In vitro Evaluation of a Hypobromous Acid Hygiene Stabilized Solution in the Reduction of Bacterial Load Associated to Blepharitis Conditions
Aims: Blepharitis is a chronic inflammation of the periocular skin area and it is characterized by eye itching, burning, dryness and irritation, with progression to chronic dry eye syndrome, where the eyelids margins of blepharitis patients are frequently colonized by bacteria. The aim of the present study was to investigate the in vitro bactericidal activity (BA) of a stabilized active bromine solution (MDI-102) at neutral pH for the potential use in the treatment and prevention of blepharitis. Methods and Results: The kinetic experiments have been conducted both in clean and in dirty conditions (by using bovine albumin solution as the interfering substance) at different ranges of concentration. The results show the topical solution to be capable of inactivating, in less than 0.5 minutes, more than 99.9% of several bacterial species involved in the clinical manifestations of blepharitis: Enterococcus hirae, Escherichia coli, Pseudomonas aeruginosa, Staphylococcus aureus, Staphylococcus epidermidis, and Serratia marcescens. Dirty condition tests confirm the results shown without albumin (clean conditions). Conclusions: MDI-102 is considered not irritating and dermatologically tested. This study demonstrates that MDI-102 active bromine solution can markedly reduce (in vitro) the bacterial activity, responsible of clinical manifestation of blepharitis. Thus, MDI-102 can be considered a promising tool for the periocular area and eyelids cleaning for blepharitis patients. Significance and Impact of the Study: The use of this formulation may contribute in the long-term prevention and hygienic treatment of blepharitis condition. Furthermore, MDI-102 can be considered as an alternative to reduce the use and the abuse of topical antibiotics in the daily practice, which may contribute to the increase of resistance to the antibiotics in the clinical setting
Introduction
Blepharitis is a chronic inflammation of the periocular skin area, which includes eyelids and sometimes eyelashes and may involve the Meibomian glands [1]. This condition is a very common ocular disorder [2] and it is characterized by eye itching, burning, dryness and irritation, with progression to chronic dry eye syndrome [2, 3, 4].
Meibomian gland dysfunction is the most common aspect of posterior blepharitis [5] and the local microbiome plays an important role in the clinical manifestation of this condition [6]. This is the reason why topical antibiotics can be used to reduce the bacterial load and provide symptomatic relief [7].
The eyelids margins of blepharitis patients are frequently colonized by bacteria, predominantly by Gram- positive bacteria, including species of Staphylococcus, Propionibacterium (Cutibacterium) and Corynebacterium spp [8, 9, 10].
Current standard treatment of initial blepharitis includes the use of antibiotics [7] however, the mainstay of the treatment is an eyelid hygiene regimen, which needs to be continued long term to prevent recurrence of the disease [11]. An effective solution for the eyelid and eyelash hygiene thus represents a valid tool to reduce the use, and the abuse, of topical antibiotics in the daily practice, which may contribute to the increase of resistance to the antibiotics in the clinical setting [12].
Hypobromous acid (HBrO) is a weak, inorganic acid mainly produced and handled in aqueous solution. HBrO is used as bleach, oxidizer, deodorant, and disinfectant, due to its ability to kill the cells of many pathogens [13]. The opportunity to test the use of HBrO in the hygiene treatment of blepharitis has the following rationale:
- HBrO was proven to induce lysis of blood cells at approximately 10-fold lower concentration than HClO [14]. Furthermore, in general, bromine compounds show higher bactericidal efficacy compared to chlorine solutions [15, 16];
- Bromine is less toxic than chlorine [17];
- Bromine and HBrO are more stable at neutral pH and more compatible with the physiological pH of the periocular skin area, compared to HClO solutions, used in the same setting [18];
- Br-species are more effective bactericidal on acneic skin compared to Cl-species [15, 19, 20].
All these background data, suggest that active bromine compounds are very potent oxidants and that they clearly excel their chlorine analogues.
This study describes the effect of active bromine compounds (Br2, HBrO/BrO-) stabilized solution, concentration ranged between 0.005% and 0.05%, on bacterial species involved in the periocular skin flora. The aim of the present work is to test this active bromine compounds solution, named MDI-102, for its potential use for the treatment and prevention of blepharitis.
Materials and Methods
Chemicals and Solution Preparation
KBr was purchased by CARLO ERBA Reagents, H3PO4 (85%) was from Merck-Sigma Aldrich, while the NaClO (3%) was a commercial hypochlorite used for water intended for human consumption (in compliance with UNI EN 901:2013).
