Visual Acuity after AcrySoft®IQ PanOptix®/PanOptix® TORIC Lens Implantation in Relation to Preoperative Pupil Size Values, Angles Alpha and Kappa Examined using the iTrace Analyzer
Visual acuity of 35 patients (49 eyes) implanted with AcrySoft®IQ PanOptix® spherical or toric lenses by Alcon was analyzed considering preoperative pupil size, angles alpha and kappa, the values of which were obtained in the examination using iTrace analyzer. Overall, no statistically significant changes in visual acuity were observed for changing values of the above parameters, except in the preoperative group with hyperopia, in which visual acuity to far distances improved with increasing pupil size. In some patients after refractive lens exchange, a slight deterioration in visual acuity to far distances was observed compared to preoperative values obtained with best correction; however, this did not have a significant impact on the level of patient satisfaction.
Introduction
AcrySoft®IQPanOptix® (PanOptix), AcrySoft®IQ PanOptix®TORIC (PanOpix toric) lenses are among the latest arrivals by Alcon used in the correction of postoperative aphakia. As one of only few models in the world, this product has undergone FDA registration for eye correction after refractive lens exchange (RLE). Lenses with a concentric, trifocal structure, allowing for good visual acuity to far distances, intermediate distances and near distances, are the unquestionable bestseller for Alcon Company. Since their introduction on the market, the number of implantations has exceeded 500,000 pcs. The company’s success is even greater as it concerns a premium class lenses. What is behind such an achievement? The recognition of Alcon, its global reach, a huge number of doctors who trust and therefore use the company’s products, including “doctors-advocates”, certainly helps promote the product. However, if the product does not have appropriate quality, its promotion may have a limited effect. So, what is behind the success of the PanOptix lens? Proven material and shape certainly facilitate the process of doctors getting used to the new product. However, this is still not enough. A specific structure that allows for the intended effects in terms of visual acuity and quality of vision to be achieved repeatedly is the key to success. A diffraction structure, addition to near distances at the level of + 3.25Dsph, good quality of vision to far, near and intermediate distances (at a distance of 60-70 cm) are the most important features of this lenses. The light energy transmission to the retina at the level of 88% with the use of ENLIGHTEN™ technology allows us to obtain the appropriate image quality through more efficient use of light energy. The risk of developing postoperative visual impairments is only 4.8%. Patients said, they were bothered very much by starbursts (n=125), 2.4% by halos and 1.6% by glare [1, 2].
Lens surgery is performed in ever younger patients who are not diagnosed with cataract, but only with refractive errors. They are middle-aged people, often 40-year-olds, with very good visual acuity to far and near distances, requiring the use of eyeglasses or contact lenses. Patients who decide to have RLE, first of all want to get rid of the unwanted correction. Their expectations involve quality of vision and visual acuity at least comparable to that, which can be obtained using non-surgical methods of correcting the eye defect. How to assess which lens model is best for a given patient? An individual approach to each patient is a clue for best correction.
Qualification for the implantation of premium class lenses should normally include the patient’s medical history, specification of the patient’s expectations after the procedure and examination of all eye structures. Particular attention should be paid to the condition of the cornea, including its anterior surface, pupil function and condition of the retina. An examination of visual acuity (VA) to far and near distances is another inseparable element of the qualification that may result in disqualification from a premium class lens implantation. Preoperative assessment of the pupil size, its normal function and determination of ocular dominance are other constant elements of the qualification process. In the case of EDOF lenses, pupil size is one of the most important qualifying factors [3].
Are the above tests sufficient to choose the best product for the patient? A lot of uncertainties regarding the correct qualification arise when a doctor or center specializes in the implantation of premium class intraocular lenses, and the monofocal lens is the product recommended last.
The complex structure of the lens itself poses a risk of adverse effects in terms of postoperative visual quality [4]. In the case of a complex structure of the eye, including, for example the presence of higher-order aberrations (HOA) generated by the cornea, a paracentrally located pupil, which is determined by the size of angle kappa, or the presence of excessively large angle alpha, the lack of information on this topic can completely eliminate or lower the expected beneficial postoperative effect.
