Contribution of Optical Coherence Tomography in the Diagnosis of Idiopathic Polypoidal Choroidal Vasculopathy in a Young Adult at Iota-Teaching Hospital
Introduction: Idiopathic polypoidal choroidal vasculopathy (IPCV) is a common cause of hemorrhage of the retinal pigmentary epithelium and neurosensory retinal detachment of oxidative origin. Its diagnosis is more easily made by Optical Coherence Tomography and Fluorescence Angiography or ICG. The aim of our work is to highlight the accuracy of OCT and AGF in the diagnosis of IPCV. We report a clinical case received in February 2019 in the vitreoretinal surgery and functional exploration of the visual apparatus department of the IOTA-Teaching Hospital. Case Report: A young man with a personal pathological history of arterial hypertension was referred to the department for macular OCT for central serous chorioretinitis. OCT and intravenous fluorescein angiography showed features of idiopathic polypoidal choroidal vasculopathy. The patient received anti-VEGF injections followed by significant visual improvement. Discussion: The pathogenesis of IPCV is not clearly elaborated, but it appears to be primarily due to an abnormality of choroidal vasculature. Conclusion: IPCV can occur in young subjects and leads to severe impairment of visual function. These severe visual impairments are resolved by the correct use of anti VEGF associated or not with the Argon laser
Introduction
Yannuzzi was the first ophthalmologist to describe Idiopathic Polypoidal Choroidal Vasculopathy (IPCV) in 1982 [1]. Idiopathic choroidal polypoidal vasculopathy is an abnormal, branched vascularization of the internal choroid associated with aneurysmal vascular dilations that may be responsible for detachment of the serous pigmentary epithelium and sometimes a true hemorrhagic picture [2]. While most often idiopathic, PCV may also be secondary to exudative AMD, myopic staphyloma, central serous chorioretinopathy/ diffuse retinal epitheliopathy or nevus. More recently, Freund has included PCV in the spectrum of pachychoroids [2].
The etiopathogeny of PCV is still unknown today [3]. PCV is clinically characterized by the presence of juxtapapillary and/or macular choroidal polypoidal excrescences. The visual prognosis is correlated with either the evolution of retinal lesions or the physical treatment of active polyps by argon or diode laser photocoagulation [4].
Optical coherence tomography allows us to obtain, in a noninvasive way, the characteristic signs of PCV such as the detachment of the dome-shaped pigmentary epithelium (DEP) and the sign of double- layer [5, 6].
Apart from treatment of polyps with argon or diode laser, there are other therapeutic alternatives such as focal laser, dynamic phototherapy (PDT), Anti-VEGF and combined treatment (PDT + anti-VEGF) [6, 7, 8].
Case Presentation
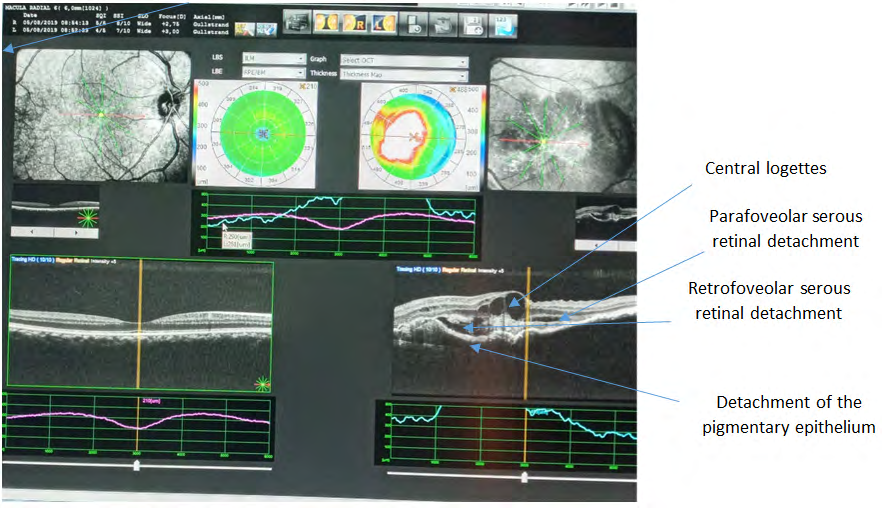
This is a 44-year-old man with a history of high blood pressure referred from a clinic in Bamako for macular OCT for central serous chorioretinitis. He had a sudden drop in visual acuity in his left eye. His best corrected visual acuity was 10/10 in the left eye and 10/10 in the contralateral eye. Examination of the fundus of the left eye revealed the presence of retinal hemorrhages, dry exudates, and multiple serous and hemorrhagic retinal detachments located along the temporal vascular arches. Optical coherence tomography revealed central fossae, multiple retinal serous detachments, serous detachment of the pigmentary epithelium, and a para- papillary vascular polyp in the left eye and a normal one in the right eye (Figure 1).
