Evaluation of Effectiveness of Bilamellar Tarsal Rotation Surgery in Trachomatous Trichiasis-A Study from Nepal
Background: WHO has recommended Bilamellar Tarsal Rotation (BLTR) surgery for Trachomatous Trichiasis. Though, several studies have addressed the success rate of this surgery, the reported success rate shows great variation. The aim of this study was to evaluate the effectiveness of Bilamellar Tarsal Rotation (BLTR) surgery in Trachomatous Trichiasis. Methods: This hospital based, prospective and interventional study was conducted at Geta Eye Hospital, Kailali, Far West Province of Nepal from February 15, 2005 to July 31, 2006 that included patients with Trachomatous Trichiasis undergoing BLTR surgery. Preoperative, operative and postoperative details were evaluated according to proforma. Patients were examined on 1st and 10th post-operative days and later between 6-9 months after surgery (1st follow-up) and between 14-17 months after surgery (2nd follow-up). Results: Altogether 67 patients were included in this study period. Out of total 99 lids with trichiasis, 85 lids underwent BLTR surgery. Among 85 lids that underwent BLTR surgery, 67 were of minor type and 18 were of major type of trichiasis. Recurrence of trichiasis was not found at 10th post operative day. At first follow-up, 5 (5.9%) lids had recurrence and at 2nd follow-up, 13 (15.3%) lids had recurrence of trichiasis. Among minor group of trichiasis 3 (4.5%) lids had recurrence at 1st follow-up and 10 (14.9%) lids had recurrence at 2nd follow-up. Similarly among major group of trichiasis, 2 (11.1%) lids had recurrence at 1st follow-up and 3 (16.7%) lids had recurrence at 2nd follow-up. Conclusion: BLTR surgery is simple, safe and successful. Recurrence of trachomatous trichiasis is common following BLTR surgery.
Introduction
Trachomatous trichiasis (TT) is the misdirection of eyelashes towards the globe which is called following scarring of palpebral conjunctiva in trachoma. Trachoma affects approximately 150 million individuals worldwide and is the leading cause of preventable blindness. Active trachoma is seen in communities with poor hygiene and inadequate sanitation [1, 2, 3, 4, 5, 6]. Acute infection is usually self- limited with few long-term sequelae. Repeated exposure to the agent leads to conjunctival cicatrization and corneal scarring [7]. Ocular strain of chlamydia trachomatis cause repeated episodes of conjunctivitis, with the peak prevalence of infection usually occurring in 3-5 years old [8]. Progressive scarring, entropion, and trichiasis lead to blinding corneal ulceration, typically some 40 years or later [9]. Among children, the prevalence and severity of the acute infection are equal between the sexes. Among adults, the prevalence of severe cicatrizing trachoma is 2-3 times higher for women [10].
Nepal was also one of the endemic regions for Trachoma. However, with continuous effort of eye care stake holders, trachoma is eradicated from Nepal. In Nepal overall prevalence of trachoma is 6.9% and is responsible for 2.4% blindness [11]. It was second leading cause of blindness. Highest prevalence of trachoma was found in mid-western and far-western region in Nepal. Fifty percent of trachoma cases are found within a 100 km radius of Nepalgunj and 90% of cases are found within a 200 km radius of Bheri and Seti zones. Certain ethnic groups are affected more, particularly Tharus, Ranatharus, Magars and Gurungs. Bilamellar Tarsal Rotation (BLTR) surgery has been found to be most effective by different comparative studies and is recommended by WHO as well.
A three-year follow-up of individuals who had undergone BLTR surgery found recurrent TT in 62% [12]. A Gambian study estimated that the median time to recurrence was 10 years after surgery [13]. El Toukhy, et al. [14] found that specific sutures or needles was associated with early failure of the BLTR procedure for Trachomatous trichiasis was unexpected. In a study conducted in Nepal, Zhang H, et al. [15] found that chlamydial infection at the time of surgery and at follow-up is a significant risk factor for postoperative TT recurrence.
The aim of this study was to evaluate the effectiveness of Bilamellar Tarsal Rotation (BLTR) surgery in Trachomatous Trichiasis. We also wanted to study, correction of trichiasis following BLTR surgery, evaluate the pre-operative and post- operative visual status, complications of BLTR surgery, age and sex distribution, ethnic predilection. Though, various studies have been done in Bilamellar Tarsal Rotation (BLTR) surgery in various parts of the world, no such study has been done Nepal. Though trachoma has been eliminated from Nepal, the outcomes of this study are relevant as it is still one of the major causes of blindness in some parts of the world.