Objective
Retrospective comparative analysis of pre- and postoperative values of visual acuity to far and near distances in patients who underwent lens removal surgery due to lens opacification or existing refractive errors, and subsequent PanOptix or PanOptix toric lens implantation. The obtained results were analyzed taking into account preoperative angles kappa and alpha, pupil size, and the type of preoperative refractive error.
Materials and Methods
35 people, 49 eyes were subjected to lens removal and subsequent implantation of an artificial PanOptix/PanOptix toric lens.
The procedure was carried out in thirty eyes due to diagnosed cataract. This group included two patients (2 eyes) in whom a monofocal lens was replaced with PanOptix lens (1 eye) and PanOptix toric lens (1 eye). The procedure was carried out 5 years after the implantation of a monofocal lens also made by Alcon (33-year-old patient, eye after a trauma). Below is a short video presenting the procedure: https://www.youtube.com/watch?v=OWznWiXn_uo&t=5s The second group consisted of 17 patients qualified for RLE-19 eyes. In this group 7 patients were waiting for the implantation of the same model of the lens into the second eye. The next three people are monocular patients. The remaining seven patients got lenses from another companies: a premium lens was implanted in 4 eyes, a monofocal lens in 3 eyes.
All procedures were performed by one surgeon at a private medical center-Silesian Eye Treatment Center in Zory, Poland. Statistical information related to the performed procedures is included in the (Table 1).
| Total number of patients (eyes) | 35 (49) |
|---|---|
| Age (years) | 56 ±23 |
| male | 17 |
| female | 16 |
| cataract | 22 (30) |
| RWS | 13 (19) |
| Monocular implant | 17 |
| Binocular implant | 16 |
| PanOptix spherical | 41 |
| PanOptix toric | 8 |
| Preoperative hyperopia | 14 |
| Preoperative myopia | 27 |
Table 1: Contains information on the age and gender of patients, the reason for lens removal, the number of spherical and toric i
Qualification for Implantation of the Panoptix/Panoptix Toric Lens