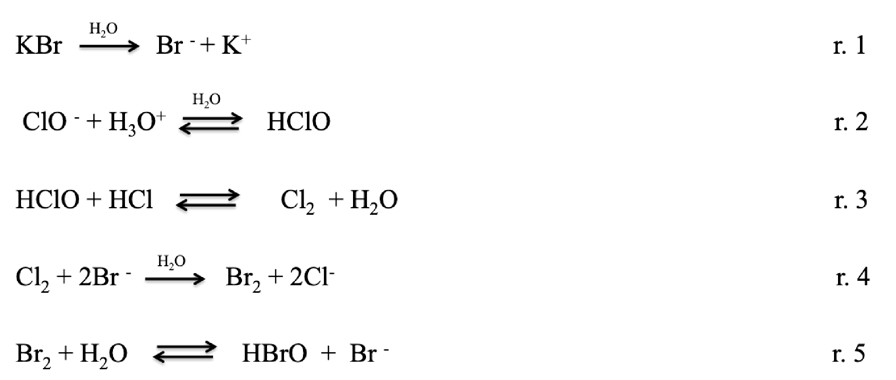
The albumin, used for the dirty test, was purchased by VWR. The present solution, named MDI-102, consists in active free bromine solution (Br2, HBrO/BrO-) in a concentration ranged between 50 and 550 ppm. MDI-102 was prepared as follows. KBr (0.1-1%), phosphoric acid solution (H3PO4 85%) 0.05-0.5% and sodium hypochlorite (NaClO al 3%) 0.005-0.05% were mixed in ultra-pure water solution (90-99%). The reactions occurring in the solution during the preparation are outlined in (Figure 1). Briefly, KBr dissolved in water, forms Br- and K+ (r. 1). After the addiction of hypochlorite, and the chlorine formation in water (r. 2-3), the bromide reacts with the chlorine forming Br-, HBrO, Br2 and Cl- (r. 4-5), which are the main components of the solution MDI-102. Furthermore, as previously described, due to the excess of KBr compared to the hypochlorite, all the ClO- can be considered converted to Cl-; it follows that the only antimicrobial effect is due to Br-based species.
Due to the low NaClO stability, the hypochlorite concentration is always analysed before the solution preparation. The free halogen concentration has been assessed using Hach Lange kit. The kit measures the free halogen concentration as follow. The N, N-diethyl- p-phenylenediamine, in the kit, is oxidized by the free halogen making a reddish compound which absorbs at 510
nm. The concentration is measured using Hach DR6000 spectrophotometer (cuvette with 2.5cm optical path length).
Kinetic Test
Kinetic test was performed in order to test the bactericidal activity (BA) of MDI-102, using the bacterial strains reported by: • Standard UNI EN ISO 11930:2019 (Evaluation of the antimicrobial protection of cosmetics);
• Standard UNI EN 1276:2019 (Quantitative suspension test for the evaluation of bactericidal activity of chemical disinfectants and antiseptics used in food, industrial, domestic and institutional areas);
• Standard UNI EN ISO 14729:2010 (Contact lens care products - Microbiological requirements and test methods for products and regimens for hygienic management of contact lenses);
• Stroman DW, et al. [21] (blepharitis treatments products) and Groden LR, et al. [10] (blepharitis flora).
The tested microorganisms were:
- Pseudomonas aeruginosa ATCC: 9027 (UNI EN ISO 11930:2019),
- Enterococcus hirae ATCC: 10541 (UNI EN 1276:2019),
- Serratia marcescens ATCC: 13880 (UNI EN ISO 14729:2010),
- Staphylococcus aureus ATCC: 6538 (UNI EN 1276:2019),
- Pseudomonas aeruginosa ATCC: 15442 (UNI EN 1276:2019),
- Escherichia coli ATCC: 8739 (UNI EN ISO 11930:2019),
- Staphylococcus epidermidis ATCC: 12228 [21].
MDI-102 bactericidal activity was tested at 500 and 80 ppm (active bromine concentration). Microorganisms were inoculated at concentration ranged between 2x105 and 3x107 colony-forming unit (CFU) mL-1 [21]. Microbial concentration was monitored at different times: 0.5, 1, 2, 5, 20, 30 minutes after the addition of the bactericidal solution (MDI-102). After the selected time a neutraliser was added as inactivator. A blank test (control) without the bactericidal solution was carried out before each test in order to assess the initial microbial concentration, thus to monitor the microbial concentration over time. All the tests were carried out in triplicates; the standard error for all the tests was ranged between zero and 1.5%.
Tests were performed at 25±1°C, room temperature. After the fixed time, a solution aliquot was sampled, inoculated on a Petri dish and incubated at 36±1°C for 48 h.
These tests are following referred as “clean tests”.
Kinetic tests were also carried out in “dirty condition” in order to assess the solution’s BA effectiveness under real conditions. Dirty tests were performed adding albumin (3gL-1) as interfering substance (UNI EN 1276:2019). The tests were carried out as previously described, thus with same microorganisms’ strains and concentration, times, temperatures, etc.; the only difference between the clean and the dirty condition was the presence of albumin in the dirty condition tests. The dirty condition tests were carried out using the only MDI-102 at 80 ppm (MDI-10280ppm) solution because it has been considered sufficient to prove the bactericidal solution effectiveness. In fact, if MDI-10280ppm is effective in dirty condition, the solution at higher active bromine concentration (MDI-102500ppm) must be effective as well.
Skin Tolerability
Skin tolerability has been assessed in order to check if the bactericidal solution could cause any undesired skin inflammation. This allergy test, known as Patch test, was carried out in compliance with the following ethical requirements: • All of the subjects participating in the study are healthy volunteers (at least 18 years old);
• All of the subjects participating in the study are selected under the supervision of a dermatologist according to inclusion/non-inclusion criteria (see the paragraph “Inclusion criteria” and “Non-inclusion criteria”);
• The participation of volunteers in the study is completely free;
• All of the subjects participating in the study are informed about the purpose and nature of the study;
• All of the subjects participating in the study are informed of the potential risks involved;
• All of the subjects participating in the study give their informed consent signing at the beginning of the study;
• Before the start of the test, all relevant safety information about the product itself and each ingredient are collected and evaluated;
• All procedures are performed in accordance with the ethical principles for the medical research [22];
• All necessary precautions are taken to avoid adverse skin reactions;
• If unexpected/adverse skin reactions occur, the dermatologist evaluates the severity of the reaction (and report it in the data collecting sheet) and if necessary, proceed with the appropriate therapy.