Methods
This is a hospital based, prospective and interventional study. The study was conducted at Geta Eye Hospital (GEH), Kailali. All the cases of trachomatous trichiasis attending Geta Eye Hospital (GEH) undergoing BLTR surgery were included in the study. Cases excluded were Trichiasis/Entropion due to any cause other than trachoma, Trachomatous trichiasis with lagophthalmos, Cases of trachomatous trichiasis who are not suitable for operation such as hypertensive, diabetic, anemic, patients having bleeding disorder, Lids with trachomatous trichiasis with history of previous surgery for trachomatous trichiasis including electro epilation, cryotherapy, and Patients who didn’t come for follow-up examination. Cases of trachomatous trichiasis were screened from communities by trained eye health worker and brought to Geta Eye hospital. Those cases were rescreened in the hospital according to inclusion and exclusion criteria and selected for study. Informed consent was taken from the patients. Proforma was the tool for data collection which was designed to record the relevant history and clinical findings.
Detail history was taken from the patient and/or patients relatives. The proforma recorded demographic data, chief complaints, treatment history for trachoma if any history of epilation, past history of lid surgery if any (other than surgery for trachomatous trichiasis). Visual Acuity was assessed by illuminated Snellen vision box with multiple optotypes/E-chart. Examination of lid and adnexa was performed with daylight/bright and focused light. Trichiasis were assessed and graded as minor (less than 5 lashes) and major (5 or more than 5 lashes). Entropion and ptosis if present were recorded. Examination of lacrimal system (punctal position, occlusion, phimosis, regurgitation of mucus/pus on pressing sac) was done with the help of slit lamp in appropriate magnification and illumination. Anterior segment was examined under 5 step Haag Streit slit lamp. Posterior segment examination was performed with the help of Heine Beta 200 Direct Ophthalmoscope. Clinically diagnosed cases of trachomatous trichiasis were then posted for Bilamellar Tarsal Rotation (BLTR) surgery after consent. The latest grading of trachoma suggested by WHO (1987) is as follows was used to define trachomatous trichiasis. Trachomatous trichiasis is defined as at least one eyelash rubs on the eyeball or evidence of recent epilation of eyelashes. Indication for surgery were, one or more eyelashes which turn in and scratch the cornea when patient looks straight ahead, evidence of corneal damage from trichiasis, severe discomfort from trichiasis. BLTR surgery was considered contraindicative for cases with defective lid closure (lagophthalmos), poor general health, Hypertension, Diabetes, Asthma, heart failure, bleeding disorder, allergy to local anaesthesia.
Two trained ophthalmic assistants were the surgeons for the study. Both of them had at least 4yrs experience in BLTR surgery and each had already done more than 500 BLTR surgeries prior to doing surgery in this study. The operation was carried out in the minor operation theater in the hospital. Standard surgical sets were used in the operation. The operation was performed under local anesthesia. Injection Lignocaine (2%) was used for the anesthesia. Surgeons
performed the operation using 4X Carl Zeiss Loupe. Aseptic precaution was taken during surgery. Maximum 3ml of 2% lidocaine injected in the sub muscular plane above 3mm from lid margin and parallel to it.
In each case a skin incision 3mm above the lid margin in upper lid and below the lid margin in lower lid was given parallel to the lid margin from slightly lateral about 1mm. lateral to the lacrimal punctum to the lateral canthus. Upto muscle layer was incised. The lid was everted with the help of two hemostat forceps placed medially and laterally 5mm from the lid margin and again incision was given about 3mm from the lid margin through conjunctival surface. Palpebral conjunctiva and tarsal layer incised. Then through and through opening was made with the help of scissor. Rotating suture was placed at the central part and two ends of the incision. The suture was passed through the palpebral conjunctiva and partial thickness of the proximal tarsus and marginally through the orbicularis oculi muscle and skin to emerge about 1mm above the lash line. The suture was tied under moderate tension. The 4-0 single armed sutures were used in the operation. Padding of the operated eye was done after application of tetracycline eye ointment.
The patients were examined on 1st post-operative day and on 10th post-operative day. On the 10th post-operative day, sutures were removed. Detail ocular examination of the operated eye was done with torch light and under slit lamp on each follow-up and was recorded on the proforma. Besides the immediate postoperative examinations on 1st and 10th postoperative day, two major follow-up examinations were done, first at least 6 months following surgery (between 6 months to 9 months) and second at least 14 months following surgery (between 14 months and 17 months). Data were recorded according to proforma.