Optometric Examination
They included assessment of visual acuity to far and near distances without correction and with best correction, assessment of ocular dominance, color differentiation tests and examination assessing the state of stereoscopic vision.
Ophthalmological Examination
The pupil size was assessed under photopic conditions, its reaction to light, the condition of the iris structure, lens, vitreous body, and retina. In eyes with existing macular degenerative changes, but with normal visual acuity values, optical coherence tomography (OCT) was performed in each case.
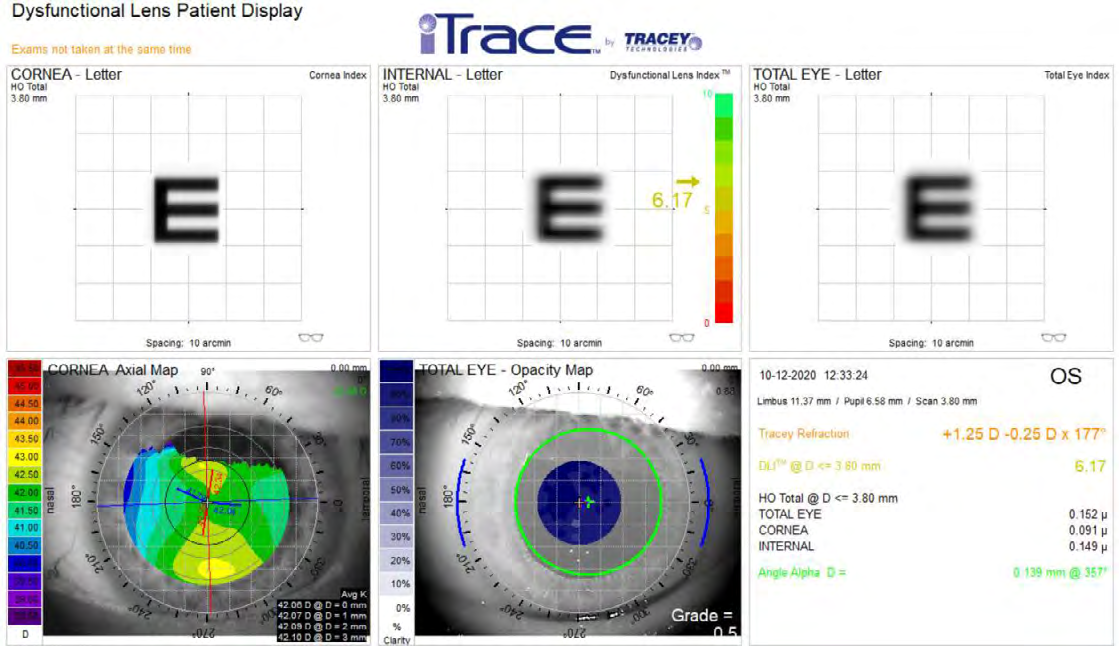
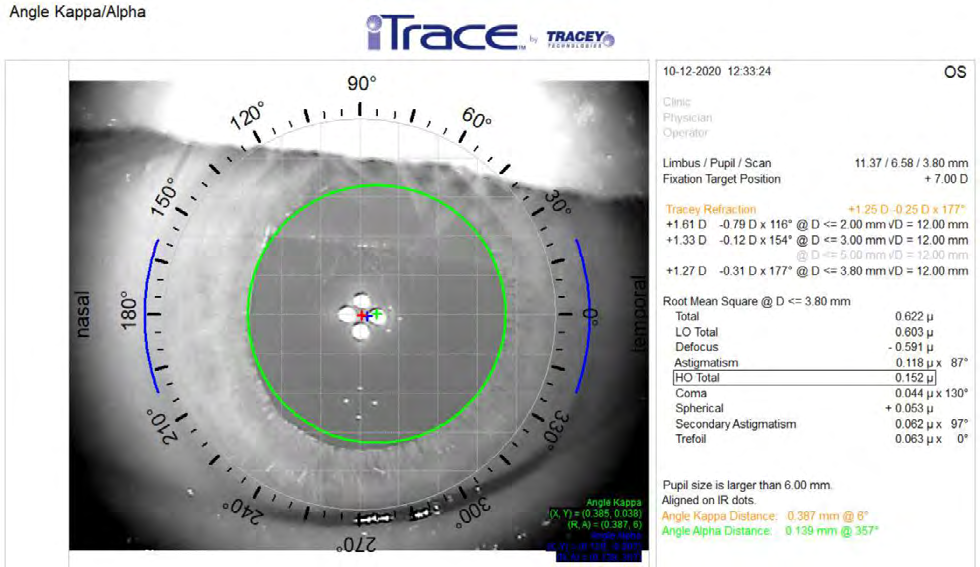
The standard of preoperative examinations performed at the Silesian Eye Treatment Center in the qualification process for the implantation of premium class lenses is examination using the iTrace analyzer. Using the Dysfunctional Lens Patient Display module (Figure 1), among others, condition of the cornea in terms of the presence of HOA was assessed. The Angle Kappa/Alpha module was used for the assessment of the size of angle kappa, its position relative to the visual axis and the size of angle alpha (Figure 2).
Exclusion Criteria
The presence of corneal HOA, pupil size greater than 6.0 mm as assessed under photopic conditions, lens subluxation, vitreous thickening impeding fundus view are main contraindication factors. Subsequently, the presence of macular degeneration causing visual impairment and eye amblyopia were other reasons for the patient’s disqualification from the procedure.
It is worth mentioning that the presence of mild retinal degenerative changes, conditions after posterior vitrectomy (retinal detachment, macular hole, and epiretinal membrane) were not a contraindication to this model of lens implantation, if the predicted postoperative visual acuity to far and near distances was good.
The main factor disqualifying patients from RLE procedure is saved lens accommodation. According to the authors of this study, a properly functioning accommodation is currently irreplaceable by intraocular artificial lenses.