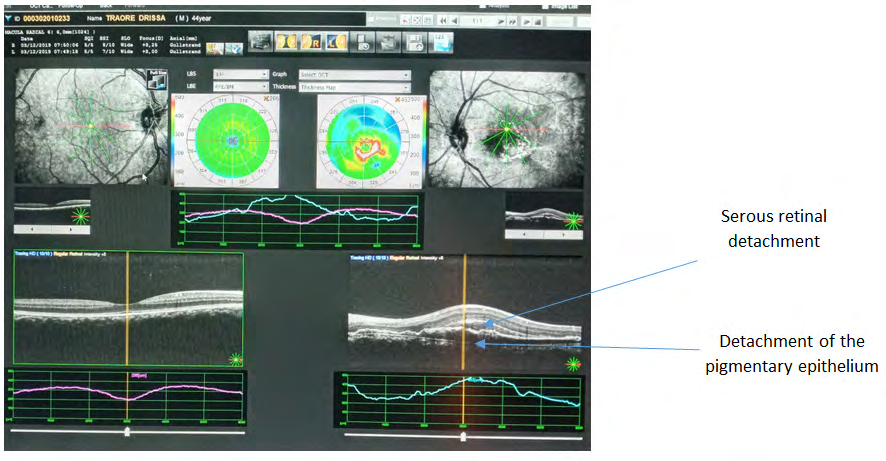
The diagnosis of idiopathic Choroidal polypoid vasculopathy was retained in front of this table. He then received 3 monthly injections of anti VEGF, followed by an improvement in visual acuity of the left eye with a 3/10 correction, disappearance of the stalls, regression of retinal serous detachment with persistence of a fine blade of retinal serous detachment and serous detachment of the retrofoveolar pigmentary epithelium and disappearance of the polyp (Figure 2).
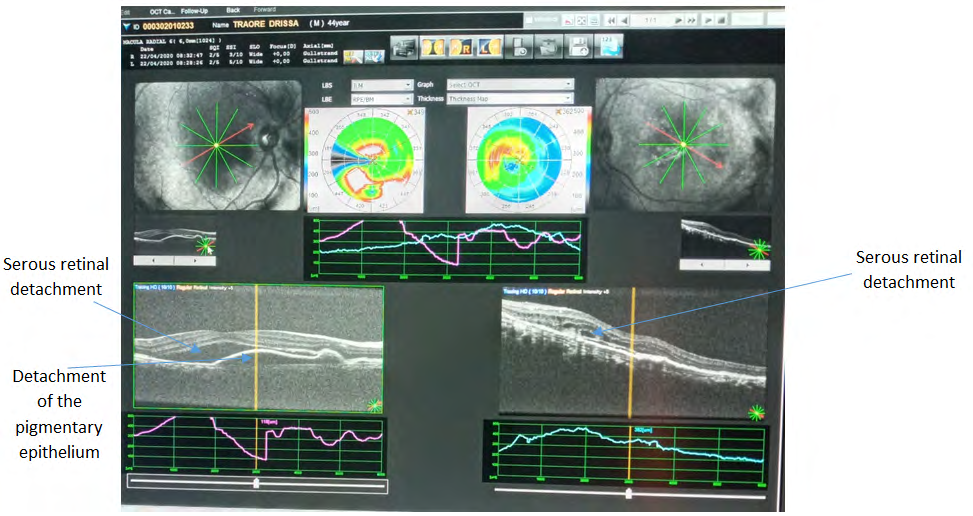
The patient was subsequently lost to follow-up. In April
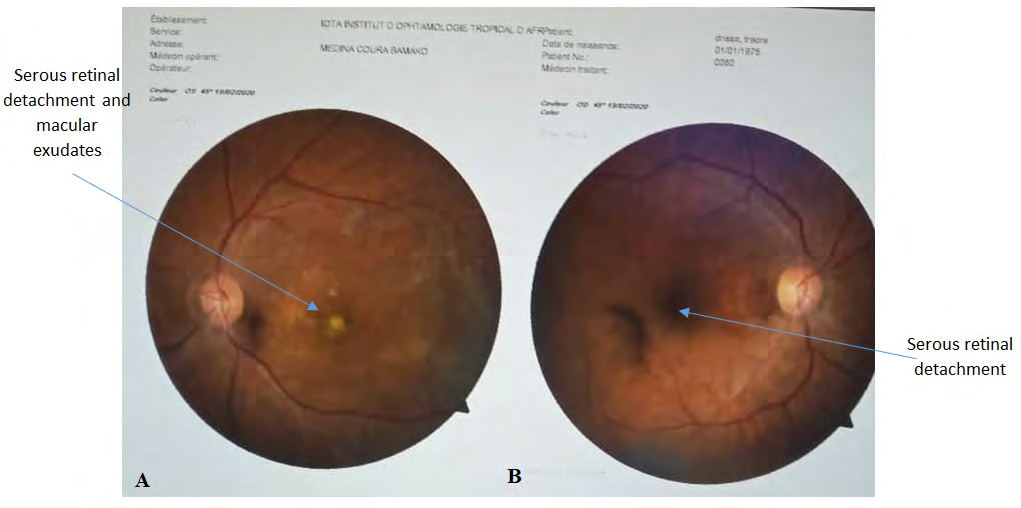
2020, we received him for decreased bilateral vision. His best corrected visual acuity was 3/10 in the right eye and 1/10 in the left eye. Examination