Any eyelash touching the globe following BLTR surgery in primary position of eye was considered as recurrence. Trichiasis was graded as minor if less than 5 eyelashes touch the eye globe and it was graded as major if 5 or more than 5 eyelashes touch the eye globe. Useful data were entered in computer database for statistical analysis. p-value was calculated by applying chi-square test, yates corrected test, fisher exact test wherever needed. The SPSS 14 version was used for this purpose.
Results
A total 67 patients, meeting the inclusion criteria, were included in this study. Total number of patients who had undergone Bilamellar Tarsal Rotation (BLTR) surgery in this study was 75. Of the 8 patients who were not seen, 5 patients were lost for follow-up on first follow-up examination and 3 patients were lost for follow-up on second follow-up examination. Of the 5 patients who were lost for first follow- up examination 3 had died and 2 could not be traced. The 3 patients who had been lost for second follow-up examinations also could not be traced.
Table 1 show that out of 67 patients, 19 (28.4%) were males and 48 (71.6%) were females. Patients were divided into different age group in the interval of 10 years. Table 1 show majority of the patients were of the age between 41 years to 70 years with peak at the age range of 51-60 years followed by 61-70 years and 41-50 years. Majority of the patients, 65 (97%) were Tharus and only 2 (3%) were from other ethnic group, one was Chettri and another was Biswokarma (Schedule cast).
| Age Group | Male | Female | Total | |
|---|---|---|---|---|
| <20 | 0 | 1 | 1 | |
| <20 | 0.00% | -2.10% | -1.50% | |
| 21-30 | 0 | 3 | 3 | |
| 21-30 | 0.00% | -6.30% | -4.50% | |
| 31-40 | 0 | 7 | 7 | |
| 31-40 | 0.00% | -14.60% | -10.40% | |
| 41-50 | 2 | 9 | 11 | |
| 41-50 | -10.50% | -18.70% | -16.50% | |
| 51-60 | 9 | 13 | 22 | |
| 51-60 | -47.40% | -27.10% | -32.80% | |
| 61-70 | 4 | 11 | 15 | |
| 61-70 | -21.10% | -22.90% | -22.40% | |
| 71-80 | 3 | 4 | 7 | |
| 71-80 | -15.80% | -8.30% | -10.40% | |
| >80 | 1 | 0 | 1 | |
| >80 | -5.20% | 0.00% | -1.50% | |
| Total | 19(28.4%) | 48(71.6%) | 67(100.0%) |
Table 1: Age and Sex Distribution of Patients.
Most common symptoms at presentation were foreign body sensation in the eye; all patients had foreign body sensation. Other symptoms at presentation were watering (64.2%), redness (31.3%) and diminution of vision (28.4%). Among the signs all patients had palpebral conjunctival scarring. Other common signs were Pannus (91%), superficial punctate keratitis (70.1%), Papillae (46.3%), Herbert’s pit (35.8%), Concretions (29.9%) and corneal ulceration (6.0%).
Table 2 shows that the total number of lids with trichiasis. A total of 268 lids of 67 patients were evaluated. Out of 268 lids, 28 right upper lids had trichiasis, of which 22 were of minor and 6 were of major category. Out of 15 right lower lids with trichiasis, 10 were of minor and 5 were of major category. Out of 42 left upper lids with trichiasis, 36 were of minor and 6 were of major category and out of 14 left lower lids with trichiasis, 10 were of minor and 4 were of major category. Total number of lids having trichiasis were 99, of which 78 (78.8%) were of minor category and 21 (21.2%) were of major category. Out of 268 lids of 67 patients, 9 lids had entropion (4 right lower lids, 3 left lower lids and 2 left upper lids). Out of total 134 eyes, 35 right eyes and 42 left eyes had corneal opacities. Of the 35 right eyes, 19 had nebular, 6 had macular and 10 had leucomatous opacities. Similarly of the 42 left eyes, 26 had nebular, 8 had macular and 8 had leucomatous opacities.
| Lid | Trichiasis | No. of Lids having Trichiasis | No. of Lids not having Trichiasis | No. of Lids having Entropion | No. of Lids not having Entropion | Total no. of Lids | |
|---|---|---|---|---|---|---|---|
| Minor | Major | ||||||
| RUL | 22 | 6 | 28 | 39 | 0 | 67 | 67 |
| RLL | 10 | 5 | 15 | 52 | 4 | 63 | 67 |
| LUL | 36 | 6 | 42 | 25 | 2 | 65 | 67 |
| LLL | 10 | 4 | 14 | 53 | 3 | 64 | 67 |
| Total | 78(78.8%) | 21(21.2%) | 99(36.9%) | 169(63.1%) | 9(3.4%) | 259(96.6%) | 268 |
Table 2: Lids with Trichiasis.