An examination using the iTrace analyzer were performed in each eye 3 times, with an interval of 1-3 minutes, in the preoperative period. The iTrace is a powerful device to analyze visual function and sources of aberrations. This is the only device that uses ray tracing for wavefront analysis. Using this analyzer one of authors in the article “Usefulness of Itrace in Diagnosing Unclear Cases of the Deterioration in Visual Acuity. Congenital Lens Dysfunction as a New Disease Entity. Preliminary Reports” discover a correlation between the presence of dysfunctional (although looking healthy) lens and poor visual acuity to far distance with saved, normal visual acuity to the near distances [5].
Technique
Each lens was introduced into the capsule following phacoemulsification (cataract) or phacoaspiration (RLE). The axis of corneal astigmatism was determined in two stages, in a sitting position marking the cornea, then with the use of a Tocular® axial scale lens mounted in a Muller- Wedel microscope. When performing statistical analysis, the correlation coefficient was used, and then a correlation significance test was performed at the significance level of 0.05. Each of the patients was asked about the quality of postoperative vision and satisfaction with the procedure performed.
Results
The procedures were performed in the period from January 2020 to March 2021. The average follow-up was 5 months. Patients with myopia constituted the majority of the group. Eye defects ranging from -0.75Dsph to -19.5Dsph were corrected. The next group was patients with hyperopia, within the scope of the corrected error from + 0.5Dsph to +2.5Dsph. The remaining group consisted of patients without eye defect and patients with diagnosed astigmatism, which most often accompanied myopia.
Visual Acuity
Visual acuity to far distances was performed using LogMAR charts, and to near distances using Snellen charts. Vision to intermediate distances was assessed by asking patients to read the text from a computer with a standard font, from a distance of 60-80 cm.
The analysis of visual acuity included the comparison of the preoperative values, with best correction, with the postoperative values, tested without correction, 3 months after the procedure. Such a postoperative period was chosen due to the anatomical changes occurring in the lens capsule. Immediately after the procedure, in most cases, the presence of capsular folds was observed which could affect quality of vision and visual acuity. The folds receded almost completely by two months after the procedure. The patients were divided into two groups depending on the reason for the procedure. Patients with visual acuity to far distances of ≤ 0.2 LogMAR were included in the group diagnosed with cataract.
The group of patients undergoing RLE included patients with visual acuity to far distances of ≥ 0.1 LogMAR.
The obtained values of visual acuity to far distances in both groups were presented in a (Graph 1a & 1b).
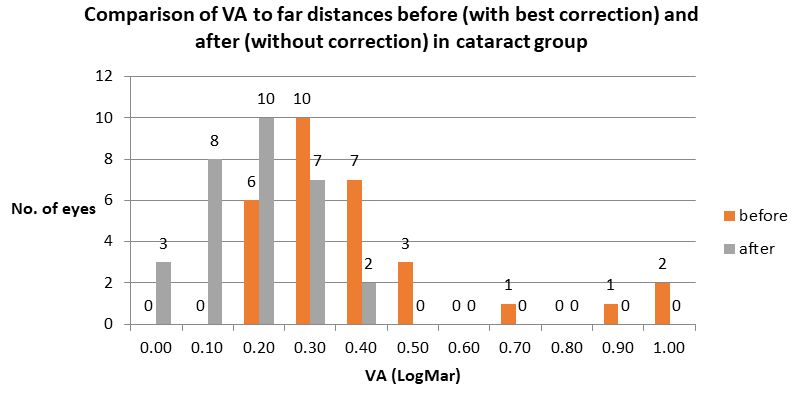
Graph 1a: Comparison of visual acuity values to far distances obtained in the group of patients with cataract. The preoperative values obtained with best correction were compared with postoperative values without correction.
Comment
In none of the patients postoperative visual acuity values were worse than those obtained before surgery. Visual acuity of ≥0.1 was obtained in 11 eyes (36%), ≥0.2 in 21 eyes (70%) out of 30 treated eyes. Two people (3 eyes) achieved visual acuity to far distances not exceeding 0.4. One of them is a patient with high preoperative myopia diagnosed binocularly, with no macular changes; another is a patient with amblyopia. Importantly, in both patients, visual acuity to near distances was normal before the procedure and the ophthalmological history did not indicate the likelihood of amblyopia.