MDI-102500ppm was tested on 20 volunteers. The volunteers were recruited to take part in the test in accordance with the following inclusion and exclusion criteria (see 5.3.1., 5.3.2., 5.3.3.). Furthermore, during patch application and 24 hours after patch removal, volunteers must avoid situations or activity that could interfere with the evaluations: • Exposition to the sun or solarium;
• Sport activity;
• Immersion in water or steam bath;
• Rubbing and mechanical or thermal stresses in the skin area, where the patch was applied.
Inclusion Criteria: The inclusion criteria for the Patch test were: • Male and/or female subjects;
• Subjects between 18 and 70 years old;
• Healthy subjects;
• Subjects informed about the purpose of the study.
Exclusion Criteria: The exclusion criteria for the patch test were: • Subjects who do not fit the inclusion criteria;
• Subjects with marks (for example tattoos, scars, burns) in the tested skin region, which might interfere with clinical evaluation;
• Subjects with dermatological problems in the tested area;
• Subjects with medication that can interfere with the skin response;
• Subjects undergoing pharmacological treatment (both locally or systemically);
• Subjects with past history for contact dermatitis;
• History of positive atopy;
• Pregnant and breastfeeding women.
Withdrawal Criteria: Participants are withdrawn if: • They do not follow the conditions of the Study Information Sheet that they receive after the recruitment;
• They suffer any illness or accident or develop any condition during the study which could affect the outcome of the study;
• They no longer wish to participate in the study.
Clinical Examination: The product, as it is, is applied using a Finn Chamber. The Finn Chamber is fixed to the skin using a patch already tested for its harmlessness. The quantity of product applied is sufficient to saturate the paper disk, avoiding the product to come out of the cell, once applied to the skin. The product is left on the skin surface for 48 hours. The cutaneous reactions are analysed 15 minutes, 1 hour and 24 hours after product removal. A Finn Chamber, containing a blotting paper disk soaked with distilled water, is applied and used as a negative control.