RUL: Right Upper Lid, RLL: Right Lower Lid, LUL: Left Upper Lid, LLL: Left Lower Lid Table 2: Lids with Trichiasis.
Table 3 shows out of 99 lids with trichiasis, 85 lids underwent Bilamellar Tarsal Rotation (BLTR) surgery. Out of 23 right upper lids that underwent BLTR surgery, 18 lids had minor trichiasis and 5 lids had major trichiasis. Out of 12 right lower lids that underwent BLTR surgery, 8 had minor and 4 had major trichiasis. Similarly, 38 left upper lids underwent BLTR surgery, of which 32 had minor and 6 had major trichiasis. Out of 12 left lower lids that underwent BLTR surgery, 9 had minor and 3 had major trichiasis. Altogether 85 lids underwent BLTR surgery, of which 67 had minor trichiasis and 18 had major trichiasis.
| Lid | Trichiasis | Total | |
|---|---|---|---|
| Minor | Major | ||
| RUL | 18 | 5 | 23 |
| RLL | 8 | 4 | 12 |
| LUL | 32 | 6 | 38 |
| LLL | 9 | 3 | 12 |
| Total | 67 | 18 | 85 |
Table 3: Lids completing BLTR Surgery.
10 patients had undergone cataract surgery following BLTR surgery in the same eye. So, this table includes total 68 eyes of 57 patients (excluding 10 patients who underwent cataract surgery in the same eyes concomitant with BLTR surgery). The visual acuity was grouped into four categories as above. Before operation 27 eyes had visual acuity in between 6/6-6/18 and 17, 7 and 17 eyes had visual acuity between <6/18-6/60, <6/60-3/60 and <3/60 respectively.
However, at 1st post-operative day, the number of eyes having visual acuity in between 6/6-6/18 was reduced to 24 eyes from 27 eyes. Similarly, 20, 7 and 17 eyes had visual acuity between <6/18-6/60, <6/60-3/60 and <3/60 respectively at 1st post-operative day. At 10th post-operative day 28, 19, 8 and 13 eyes had visual acuity between 6/6-6/18, <6/18- 6/60, <6/60-3/60 and <3/60 respectively. At 1st follow up 29, 21, 7 and 11 eyes had visual acuity between 6/6-6/18, <6/18-6/60, <6/60-3/60 and <3/60 respectively. Similarly at 2nd follow up 28, 19, 7 and 14 eyes had visual acuity between 6/6-6/18, <6/18-6/60, <6/60-3/60 and <3/60 respectively. Statistically, p value by chi-square test was not found to be significant on comparing the pre-operative with post-operative visual acuity.
Figure 1 show comparison of foreign body sensation and functional disability pre-operatively and post-operatively at first and tenth post-operative day and at first follow- up and second follow-up. All 67 patients had foreign body sensation before BLTR surgery. Following surgery 4, 1, 4 and 11 patients had foreign body sensation respectively at 1st post-operative day, 10th post-operative day, 1st follow-up and 2nd follow-up. Similarly 20 patients had functional disability pre-operatively and 1, 1, 2 and 1 had functional disability at 1st post-operative day, 10th post-operative day, 1st follow- up and 2nd follow-up respectively following BLTR surgery. Statistical analysis showed that p-value was significant for both foreign body sensation and functional disability on comparing foreign body sensation and functional disability pre-operatively and post-operatively at 1st post-operative day, 10th post-operative day, 1st follow-up and 2nd follow-up.
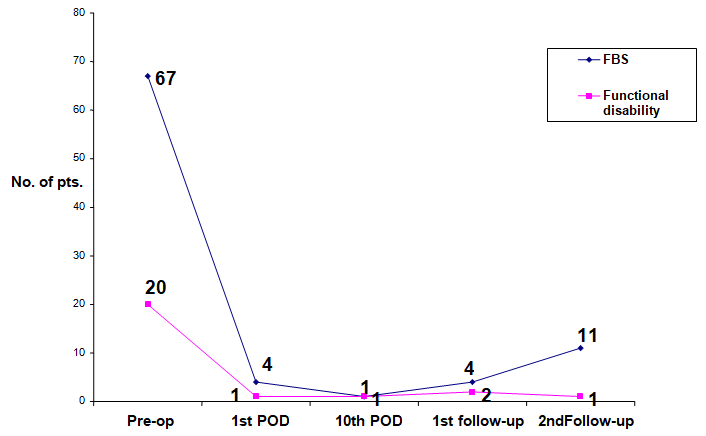
Figure 2 show that a total 85 lids were operated for trachomatous trichiasis. Outcome of operated 85 lids showed no recurrence at 10th post-operative day. However, at first follow-up, 5 (5.9%) lids and at 2nd follow up, 13 (15.3%) lids had recurrence of trichiasis.