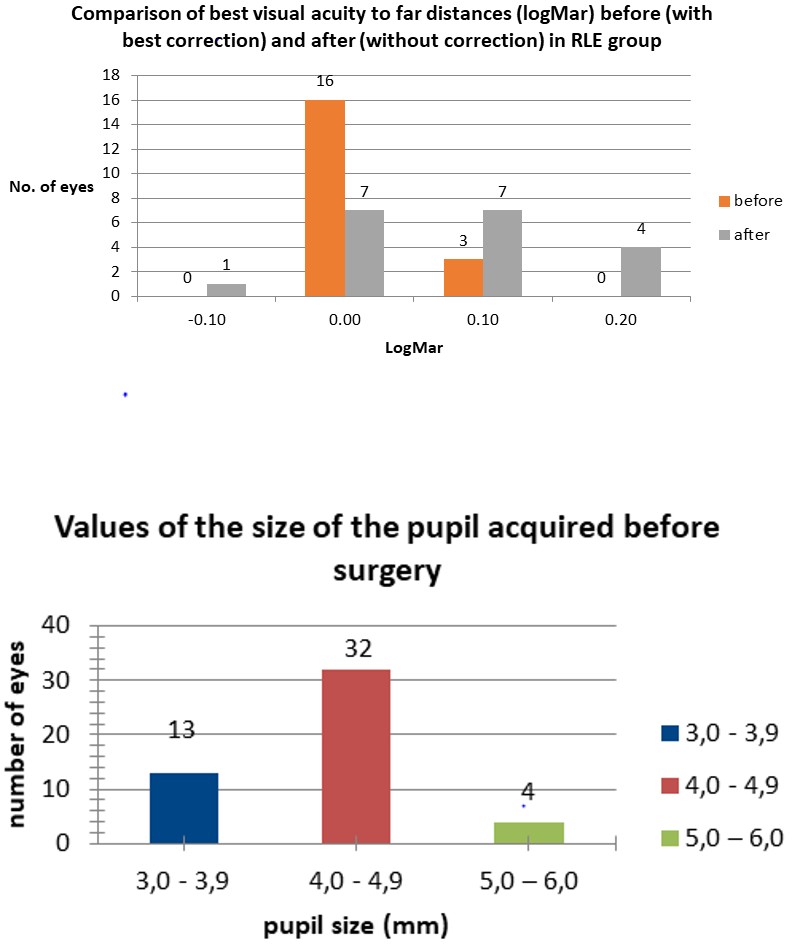
Graph 1b: Comparison of values of visual acuity to far distances obtained in the group of patients after RLE. Preoperative values obtained with best correction were compared with postoperative values without correction.
Comment
Postoperatively, none of the patients, without correction, had visual acuity worse than 0.2. What is noteworthy is the decrease in the value of postoperative visual acuity in relation to preoperative visual acuity in eight eyes in 50% of eyes. In seven eyes the values remained unchanged and only in one person (1 eye) visual acuity improved, reaching the value of -0.1.
Importantly, in the entire group subjected to RLE, only 3 people (4 eyes) stated that their visual acuity to far distances was not satisfactory, although the results obtained in the RLE group could indicate a higher percentage of dissatisfied patients.
Visual Acuity to Near Distances (Snellen)
The mean preoperative value with best correction was =D-0.52 (in the range from 1.0 to 0.5), and after the procedure, without correction, it was = D-0.54 (in the range from 1.0 to 0.5). However, these changes were not statistically significant.
Monocular PanOptix lens Implantation
In 3 patients with slight preoperative hyperopia (aged 43-45), who did not tolerate any correction both too far and near distances, lens implantation allowed them to “regain” visual acuity to near distances, albeit monocularly, giving independence from the use of glasses in everyday functioning. In the next three patients with preoperative high myopia at the level of -9.5Dsph to -19.5Dsph, visual acuity improved incomparably in relation to the condition before the procedure, but these patients used additional correction to near distances (+0.5 - +1.5 Dsph) when they wished to read for a long time.