of the fundus of the right eye revealed retinal hemorrhages and a central serous retinal detachment and a parapaillary hemorrhage and in the left eye central fibroatrophic scars e. Optical coherence tomography revealed in the left eye a central retinal serous detachment, a serous detachment of the pigmentary epithelium and a para-papillary vascular polyp. In the right eye, there were intraretinal fossae and a thin blade of retofoveolar retinal serous detachment (Figure 3).
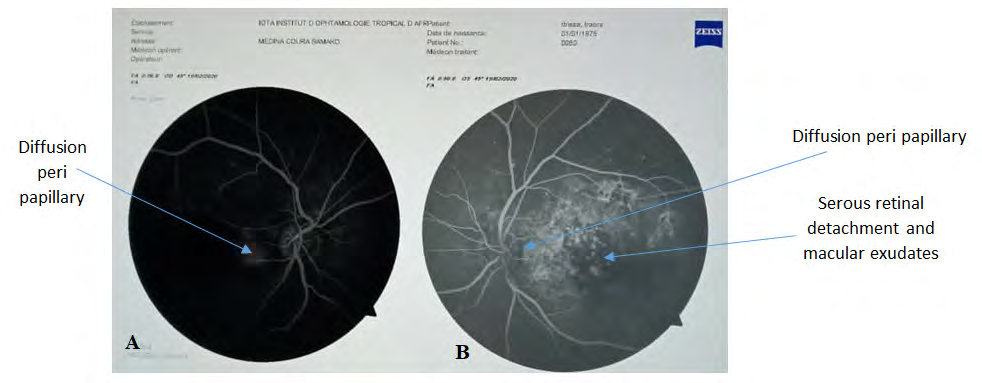
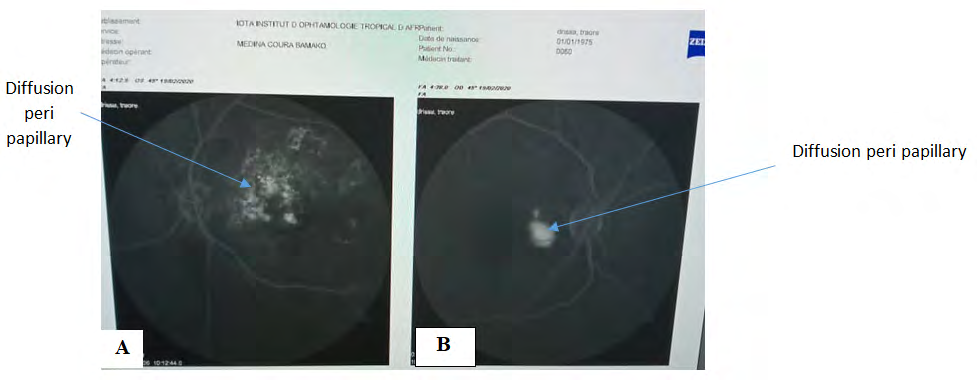
In the left eye, the AGF showed diffusion in the peri- papillary neo-vessels, macular exudates and localized mass effects in the macula. Then, in the right eye, only diffusion of the peri-papillary neo-vessels was noted (Figure 4).