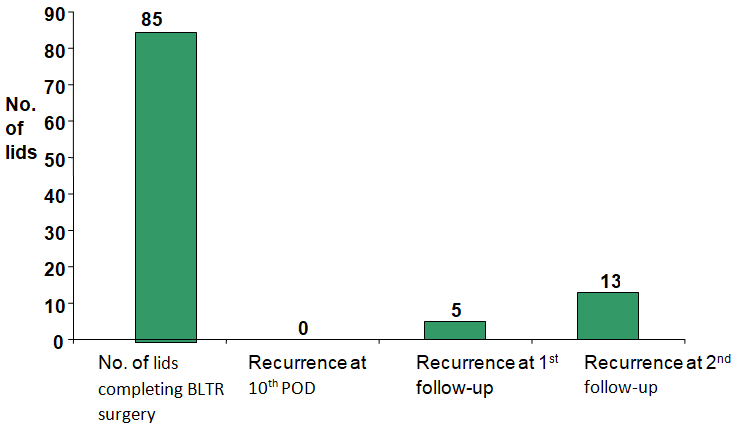
Table 4 shows that out of 85 operated lids for trichiasis, 67 lids had minor trichiasis and 18 lids had major trichiasis. Of 67 lids having minor trichiasis, there was no recurrence at 10th post-operative day, 3 (4.5%) lids had recurrence of trichiasis at 1st follow-up and 10 (14.9%) lids had recurrence of trichiasis at 2nd follow-up. Similarly, out of 18 lids having major trichiasis, there was no recurrence at 10th post- operative day, however, 2 (11.1%) lids had recurrence of trichiasis at 1st follow-up and 3 (16.7%) lids had recurrence of trichiasis at 2nd follow-up. Statistically, p-value was not found to be significant for recurrence among minor and major groups.
| Types of Trichiasis | No. of Lids with Trichiasis (Pre-Op) | Recurrence | ||
|---|---|---|---|---|
| 10th Post-Operative Day | 1st Follow-up | 2nd Follow-up | ||
| Minor | 67 | 0 | 3 | 10 |
| -4.50% | -14.90% | |||
| Major | 18 | 0 | 2 | 3 |
| -11.10% | -16.70% | |||
| Total | 85 | 0 | 5 | 13 |
| -5.90% | -15.30% | |||
| p value | 0.29 | 1 |
Table 4: Recurrence of Trichiasis in Minor and Major Group.
Table 5 shows that recurrence of trichiasis was seen between age group 41 years to 80 years. In the age group between 41-50 years there was recurrence in 2 lids at 1st follow-up and 5 lids had recurrence at 2nd follow-up. In the age group of 51-60 years, 2 lids had recurrence at 1st follow- up and 3 lids had recurrence at 2nd follow-up. In the age group of 61-70 years, 1 lid had recurrence at 1st follow-up and 3 lids had recurrence at 2nd follow-up. In the age group, 71-80 years, there was no recurrence at 1st follow-up and 2 lids had recurrence at 2nd follow-up. Statistically, p-value was not found to be significant for recurrence among the age groups. There were 2 lids had granuloma, one presented after 1 month of operation and another at 1st follow-up and 2 lids had lid notching.
| Age Group (Years) | No. of Lids Underwent BLTR Surgery | Recurrence of Trichiasis | ||
|---|---|---|---|---|
| 10th POD | 1st Follow-up | 2nd Follow-up | ||
| <20 | 1 | 0 | 0 (0.0%) | 0 (0.0%) |
| 21-30 | 3 | 0 | 0 (0.0%) | 0 (0.0%) |
| 31-40 | 9 | 0 | 0 (0.0%) | 0 (0.0%) |
| 41-50 | 14 | 0 | 2 (14.3%) | 5 (35.6%) |
| 51-60 | 28 | 0 | 2 (7.1%) | 3 (10.7 %) |
| 61-70 | 20 | 0 | 1 (5%) | 3 (15.0%) |
| 71-80 | 9 | 0 | 0 (0.0%) | 2 (22.2%) |
| >80 | 1 | 0 | 0 (0.0%) | 0 (0.0%) |
| Total | 85 | 0 | 5 (5.9%) | 13 (15.3%) |
| p value | p value | 0.85 | 0.35 |
Table 5: Recurrence of Trichiasis in Different Age Group.