Pupil Size before the Procedure vs Visual Acuity after the Procedure
Preoperative pupil size values ranged from 3.0 to 6.0 mm, 4.26 mm on average. The number of patients and pupil size are presented in a Graph 2.
Graph 2: Values of the size of the pupil acquired before surgery.
A very strong, statistically significant correlation between the postoperative improvement in visual acuity to far and near distances and the preoperative increase in pupil size be observed in 14 patients with preoperative hyperopia.
Similarly, a very strong, statistically significant correlation was found between the increase in pupil size as assessed preoperatively and the postoperatively assessed decrease in visual acuity to far and near distances in eight eyes diagnose with corneal astigmatism. However, a small number of eyes with this condition does not allow to draw specific conclusions. In the remaining cases, a noticeable weak, however not statistically significant correlation between the increasing pupil size and the decrease in visual acuity to far and near distances was found.
Angle Kappa (Mm) before the Procedure and Visual Acuity after the Procedure
Angle kappa informs us about the position of the pupil center in relation to the visual axis. The mean value for the study group is 0.323, ranging from 0.096 to 0.594. There was a weak, correlation, however not statistically significant, between the increase in the angle and the decrease in visual acuity to far and near distances in most cases.
Angle Alfa (mm) and Visual Acuity to Far and near Distances after the Procedure
This angle defines the position of the eyeball axis in relation to the visual axis. The mean value is 0.386, ranging from 0.024 to 0.694. The increase in the angle size showed a weak correlation with the decrease in visual acuity to far and near distances. No statistical significance was found in any of the studied groups.
Visual Acuity to Intermediate Distances
None of the patients who were asked to read the text from a computer had a problem reading standard font at a distance of 60-80 cm, although some patients happened to change the distance at which they read.
Complaints Reported by Patients
All problems with visual acuity and visual impairments are listed in Table 2.
| Complaint | Number of Patients |
|---|---|
| Negative dysphotopsia | 16 |
| Positive dysphotopsia | 3 |
| Dissatisfaction of VA to far distances | 2 |
| Dissatisfaction of VA to near distances | 3 |
| Seeing rings in visual field | 3 |
| Noticeable darker image in the eye after the procedure | 2 |
Table 2: Problems with visual acuity and visual impairments.
It was noticed that the number of reported complaints decreased with the patient’s age.
Postoperative Complications
Transient corneal edema - 17 eyes. In most cases, it was not noticeable during the second postoperative follow-up, i.e., after 7-9 days; it affected patients with cataract. It is worth noting that each of the patients had an endothelial cell examination performed as standard before the procedure. In the case of the count lower than 2000/mm2, viscoelastics with increased density were used intraoperatively.
The lens capsule folds were found on the first postoperative day in 30 eyes, mainly in myopic eyes. The folds practically disappeared in all cases about 2 months after the procedure. Glistening was observed in 2 patients (2 eyes) 12 months after the procedure.
Discussion
Correction of aphakia after cataract removal is increasingly often performed with the use of premium class, intraocular lenses, although this is still only a fraction of all procedures. In the case of correction of aphakia aimed at getting rid of an unwanted refractive error, the use of premium lenses is already standard. As shown by, among others, this study, the PanOptix and PanOptix toric lens is a product that gives good, stable results in terms of visual acuity to far, near, and intermediate distances. It allows for the correction of refractive errors in eyes with a large pupil size of up to 6mm. Also, high values of angle kappa, up to 0.6 mm, and angle alpha, reaching even 0.7 mm, did not cause radical changes in visual acuity.
Despite good vision parameters that patients can obtain after the implantation of this lens model, its use is associated with the possibility of a number of adverse postoperative consequences (Table 2). However, one should consider it and ask him/herself a question: do we know any ideal method of correcting refractive errors?