In venous time, in the left eye there was an accentuation of the diffusion of the peri-papillary neo-vessels and macular exudates, and in the right eye only the accentuation of the diffusion of the peri-papillary neo-vessels was observed (Figure 5).
exudates, retinal serous detachment and macular scars in the left eye. Then the right eye showed mainly peri-papillary neo-vessels (Figure 6).
The persistence of these retinal lesions of the IPCV despite the series of 3 injections of Anti VEGF is in favour of the poor evolution of the IPCV in our patient.
Discussion
OPCV particularly affects black women between the ages of 50 and 65 with high blood pressure [9]. Its nosological framework has recently been redefined by Yannuzzi LA, et al. [10]. Vascular lesions correspond to dilated networks of choroidal vessels resulting in multiple aneurysmal lesions forming true “polyps” sometimes visible at the fundus as a red-orange subretinal mass. These polyps are usually located in the peripapillary region. However, a macular variant of IPCV has recently been described [10]. It is interesting to note in our patient’s case that the macular involvement was initially in the second eye and in the first eye we saw the macular lesions at an advanced stage.
Age-related macular degeneration (AMD) is the main differential diagnosis of IPCV in Caucasian subjects, but also central serous chorioretinitis [8, 9]. Although the abnormalities of the funds are sometimes identical, unlike AMD, there is generally no drusen or PE revisions in patients with AMD [10]. In addition, IPCV appears to have a better visual prognosis and a more stable long-term course than AMD [11]. Yannuzzi considers that the majority of patients with VCPI maintain a visual acuity of 2-3/10 or greater [10]. OCT SD allows the diagnosis of VCPI to be strongly suspected, by showing the characteristic signs which are: polyps, in the form of elevations of the domed pigmentary epithelium, and the double layer sign which is an irregular planar elevation of the pigmentary epithelium associated with a thickened choroid [12]. FFA, on the other hand, is not very specific of VCPI and shows a hyperfluorescence crescendo with a late hypofluorescence and leakage pattern or serous pigmentary epithelium detachment [12]. However, in China, the authors have shown that the combination of OCT and FFA increases the sensitivity of the diagnosis of VCPI from 60% to 90% [13]. The common sign of VCPI in OCT SD and FFA is the pigmentary epithelium detachment. In our patient the combination of OCT and FFA allowed us to diagnose VCPI in front of the following signs: Serous pigmentary epithelium detachment, serous retinal detachment, leakage pattern. However, the prognosis of the disease is heavily influenced by the presence of occult choroidal neo-vessels [11]. This may be the reason for the extremely unfavorable course of our patient’s IPCV. Nevertheless, rapidly developing exudative and hemorrhagic lesions are usually accompanied by a significant but transient loss of vision due to subretinal hemorrhages and PE detachments that resolve over time. In contrast, the severe loss of vision in the left eye observed in our patient as a result of chorioretinal scarring and areas of extensive retinal fibrosis is a more unusual course of the disease, although we cannot definitively rule out an association between IPCV and subretinal neo-vessels. In addition, the pejorative evolution of the right eye could be due to delayed diagnosis and irregular follow-up. In fact, the optimal treatment of IPCV is currently not clearly codified. There is no medical treatment. Data from the literature show that corticosteroids provide little or no benefit in the treatment of IPCV.