Discussion
Our study also found female preponderance among patients with trachomatous trichiasis. Trachomatous trichiasis is a sequela of trachoma. Among 67 patients that were included in the study, 19 (28.4%) were males whereas 48 (71.6%) were females. This finding is supported by various other studies [11, 16, 17, 18, 19]. Children are considered as a reservoir for the Chlamydia trachomatis which causes trachoma and children are generally looked after by their mothers. So, the repeated infections transmitted to mother by their children may be the cause of higher number of females among the patients with trachomatous trichiasis.
Majority of the study subjects (55.2%) were in the age group of 51-70 years with peak age group of 51-60 years which comprised 32.8% of the study subjects. Trachomatous trichiasis is a sequela of trachoma and usually occurs in 4th to 5th decades of age. In our study, the age above 60 years comprised a smaller number of patients. Similar findings are reported in other studies [20]. Shannath ML, et al. [19] found majority of the patients (57.2%) were above 65 years of age which did not match to our study. Majority of the study population were the ethnic Tharus. The hospital where the study was carried out, itself was located in the tharu dominant society. This may be the cause of higher number of tharus in the study population. Nepal blindness survey (1981)11 also reported that the highest prevalence of trachomatous trichiasis is among the tharus.
In this study, more than one third, 99 lids (36.9%) lids had trichiasis. Other studies were done where Reacher MH, et al. [21] found 685 (41.36%) lids having trichiasis, Burton MJ, et al. [22] found 124 (52%) eyes had major trichiasis, 75 (31%) eyes had minor trichiasis and 42 (17%) eyes had no trichiasis. This study did not match to our study as our study had more number of lids with minor trichiasis [20]. similar to our study, reported majority lids 45.3% had minor trichiasis and 27.7% lids had major trichiasis. The corneal opacity is the main cause for visual impairment and blindness in trachoma Burton MJ, et al. [17] found corneal opacities in 47.9% of eyes in their study which was less than that found in this study, 77 eyes (57.5%).
There was slight improvement of visual acuity following BLTR surgery starting with 10th post-operative day which could be due to removal of the irritating ailments like foreign body sensation following surgery. There are studies which report improvement of visual aucity after surgery, Reacher MH, et al. [21] reported beneficial effect on visual acuity following surgery in general and studies which report no improvement of visual acuity after surgery Burton MJ, et al. [18] showed general deterioration in visual acuity between surgery and follow-up. Another study by Burton MJ, et al. [17] showed improvement of visual acuity by 12 months following operation.
This shows that both foreign body sensation and functional disability markedly got reduced following BLTR surgery. Functional disability was defined as those whose normal activities of life were hampered due to trichiasis. The foreign body sensation was gradually experienced again during subsequent follow-ups which could be due to the recurrence of trichiasis at follow-up. Khandekar R, et al. [16] reported patients without recurrence to have better quality of life and satisfaction compared with those patients with recurrence.
Out of 99 lids with trichiasis, only 85 lids underwent BLTR surgery. 9 lids had trichiasis which was already operated for trachomatous trichiasis and those lids were excluded and 5 lids with trichiasis could not be operated as those patients did not allow performing surgery in more than one lid. Out of the operated 85 lids, trichiasis recurrence was looked for at 10th post-operative day, 1st follow-up and 2nd follow-up. Recurrence was entertained even if a single eyelash touched the eye globe in primary position of the eye. There was no trichiasis recurrence at 10th post-operative day. At first follow-up 5.9% (n=5) lids had trichiasis recurrence while at second follow-up 15.3% (n=13) lids had trichiasis recurrence. Recurrence rate was statistically significant at each follow-up in comparison to baseline. Zhang H, et al [15] reported 11.1% trichiasis recurrence at 6 months and 25% recurrence at 12 months following BLTR surgery. Trichiasis recurrence rate in this study is higher than that of our study el Toukhy, et al. [14] evaluated the short-term outcome of BLTR surgery and found 16.4% trichiasis recurrence after 8 weeks. This study has high recurrence rate of trichiasis following BLTR surgery than our study even at short duration. Shannath ML, et al. [19] found 28% recurrence rate of trichiasis following BLTR surgery where the follow-up was done for minimum period of 18 months after surgery. This study again found the recurrence rate higher than our study Alemayehu W, et al. [23] reported 5.4% recurrence at 3 months and 14.3% recurrence at 6 months which has higher trichiasis recurrence rate than our study Khandekar R, et al. [12] in a study found 61.8% recurrence rate of trichiasis following BLTR surgery after an average of 3.1 years. The trichiasis recurrence rate in this study is higher in comparison to our study but the recurrence was evaluated at longer duration. Another study by Khandekar R, et al. [16] reported 47.2% trichiasis recurrence after 17 years of BLTR surgery. Trichiasis recurrence rates reported by more formal prospective clinical studies have reported lower at around 20% after 2 years [21, 24] which is comparable to our study. Our study also showed increased recurrence rate with increasing time period which is comparable to the study done by Zhang H, et al. [20] and Alemayehu W, et al. [23]. There is no consistency in the recurrence rate of trichiasis following BLTR surgery as shown by various studies done at various places. Compared with most of the studies, our study has documented less trichiasis recurrence rate.