Skin reactions are evaluated 15 minutes, 1 hour and 24 hours after patch removal according to the scores reported in Table 1, that describes the severity of erythema, oedema or other types of skin irritation. For each experimental time Mean Irritation Index (IMM) is calculated by adding erythema mean value and oedema mean value. The tested product is then classified following Table 2 that is based on the Mean Irritation Index.
| 0 | |
|---|---|
| No erythema | 1 |
| Light erythema | 2 |
| Clearly visible erythema | 3 |
| Moderate erythema | 4 |
| Serious erythema | 5 |
| No oedema | 6 |
| Light oedema (hardly visible) | 7 |
| Light oedema | 8 |
| Moderate oedema | 9 |
| Strong oedema | 10 |
Table 1: Clinical score of skin reactions.
| Mean Irritation Index (IMM) | Product Classification |
|---|---|
| < 0.5 | Non irritating |
| 0.5 - 2.0 | Slightly irritating |
| 2.0 - 5.0 | Moderately irritating |
| 5.0 - 8.0 | Highly irritating |
Table 2: Classification of the medium irritation index.
Results
Kinetic Test
Kinetic tests were carried out in order to:
- Assess the BA effectiveness of MDI-102 towards periocular microorganism;
- Determine the time required to kill the microorganisms connected to the blepharitis.
Kinetic tests carried out with MDI-102500ppm are reported in Figures 2 (a-g).
(a)
(b)
(c)
(d)
(e)
(f)
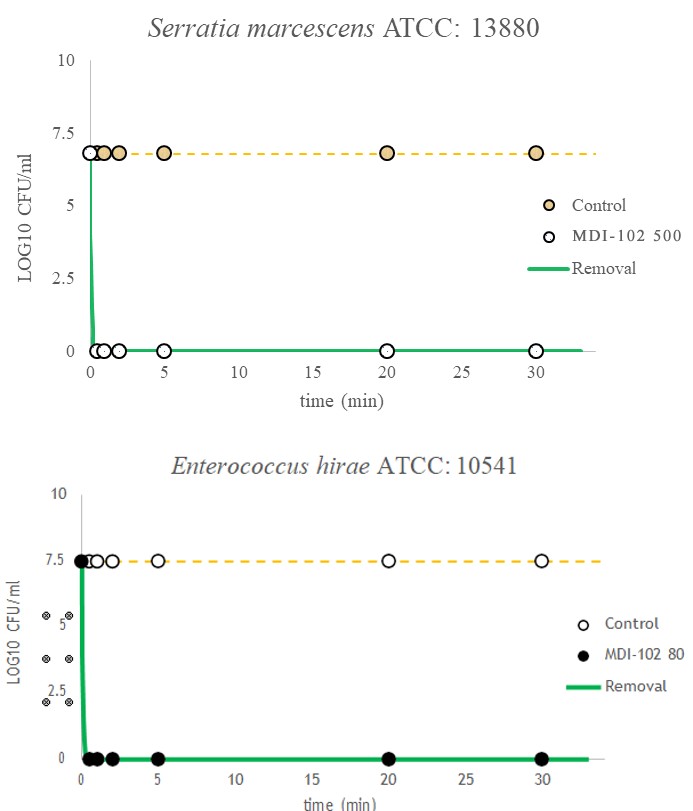
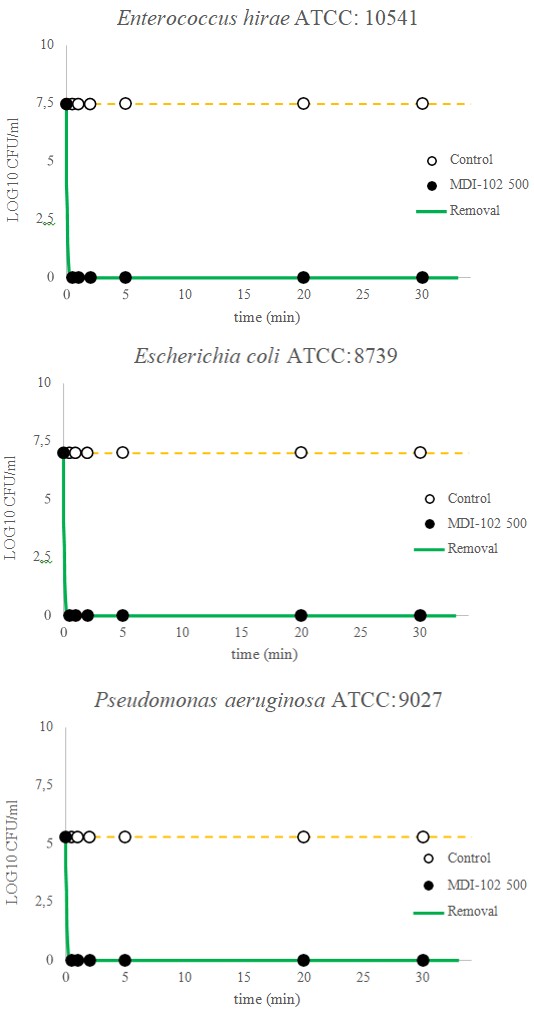
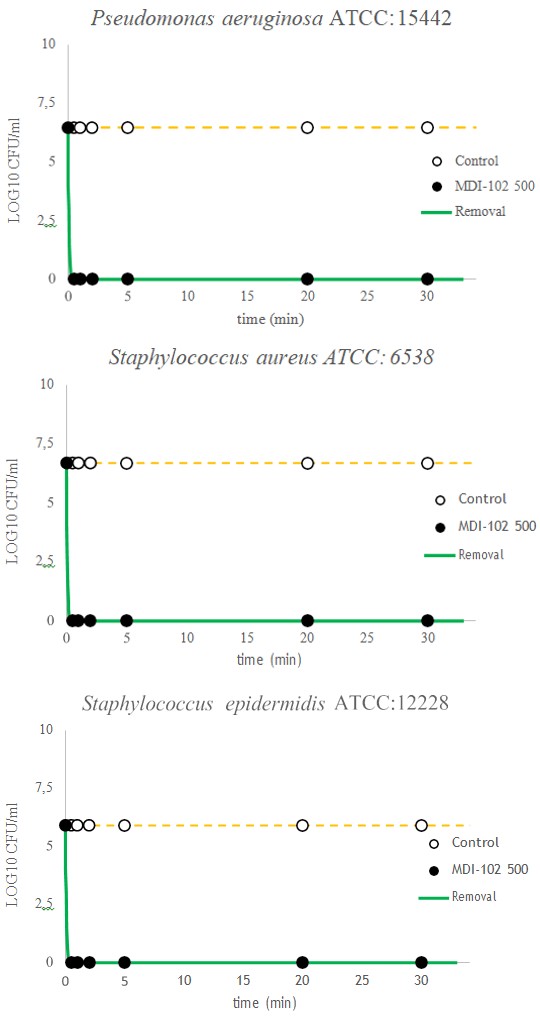
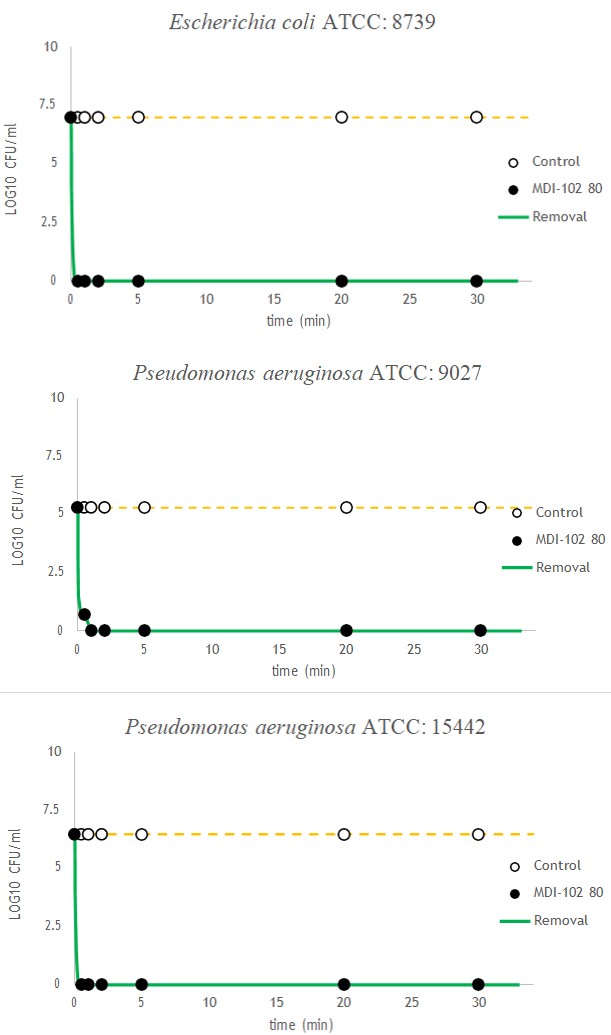
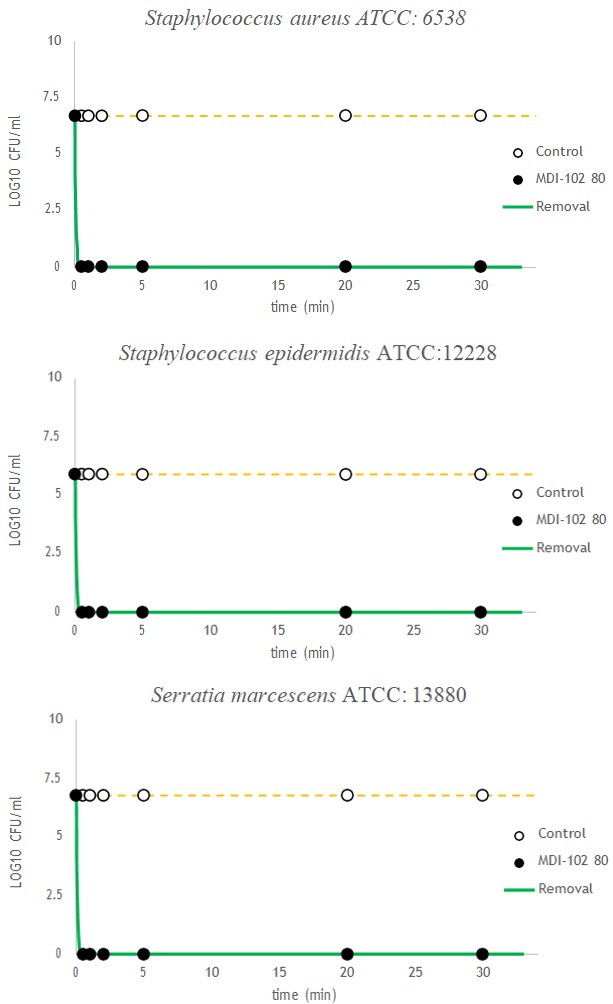