Concerning the therapeutic management of polyps, there are therapeutic alternatives: focal laser, dynamic phototherapy (PDT), anti-VEGF and combined treatment (PDT + anti-VEGF). We have achieved functional and anatomical improvement with intravitreal injections of anti- VEGF.
Conclusion
Although ICGA remains the current gold standard for the diagnosis of VCPI, the combination of FFA and OCT nevertheless has a high sensitivity for the diagnosis of VCPI. This is a godsend for us ophthalmologists working in the tropics with limited resources.
Conflict of Interest: None
Source of Funding: IOTA-Teaching Hospital research fund.
References
-
Yannuzzi LA, Sorenson J, Spaide RF, Lipson B (1990) Idiopathic polypoidal choroidal vasculopathy (IPCV). Retina 10:1-8.
-
Burelle X, Dot C, Henckes O, Wary P, Meurie D, et al. (2007) Idiopathic choroidal polypoidal vasculopathy and treatment difficulties: a case report. J Fr Ophtalmol 30: 25273.
-
Leblanc A, Sztermer E, Boixel R, Rumen F, Gobert F (2016) Hemorragie sous-epitheliale massive chez un sujet jeune: a propos d’un cas de vasculopathie polypoidale choroïdienne idiopathique. Images en Ophtalmologie X (3): 108-111.
-
Guyomarch J, Charles JA, Acis D, Donnio A, Richer R, et al. (2008) Vasculopathie polypoïdale choroïdienne idiopathique : aspects cliniques et angiographiques. J Fr Ophtalmol 31(6): 579-584.
-
Sato T, Kishi S, Watanabe G, Matsumoto H, Mukai R (2007) Tomographic features of branching vascular networks in polypoidal choroidal vasculopathy. Retina 27(5): 589-594.
-
Srour M, Querques G, Semoun O, Ameen AE, Miere A, et al. (2016) Optical coherence tomography angiography characteristics of polypoidal choroidal vasculopathy. Br J Ophthalmol 100(11): 1489-1493.
-
Rouvas AA., Papakostas TD, Ntouraki A, Douvali M, Vergados I, et al. (2011) Photodynamic therapy, ranibizumab and ranibizumab with photodynamic therapy for the treatmet of polypoidal choroidal vasculopathy. Retina 31(3): 464-474.
-
Won CW, Cheung CM, Mathur R, Li X, Chan CM, et al. (2015) Three-year results of polypoidal choroidal vasculopathy treated with photodynamic therapy: Retrospective study and systematic review. Retina 35(8): 1577-1593.
-
Perkovich BT, Zakov ZN, Berlin LA, Weidenthal D, Avins LR (1990) An update on multiple recurrent serosanguineous retinal pigment epithelial detachments in black women. Retina 10(1): 18-26.
-
Yannuzzi LA, Ciardella A, Spaide RF, Rabb M, Freund KB, et al. (1997) The expanding clinical spectrum of idiopathic polypoidal choroidal vasculopathy. Arch Ophthalmol 115(4): 478-485.
-
Coscas G, Lupidi M, Coscas F, Benjelloun F, Zerbib J, et al. (2015) Toward a specific classification of polypoidal choroidal vasculopathy:idiopathic disease or subtype of age-related macular degeneration. Invest Ophthalmol Vis Sci 56(5): 3187-3195.
-
Mayer Srour, Oudy Semoun, Eric Souied (2017) Vasculopathie polypoïdale: diagnostic et traitement 2017. Pratiques en Ophtalmologie 10(98): 109-114.
-
Huang YM, Hsieh MH, Li AF, Chen SJ (2017) Sensitivity, Specificity, and Limitations of Optical Coherence Tomography Angiography in Diagnosis of Polypoidal Choroidal Vasculopathy. Journal of Ophtalmology pp: 1-8.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report