos Uni Med J 8(1): 69-74.
-
Turliuc DM, Costan VV, Cucu AI, Costea CF (2015) Intraorbital foreign body. The Medical-Surgical Journal 119(1): 179-184.
-
Wang X, Xie Q, Chen H, Sheng X (2013) Orbital trauma with a large plant foreign body: a case report. Eye Science 28(1): 44-47.
-
Chung IY, Seo SW, Han YS, Kim E, Jung JM (2007) Penetrating retrobulbar orbital foreign body: A transcranial approach. Yonsei Medical Journal 48(2): 328-330.
-
Hada M, Chandra P, Gangwe A (2016) An unusual case of protruding retro-orbital metallic foreign body. Indian journal of ophthalmology 64(8): 604-606.
-
Cohen MA, Boyes Varley G (1986) Penetrating injuries to the maxillofacial region. Journal of Oral and Maxillofacial Surgery 44(3): 197-202.
-
Hudson DA (1992) Impacted knife injuries of the face. British Journal of Plastic Surgery 45(3): 222-224.
-
Ho V, Wilson MW, Fleming JC, Haik BG (2004) Retained intraorbital metallic foreign bodies. Ophthal Plast Reconstr Surg 20(3): 232-236.
-
Alves LP, Biselli LG, Sorbinho MVA, Aquino JLB, Pareira DL (2019) Removal of Foreign Body from Orbital Cavity without Visual Commitment in Patient Victim of Aggression: Case Report. EC Ophthalmology 10(10): 807-810.
-
Kadir SMU, Haider G (2017) Retained Intra orbital Foreign Bodies (IOFB). International Journal of Ocular Oncology and Oculoplasty 3(1): 14-18
-
Finkelstein M, Legmann A, Rubin PA (1997) Projectile metallic foreign bodies in the orbit: a retrospective study of epidemiologic factors, management, and outcomes. Ophthalmology 104(1): 96-103.
-
Bhuyan J, Ghuge A (2020) Intraorbital foreign body- a diagnostic challenge. Int J Health Sci Res 10(5): 92-95.
-
Kadir SM, Maurya RP (2020) A Report on intraorbital Foreigen body presenting as a chronic discharging sinus. Ind J Clin Exp Ophthalmol 6(4): 657-659.
-
Wilson WB, Dreisbach JN, Lattin DE, Stears JC (1988) Magnetic resonance imaging of nonmetallic orbital foreign bodies. Am J Ophthalmol 105: 612-617.
-
Shinder R, Gutman J, Gunasekera CD, Connor M, Nakra T (2011) Occult orbital organic foreign body. Ophthal Plast Reconstr Surg 27: 463-464.
-
Lakshmanan A, Bala S, Belfer KF (2008) Intraorbital organic foreign body-a diagnostic challenge. Orbit 27(2): 131-133.
-
Hansen MLU, Thorsbergera M, Jorgensenb JS, Buchwalda CV (2020) Penetrating Orbital Sphenoid Sinus Trauma with a Wooden Stick: A Challenging Case Report. Case Rep Ophthalmol 11: 540-545.
-
Nadella KS, Bansal O (2020) Retained intraorbital foreign body imaging! BMJ Case Reports CP 13.
-
Specht CS, Varga JH, Jalali MM, Edelstein JP (1992) Orbitocranial wooden foreign body diagnosed by magnetic resonance imaging. Dry wood can be isodense with air and orbital fat by computed tomography. Survey of Ophthalmology 36(5): 341-344.
-
Heyner FJ, Passmore JW (1965) Pseudotumor of Orbit*: Caused by Retained Foreign Body. American journal of ophthalmology 59(3): 490-492.
-
Yadav I, Maurya RP, Bhushan P, Singh MK, Singh VP, et al. (2015) Unrecognized large wooden intraorbital foreign body. Ind J Clin Exp Ophthalmol 1(1): 50-55.
-
Liu D, Al Shail E (2002) Retained orbital wooden foreign body: a surgical technique and rationale. Ophthalmology 109(2): 393-399.
-
Tuppurainen K, Mantyjärvi M, Puranen M (1997) Wooden foreign particles in the orbit‐spontaneous recovery. Acta Ophthalmologica Scandinavica 75(1): 109-111.
-
Mehta NS (2017) Metallic orbital foreign body: to dive or not to dive?. Sci J Med & Vis Res Foun 35(3): 27-29.
-
Zhou L, Li SY, Cui JP, Zhang ZY, Guan LN (2017) Analysis of missed diagnosis of orbital foreign bodies. Exp Ther Med 13(4): 1275-1278.
-
Barooah PS, Saikia N, Deuri A, Handique A, Deka D, et al. (2017) Management of Intra Orbital Foreign Body- A Hospital Based Study. International Journal of Contemporary Medical Research 4(7): 1624-1626.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report