(g) Figure 2 (a-g): MDI-102 (500 ppm) kinetic tests with the following microorganisms: (a) Enterococcus hirae ATCC: 10541, (b) Escherichia coli ATCC: 8739, (c) Pseudomonas aeruginosa ATCC: 9027, (d) Pseudomonas aeruginosa ATCC: 15442, (e) Staphylococcus aureus ATCC: 6538, (f) Staphylococcus epidermidis ATCC: 12228, (g) Serratia marcescens ATCC: 13880. The white dots (yellow dashed line) represent the “control” or blank which are the microorganisms’ trend without MDI-102 (bactericidal solution) along with time. The black dots represent the microbial concentration trend along with time with MDI- 102500ppm (concentration of active free Br). The green line shows the kinetic bactericidal trend along with time.
The black dots represent the microbial concentration trend along with time with MDI-102500ppm (concentration of active free Br). The green line shows the kinetic bactericidal trend along with time.
Figures 2 (a-g) shows that MDI-102 (500 ppm) can effectively remove the inoculated microbial concentration, ranged between 105 and 107 CFUmL-1, after only 30 seconds of contact (100% of removal) between the microorganisms and the bactericidal solution. Indeed, after 30 seconds, 0 CFU are determined in the Petri dish.
The same results are shown with the tests with MDI- 10280ppm, as reported in Figures 3 (a-g).
(a)
(b)
(c)
(d)
(e)
(f)
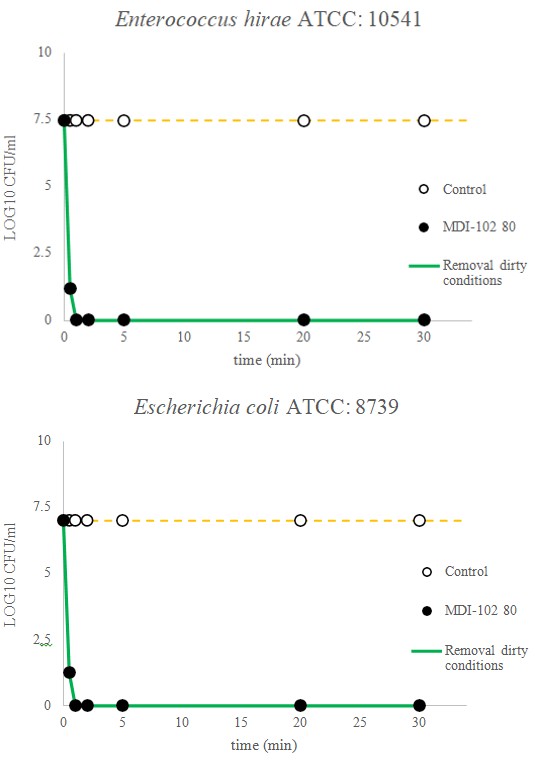
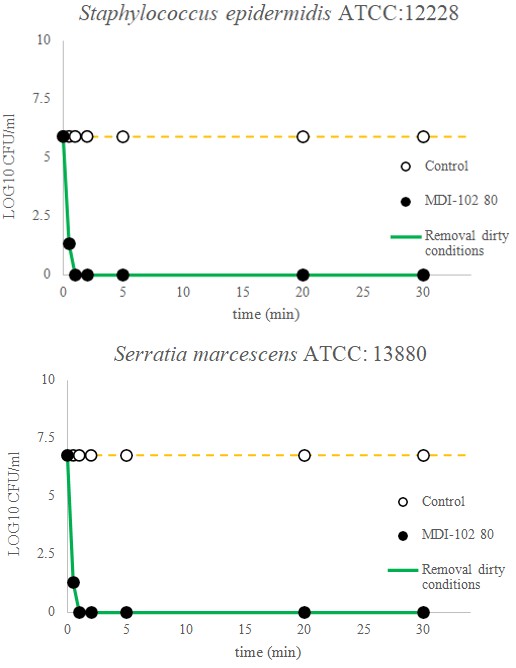
(g) Figure 3(a-g): MDI-102 (80 ppm) kinetic tests with the following microorganisms: (a) Enterococcus hirae ATCC: 10541, (b) Escherichia coli ATCC: 8739, (c) Pseudomonas aeruginosa ATCC: 9027, (d) Pseudomonas aeruginosa ATCC: 15442, (e) Staphylococcus aureus ATCC: 6538, (f) Staphylococcus epidermidis ATCC: 12228, (g) Serratia marcescens ATCC: 13880. The white dots (yellow dashed line) represent the “control” or blank which are the microorganisms’ trend without MDI-102 (bactericidal solution) along with time. The black dots represent the microbial concentration trend along with time with MDI- 10280ppm (concentration of active free Br). The green line shows the kinetic bactericidal trend along with time.