Analysis of our study found out that the recurrence rate of trichiasis following BLTR surgery in the lids with minor and major trichiasis varies. In our study 67 lids had minor trichiasis and 18 lids had major trichiasis. But statistically it was not significant while comparing the trichiasis recurrence among minor and major group. Reacher MH, et al. [21] reported 20% recurrence among the lids with minor trichiasis and 23% recurrence among the lids with major trichiasis at about 2 years after surgery. This is comparable with our study. Adamu Y, et al. [25] found the 13.8% recurrence following BLTR surgery among the lids which had minor trichiasis and 14% in lids which had major trichiasis. There was no significant difference in the recurrence rate among minor and major group which is statistically comparable to our study. Thus, minor and major type of trichiasis at the baseline before surgery does not seems to affect the recurrence rate of trichiasis. It was found that Posterior Lamellar Tarsal Rotation (PLTR) was found to have superior long-term outcomes in comparison to Bi-lamellar Tarsal Rotation (BLTR) with lower risk of post-operative trachomatous trichiasis (PTT) [26].
In this study, recurrence of trichiasis was seen from 41 years to 80 years. Statistically the recurrence of trichiasis among different age group is not significant. Alemayehu W, et al. [23] found no difference in the recurrence by age. This is comparable to our study. Conjunctival sutural granuloma and central lid notching are the commonly encountered complications which can be avoided by doing operation carefully. In our study, two lids following BLTR surgery developed granuloma, one had conjunctival granuloma presenting at 1 month after operation and the granuloma was excised under local anaesthesia. Besides this, 2 upper lids had lid notching at the central part. Bog H, et al. [24] reported wound infection in 1 eye lid among 144 eyes and 9 (6.25%) eyes developed central lid notching. We did not have even a single case of postoperative wound infection. Reacher MH, et al. [21] reported overcorrection in 1.3% of lids which persisted despite removal of rotating sutures 7 days after surgery and conjunctival sutural granuloma found in 12.6% lids.
Conclusion
Trachomatous trichiasis, a sequela of trachoma, is more prevalent in females than males. Trachomatous trichiasis is commonly seen in older age group. Ocular discomfort is significantly decreased following surgical intervention. BLTR surgery is uniformly successful for both minor and major trichiasis and recurrence of trichiasis following BLTR surgery is not associated with age. Recurrence of trachomatous trichiasis is common following BLTR surgery. Recurrence of trichiasis following BLTR surgery increases with increasing time interval following surgery. Granuloma and lid notching are common complications following BLTR surgery. Although following BLTR surgery, patients feel quite comfortable, yet no significant visual improvement occurs but it prevents the deterioration of vision.
References
-
Dawson CR, Daghfous T, Messadi M, Hoshiwara I, Schachter J (1976) Severe endemic trachoma in Tunisia. Br J Ophthalmol 60(4): 245-252.
-
Dawson CR, Jones BR, Tarizzo ML (1981) Guide to trachoma control. World Health Organization. Geneva, pp: 12-20.
-
Dawson CR, Schachter J (1967) Trachoma in Jamaica Epidemiologic and Microbiologic Observations on Mild Disease. Am J Ophthalmol 63(5): 1408-1413.
-
Duke Elder S (1965) System of ophthalmology. St Louis: Mosby 8: 258-295.
-
Fox LW (1929) The Indians and the trachoma problem. Am J Ophthalmol 12(6): 457-468.
-
Dawson CR, Daghfous T, Messadi M, Hoshiwara I, Schachter J (1976) Severe endemic trachoma in Tunisia. Br J Ophthalmol 60(4): 245-252.