In the case of the presence of cataract, we have only one effective option of treatment cataract removal. The implantation of a monofocal lens “condemns” the patient to the need for additional correction to far, intermediate or near distances, in virtually every case. However, in the case of patients with severe hyperopia and accompanying astigmatism, and additionally very high angle alpha values, exceeding 0.700 mm, according to our own experience, a toric monofocal lens seems to be the product of choice.
Correction of refractive errors has a wider, surgical, and non-surgical dimension. Many patients, in the presence of a refractive error, use progressive glasses as a form of non-surgical correction of the error. This form of non- surgical correction could be compared to surgical correction with implantation of intraocular trifocal lens. Is it really possible to compare these two forms of correction when it comes to quality of vision? No, it is not. Despite more and more advanced technology, progressive glasses have many limitations. Not very wide channels of progression and visual field, the need to rotate the head to see well from side to side, the need to move the eyes up or down depending on the selected distance from which we want to see, presence of aberrations, the size of which increases with the size of corrected error are only some of the limitations. Someone, who don’t like surgical correction may say that they can always take off such glasses and … then their visual acuity drops to a level depending on the size of the corrected error, sometimes to very low values. Considering the current ‘COVID” times when the use of protective facial masks is standard, streamy eyeglass lenses constitute one of the most important reasons that prompts patients to consider the surgical form of correction of an existing refractive error. Aberrations caused by eyeglass lenses reduce the range of the field of vision and distort the image at the edges, which can make it difficult to work on a computer [6]. Thus, this type of correction is not a “perfect” method, and in the case of more technologically advanced products, it additionally places a heavy burden on the customer’s pocket. Of course, one can opt out of correction with progressive glasses and use two or three pairs of monofocal glasses.
What is concerning about the use of the PanOptix model is the appearance of glistening phenomenon just one year after its implantation. The problem of glistening concerns mainly lenses made of a hydrophobic material. There is no single classification according to which the observed degree of this phenomenon can be estimated. Literature presents scales by for example Christiansen and Miyata [7, 8]. Data on the influence of glistening on visual acuity and quality of vision is divergent. One of the studies shows no effect on vision [9, 10]. Godlewska A, et al. [11] noticed a relationship between the scope of glistening and lens refractive power or coexisting diseases, e.g. diabetes. Subsequent studies have shown a decrease in visual acuity, especially in patients with more micro vacuoles, above the level of 2, according to the Christiansen scale [8, 12]. Geniusz M, et al. [13] believes that glistening reduces contrast sensitivity. Taking into account the above research results and the relatively young age of patients undergoing RLE procedures, glistening progressing over time is not a symptom that can be ignored. Over the next 20-30 years of “using” the lens, it can significantly and adversely affect quality of the patient’s vision. Therefore, one should be very careful with the use of these lenses in the correction of postoperative aphakia in people aged 40- 50. As Alcon Company already has products in which the level of “development” of glistening over time is significantly reduced (Clareon®-monofocal lens), we can hope that PanOptix models will also be manufactured using the same material [14].
A very small group of patients was not entirely satisfied with achieved visual acuity to far distances. It should be emphasized here that among these people there were patients who, despite the presence of a small defect of hyperopia (to far distances) of +1.0-2.0Dsph, did not apply any correction because they did not accept glasses or contact lenses. Postoperative correction of such an eye defect to the level of 0.0Dsph, additionally applied in the dominant eye, will always be perceived as the cause of deteriorated vision. Therefore, taking into account our own experience and the results described in this study, one should be very careful about surgical correction of mild hyperopia. If a patient with mild hyperopia wants to “regain” visual acuity to near distances, surgical correction should begin with the non- dominant eye. This in many cases is enough for everyday functioning.
Adverse symptoms, such as negative or positive dysphotopsia, are among the most frequently observed adverse consequences. These symptoms become less noticeable over time. It is worth mentioning that the appearance of dysphotopsia does not depend on the model and structure of the intraocular lens, but only on the size of the lens optics.