Figures 3 (a-g) shows after 30 seconds a concentration equal to zero for all the tested microorganisms (100% of removal after 30 seconds) with the exception of the Pseudomonas aeruginosa (ATCC:9027): its concentration after 30 seconds is indeed 5 CFU mL-1. On the other hand, considering a Pseudomonas aeruginosa (ATCC: 9027) starting concentration equal to 2*105 CFU mL-1 the removal % is 99.998% after just 30 seconds. MDI-10280ppm thus can be considered as effective as the MDI-102500ppm solution.
Bactericidal kinetic tests were carried out also in dirty conditions (see paragraph 6.2). The selected microorganisms were put in contact with MDI-10280ppm and 3 g L-1 of albumin, as protein-disruptor; the effectiveness of halogenated biocidal product is indeed often tested with peptone16. Figures 4 (a-g) shows the tests in dirty conditions.
(a)
(b)
(c)
(d)
(e)
(f)
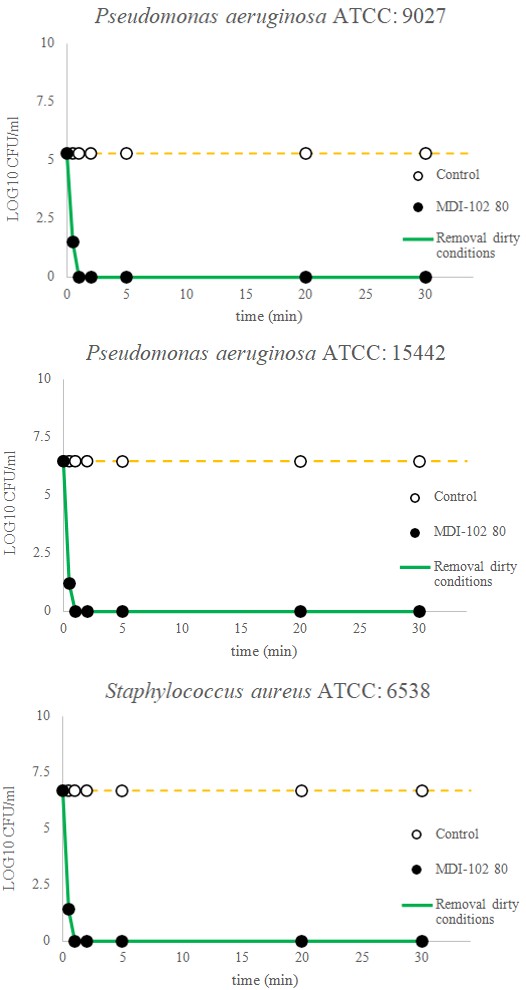
(g) Figure 4(a-g): MDI-102 (80 ppm)+albumin 3 g L-1 kinetic tests with the following microorganisms: (a) Enterococcus hirae ATCC: 10541, (b) Escherichia coli ATCC: 8739, (c) Pseudomonas aeruginosa ATCC: 9027, (d) Pseudomonas aeruginos_a ATCC: 15442, (e) _Staphylococcus aureus ATCC: 6538, (f) Staphylococcus epidermidis ATCC: 12228, (g) Serratia marcescens ATCC: 13880. -The white dots (yellow dashed line) represent the “control” or blank which are the microorganisms’ trend without MDI-102 (bactericidal solution) + albumin 3 g L-1 along with time. The black dots represent the microbial concentration trend along with time with MDI-10280ppm (concentration of active free Br). The green line shows the kinetic bactericidal trend of along with time in dirty condition.
The white dots (yellow dashed line) represent the “control” or blank which are the microorganisms’ trend without MDI-102 (bactericidal solution) + albumin 3 g L-1 along with time. The black dots represent the microbial concentration trend along with time with MDI-10280ppm (concentration of active free Br). The green line shows the kinetic bactericidal trend of along with time in dirty condition.
Dirty condition tests have confirmed the results shown without disruptor (clean condition tests): MDI-10280ppm can effectively remove more than 99.98% of the concentration of Enterococcus hirae ATCC: 10541, Escherichia coli ATCC: 8739, Pseudomonas aeruginosa ATCC: 9027, Pseudomonas aeruginosa ATCC: 15442, Staphylococcus aureus ATCC: 6538, Staphylococcus epidermidis ATCC: 12228, and Serratia marcescens ATCC: 13880, after only 30 seconds.