-
Grayston JT, Wang S (1975) New Knowledge of Chlamydiae and the diseases they cause. J Infect Dis 132(1): 87-105.
-
Bird M, Dawson CR, Schacter JS, Miao Y, Shama A, et al. (2003) Does the diagnosis of trachoma adequately identify ocular chlamydial infection in trachoma- endemic areas? J Infect Dis 187(10): 1669-1673.
-
Mabey DC, Solomon AW, Foster A (2003) Trachoma. Lancet 362(9379): 223-229.
-
Tabbara KF (1996) Chlamydia: Trachoma and Inclusion Conjunctivitis. In: Tabbara KF, et al. (Eds.), Infections of the Eye. 2nd (Edn.), USA: Little, Brown and Company, pp: 433-499.
-
Brilliant GE, Pokhrel RP, Grasset NC, Brilliant LB (1988) The Epidemiology of Blindness in Nepal: Report of the 1981 Nepal Blindness Survey. The Seva Foundation Chelsea 7: 243-311.
-
Khandekar R, Mohammed AJ, Courtright P (2001) Recurence of trichiasis: a long term follow-up study in the Sultanate of Oman. Ophthalmic Epidemiol 8(2): 155- 161.
-
Bowman RJ, Jatta B, Faal H, Bailey RL, Foster A, et al. (2000) Long term follow-up of lid surgery for trichiasis in the Gambia: surgical success and patient perceptions. Eye 14(6): 864-868.
-
el Toukhy E, Lewallen S, Courtright P (2006) Routine Bilamellar Tarsal Rotation Surgery for Trachomatous Trichiasis: short-term outcome and factors associated with surgical failure. Ophthalmic Plastic Reconstr Surg 22(2): 109-112.
-
Zhang H, Kandel RP, Sharma B, Dean D (2004) Risk Factors for recurrence of postoperative trichiasis: Implication for trachoma blindness prevention. Arch Ophthalmol 122(4): 511-516.
-
Khandekar R, Al Hadrami K, Sarvanan N, Al Harby S, Mohammed AJ (2006) Recurrence of trachomatous trichiasis 17 years after bilamellar tarsal rotation procedure. Am J Ophthalmol 141(6): 1087-1091.
-
Burton MJ, Kinteh F, Jallow O, Sillah A, Bah M, et al.(2005) A randomized controlled trial of azithromycin following surgery for trachomatous trichiasis in the Gambia. Br J Ophthalmol 89(10): 1282-1288.
-
Burton MJ, Bowman RJC, Faal H, Aryee EAN, Ikumapayi UN, et al. (2005) Long term outcome of trichiasis surgery in Gambia. Br J Ophthalmol 89(5): 575-579.
-
Shannath LM, Sheila KW, Emily SW (2004) Pattern of recurrence of trachomatous trichiasis after surgery. Presented at: Association for research in vision and ophthalmology annual meeting. Fort Lauderdale, Florida.
-
Zhang H, Kandel RP, Atakari HK, Dean D (2006) Impact of oral azithromycin on recurrence of trachomatous trichiasis in Nepal over 1 year. Br J Ophthalmol 90(8): 943-948.
-
Reacher MH, Munoz B, Alghassany A, Daar AS, Elbualy M, et al. (1992) A controlled trial of surgery for trachomatous trichiasis of the upper lid. Arch Ophthalmol 110(5): 667- 674.
-
Burton MJ, Bowman RJ, Faal H, Aryee EA, Ikumapayi UN, et al. (2006) The long-term natural history of trachomatous trichiasis in the Gambia. Invest Ophthalmol Vis Sci 47(3): 847-852.
-
Alemayehu W, Melese M, Bejiga A, Worku A, Kebeda W, et al. (2004) Surgery for trichiasis by ophthalmologists versus integrated eye care workers: a randomized trial. Ophthalmology 111(3): 578-584.
-
Bog H, Yorston D, Foster A (1993) Results of Community- based eyelid surgery for trichiasis due to trachoma. Br J Ophthalmol 77(2): 81-83.
-
Adamu Y, Alemayehu W (2002) A randomized clinical trial of the success rates of bilamellar tarsal rotation and tarsotomy for upper lid trachomatous trichiasis. Ethiop Med J 40(2): 107-114.
-
Habtamu E, Wondie T, Tadesse Z, Atinafu B, Gashaw B, et al. (2019) Posterior lamellar versus bilamellar tarsal rotation surgery for trachomatous trichiasis: Long-term outcomes from a randomised controlled trial. E Clinical Medicine 17: 100202.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report