Conclusion
Correction of an aphakic eye with the use of PanOptix and PanOptix toric models allows us to obtain stable results in terms of visual acuity to far, near, and intermediate distances, and it is practically independent of pupil size of 3-6 mm. A significant negative correlation between improvements in visual acuity to far and near distances and increasing pupil size was observed in eyes with preoperative hyperopia. A slight negative effect on visual acuity to far and near distances was observed in the eyes with high angles alpha, although even at values of up to 0.7 mm, visual acuity did not change statistically. In the case of angle kappa, a similar weak correlation was found, despite the fact that the angle values reached 0.6 mm. Postoperative deterioration of visual acuity to far distances in RLE eyes is noticeable, but in most cases, it does not affect the assessment of the quality of vision in these patients. For most patients with cataract formation, visual acuity and quality of vision were fully acceptable. Only patients with preoperative high or moderate myopia “lacked” a small addition to near distances, especially in the first months after surgery.
References
-
AcrySoft®IQ PanOptix® PRESBYOPIA CORRECTING IOL. Illustrative material of Alcon in the form of a PowerPoint presentation.
-
AcrySoft®IQ PanOptix®Trifocal IOL. Clinical Science Compendium. Summary of peer-reviewed clinical and bench research. Promotional materials of Alcon.
-
Cywinski A (2021) The Influence of Angles Kappa and Alpha and Pupil Size on Vision after Implantation of Soleko Evolve and Lucidis Lenses with a “Pure” EDOF Structure. J Ophthalmol and Adv Res 2(2): 1-12.
-
Salerno LC, Tiveron MC, Alio JL (2017) Multifocal intraocular lenses: Types, outcomes, complications and how to solve them. Taiwan J Ophthalmol 7(4): 179-184.
-
Cywinski A (2020) Usefulness of Itrace in Diagnosing Unclear Cases of the Deterioration in Visual Acuity. Congenital Lens Dysfunction as a New Disease Entity. Preliminary Reports. Journal of Bioscience & Biomedical Engineering 1(3): 1-9.
-
Rojek K (2017) Analiza przyczyn braku adaptacji do soczewek progresywnych na wybranych przykładach (Analysis of the reasons for the lack of adaptation to progressive lenses on selected examples), part I Optics 5: 62-65.
-
Miyata A, Uchida N, Nakajima K, Yaguchi S (2001) Clinical and experimental observation of glistening in acrylic intraocular lenses. Jpn J Ophthalmol 45(6): 564-569.
-
Christiansen G, Durcan FJ, Olson RJ, Christiansen K (2001) Glistenings in the AcrySof intraocular lens: pilot study. J Cataract Refract Surg 27(5): 728-733.
-
Stanojcic N, O’Brart DPS, Maycock N, Hull CC (2019) Effects of intraocular lens glistenings on visual function: a prospective study and presentation of a new glistenings grading methodology. BMJ Open Ophthalmol 4(1): e000266.
-
Colin J, Praud D, Touboul D, Schweitzer C (2012) Incidence of glistenings with the latest generation of yellow-tinted hydrophobic acrylic intraocular lenses. J Cataract Refract Surg 38(7): 1140-1146.
-
Godlewska A, Owczarek G, Jurowski P (2016) Glistening phenomenon in acrylic hydrophobic intraocular lenses how do perioperative factors and concomitant diseases effect it’s incidence and severity. Klin Oczna 118(3): 191- 196.
-
Henriksen BS, Kinard K, Olson RJ (2015) Effect of intraocular lens glistening size on visual quality. J Cataract Refract Surg 41(6): 1190-1198.
-
Geniusz M, Zajac M (2017) Influence of glistening and calcium deposits in artificial intraocular lenses on retinal image quality numerical model. Optica Applicata 47(3): 341-350.
-
Lehmann R, Maxwell A, Lubeck DM, Fong R, et al. (2021) Effectiveness and Safety of the Clareon Monofocal Intraocular Lens: Outcomes from a 12-Month Single- Arm Clinical Study in a Large Sample. Clin Ophthalmol 15: 1647-1657.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report