Skin Tolerability
Tables 3 & 4, listed below, contain the values of the erythema and oedema indices recorded for each volunteer. Potential skin irritation of the product was assessed according to the amended classification. Based on the results obtained, MDI-102 is considered non irritating and dermatologically tested, that means it can be promisingly used to clean the periocular area and for the blepharitis syndrome.
| Volunteers | Sex | Erythema 15’ | Oedema 15’ | Erythema 1h | Oedema 1h’ | Erythema 24h | Oedema 24h |
|---|---|---|---|---|---|---|---|
| MAF001 | M | 1 | 0 | 1 | 0 | 1 | 0 |
| MAF002 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF003 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF004 | F | 1 | 0 | 1 | 0 | 1 | 0 |
| MAF005 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF006 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF007 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF008 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF009 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF010 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF011 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF012 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF013 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF014 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF015 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF016 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF017 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF018 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF019 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF020 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF001 | M | 1 | 0 | 1 | 0 | 1 | 0 |
| MAF002 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF003 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF004 | F | 1 | 0 | 1 | 0 | 1 | 0 |
| MAF005 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF006 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF007 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF008 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF009 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF010 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF011 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF012 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF013 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF014 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF015 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF016 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF017 | F | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF018 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF019 | M | 0 | 0 | 0 | 0 | 0 | 0 |
| MAF020 | F | 0 | 0 | 0 | 0 | 0 | 0 |
Table 3: Oedema and Erythema reactions on 20 volunteers (SEX: F= female, M= male).
| 0.1 | |
|---|---|
| Erythema Irritation index mean values 15' | |
| Erythema Irritation index mean values 1h | 0.1 |
| Erythema Irritation index mean values 24h | 0.1 |
| Oedema Irritation index mean values 15' | 0 |
| Oedema Irritation index mean values 1h | 0 |
| Oedema Irritation index mean values 24h | 0 |
Table 4: Mean values for erythema and oedema.
Discussion and Conclusion
This study showed MDI-102 can effectively remove common eyelid bacteria connected to blepharitis. A single application with 0.008% HBrO led to a complete removal (100% reduction) of bacterial load after 60 seconds (99.998% removal after 30 seconds).
Of particular interest are S. epidermidis and S. aureus data, which can be considered two strong indicators of blepharitis syndrome [8, 16, 21, 23, 24, 25]. The results have been compared with the literature study carried out by Stroman DW, et al. [21], which tested an HClO (0.01%) solution for the periocular area hygiene. Stroman DW, et al. [21] tested the solution with several periocular microorganisms at concentration ranged between 105 and 107 CFU mL-1 (same concentration range of the current study) and showed that the hypochlorite solution (100 ppm) can effectively kill more than the 99% of Staphylococcus species after 20 minutes and, in detail, a concentration higher than 99.5% of Staphylococcus epidermidis. MDI 10280ppm (active halogen 20 ppm lower than the solution tested by Stroman DW, et al. [21]) can remove, after just 30 seconds (thus an interval of time 97.5% lower than the one chosen by Stroman DW, et al. [21]), the 99.99% of the tested microorganisms’ concentration (average calculated on all the tested microorganisms).
A single MDI 10280ppm application is thus enough to kill the blepharitis microorganism of concern. MDI 10280ppm has shown a microbial removal, at least, comparable to the commercially available bactericidal solution Chlorine- based and a much faster kinetic removal. This is particularly convenient because it allows killing the blepharitis related microorganisms in a shorter time after the product application. Furthermore, the lower bromine toxicity, compared to chlorine, makes MDI 10280ppm potentially more tolerable for the skin than the commercially available competitors chlorine based.
MDI 10280ppm was also tested in dirty condition to check its effectiveness in real conditions. Data have shown that albumin does not interfere with MDI 10280ppm BA; the bromine-based solution can effectively kill the 99.98% of the tested bacteria indeed. No comparable kinetic study has been carried out with chlorine-based solutions in “dirty conditions”, thus no further comparison is possible. On the other hand, Gottardi W, et al. [16] compared the bactericidal activity of N-bromine compounds to the N-chlorine compounds in presence of peptone. The tested compounds were: dichloro‐ and dibromoisocyanuric acid, chlorantine and bromantine (1,3‐dibromo‐ and 1,3 dichloro‐5,5‐dimethylhydantoine), chloramine T and bromamine T (N‐chloro‐ and N‐bromo‐4‐ methylbenzenesulphonamide sodium), and N‐chloro‐ and N‐bromotaurine sodium. Their study demonstrates that the N-bromine and N-chlorine BA is strictly related to the selected specific compound. Furthermore, the BA of N-bromine compounds decreases in presence of peptone. The present study shows albumin does not lead to a BA loss; the activity is still higher than 99% after the disruptor addition. This aspect might confirm effectiveness is strictly related to the specific compound used as bactericidal.
For the best of our knowledge, it is not possible to carry out a deeper comparison with other literature studies. This aspect confirms the novelty of the present study both in terms of bactericidal solution for blepharitis treatment and in terms of experimental set-up. Furthermore, as well as chorine based bactericidal solutions, this study demonstrates MDI-102 can be used to kill the susceptible strains equally well as those that are resistant to various antibiotics.
A new biocidal solution bromide-based has been developed in this study to treat the blepharitis syndrome. The solution can be effectively used to clean eyelashes, eyelids and the periocular area. MDI-102 represents an effective alternative to the available chlorine-based biocidal solutions. Bromine based solution is more effective (superior and faster bacterial removal), less toxic and more stable than chlorine base solutions.
Last but not least, based on the present in vitro results, as well as chlorine-based bactericidal solutions, MDI 10280ppm can be considered as an alternative to reduce the use and the abuse of topical antibiotics in the daily practice, which may contribute to the increase of resistance to the antibiotics in the clinical setting. Appropriate clinical investigation on the bromine-based solutions in patients with blepharitis syndrome (in vivo study) might be particularly important to be designed, in order to definitively consider the standard use of Br-based biocidal solutions in the clinical practice.
References
-
Wolffsohn JS, Arita R, Chalmers R, Djalilian A, Dogru M, et al. (2017) TFOS DEWS II diagnostic methodology report. Ocular Surface 15(3): 539-574.
-
Lemp MA, Nichols KK (2009) Blepharitis in the United States 2009: a survey-based perspective on prevalence and treatment. Ocular Surface 7(2): S1-S14.
-
Amescua G, Akpek EK, Farid M, Ferrer GFJ, Lin A, et al. (2019) Blepharitis Preferred Practice Pattern®. Ophthalmology 126(1): P56-P93.
-
Cheng AM, Sheha H, Tseng SC (2015) Recent advances on ocular Demodex infestation. Current Opinion in Ophthalmology 26(4): 295-300.
-
Nelson JD, Shimazaki J, Craig JP, McCulley JP, Den, S, et al. (2011). The international workshop on meibomian gland dysfunction: report of the definition and classification subcommittee. Investigative Ophthalmology & Visual Science 52(4): 1930-1937.
-
Watters GA, Turnbull PR, Swift S, Petty A, Craig JP (2017) Ocular surface microbiome in meibomian gland dysfunction. Clinical & Experimental Ophthalmology 45(2): 105-111.
-
Lindsley K, Matsumura S, Hatef E, Akpek EK (2012) Interventions for chronic blepharitis. Cochrane Database of Syst Rev (5): CD005556.
-
Dougherty JM, McCULLEY JP (1984) Comparative bacteriology of chronic blepharitis. British journal of Ophthalmology 68(8): 524-528.
-
McCulley JP, Dougherty JM (1986) Bacterial aspects of chronic blepharitis. Transactions of the Ophthalmological Societies of the United Kingdom 105(3): 314-318.
-
Groden LR, Murphy B, Rodnite J, Genvert GI (1991) Lid flora in blepharitis. Cornea 10(1): 50-53.
-
Jackson WB (2008) Blepharitis: current strategies for diagnosis and management. Canadian Journal of Ophthalmology 43(2): 170-179.
-
Cassini A, Plachouras D, Monnet DL (2019) Attributable deaths caused by infections with antibiotic-resistant bacteria in France-Authors reply. The Lancet Infectious Diseases 19(2): 129-130.
-
Butler A, Walker JV (1993) Marine haloperoxidases. Chemical Reviews 93(5): 1937-1944.
-
Hawkins CL, Brown BE, Davies MJ (2001) Hypochlorite- and hypobromite-mediated radical formation and its role in cell lysis. Archives of Biochemistry and Biophysics 395(2): 137-145.
-
Marcinkiewicz J, Biedron R, Bialecka A, Kasprowicz A, Mak M, et al. (2006) Susceptibility of Propionibacterium acnes and Staphylococcus epidermidis to killing by MPO-halide system products. Implication for taurine bromamine as a new candidate for topical therapy in treating acne vulgaris. Arch Immunol Ther Exp (Warsz) 54(1): 61-68.
-
Gottardi W, Klotz S, Nagl M (2014) Superior bactericidal activity of N‐bromine compounds compared to their N‐ chlorine analogues can be reversed under protein load. Journal of Applied Microbiology 116(6): 1427-1437.
-
Withers RMJ, Lees FP (1986) The assessment of major hazards: The lethal toxicity of bromine. J Hazard Mater 13(3): 279-299.
-
Pelgrift RY, Friedman AJ (2013) Topical hypochlorous acid (HOCl) as a potential treatment of pruritus. Current Dermatology Reports 2(3): 181-190.
-
Marcinkiewicz J, Pelc WA, Walczewska M, Godlewska LS, Jachowicz R, et al. (2008) Topical taurine bromamine, a new candidate in the treatment of moderate inflammatory acne vulgaris: a pilot study. Eur J Dermatol 18(4): 433-439.
-
Marcinkiewicz J (2010) Taurine bromamine (TauBr)-its role in immunity and new perspectives for clinical use. J Biomed Sci 17(1): S3.
-
Stroman DW, Mintun K, Epstein AB, Brimer CM, Patel CR, et al. (2017) Reduction in bacterial load using hypochlorous acid hygiene solution on ocular skin. Clinical Ophthalmology 11: 707-714.
-
McCulley JP, Dougherty JM, Deneau DG (1982) Classification of chronic blepharitis. Ophthalmology 89(10): 1173-1180.
-
Dougherty JM, McCulleyb JP, Silvany RE, Meyer DR (1991) The role of tetracycline in chronic blepharitis. Inhibition of lipase production in staphylococci. Investigative ophthalmology & visual science 32(11): 2970-2975.
-
Benkaouha B, Le Brun C, Pisella PJ, Chandenier J, Lanotte P (2015) Bacterial flora in blepharitis. Journal francais d’ophtalmologie 38(8): 723-728.
-
World Medical Association (2008) Ethical Principles for Medical Research Involving Human Subjects. Adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, and amended by the 59th WMA General Assembly, Seoul.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report