Overview of Orbital Inflammation/Unmet Needs
Diseases of the orbit and periorbital eye tissues manifest in a wide variety of clinical presentations. Space occupying lesions in the orbit include infections, inflammations, vascular malformations, and malignancies. The significant variation in presentations is due to the complex anatomy of the orbit and the heterogeneous nature of the multiple disease processes that present themselves as orbital inflammatory processes. Additionally, although specific disease entities often show similar patterns of orbital tissue involvement, there is still a spectrum of clinical presentations within disease processes, which furthermore overlap with other inflammatory etiologies. This heterogeneity creates a significant challenge in determining specific diagnoses and subsequently instituting timely medical and surgical management of patients with orbital inflammation. Despite advances in imaging, physical examination, and laboratory tests, a biopsy is often needed for diagnosis and to guide treatment. Unfortunately, the biopsy is too often read as non-specific or idiopathic inflammation, a term that gives minimal guidance to the patient or to the clinician. There is clearly a need for developing more specific and sensitive clinical diagnostic testing.
Introduction
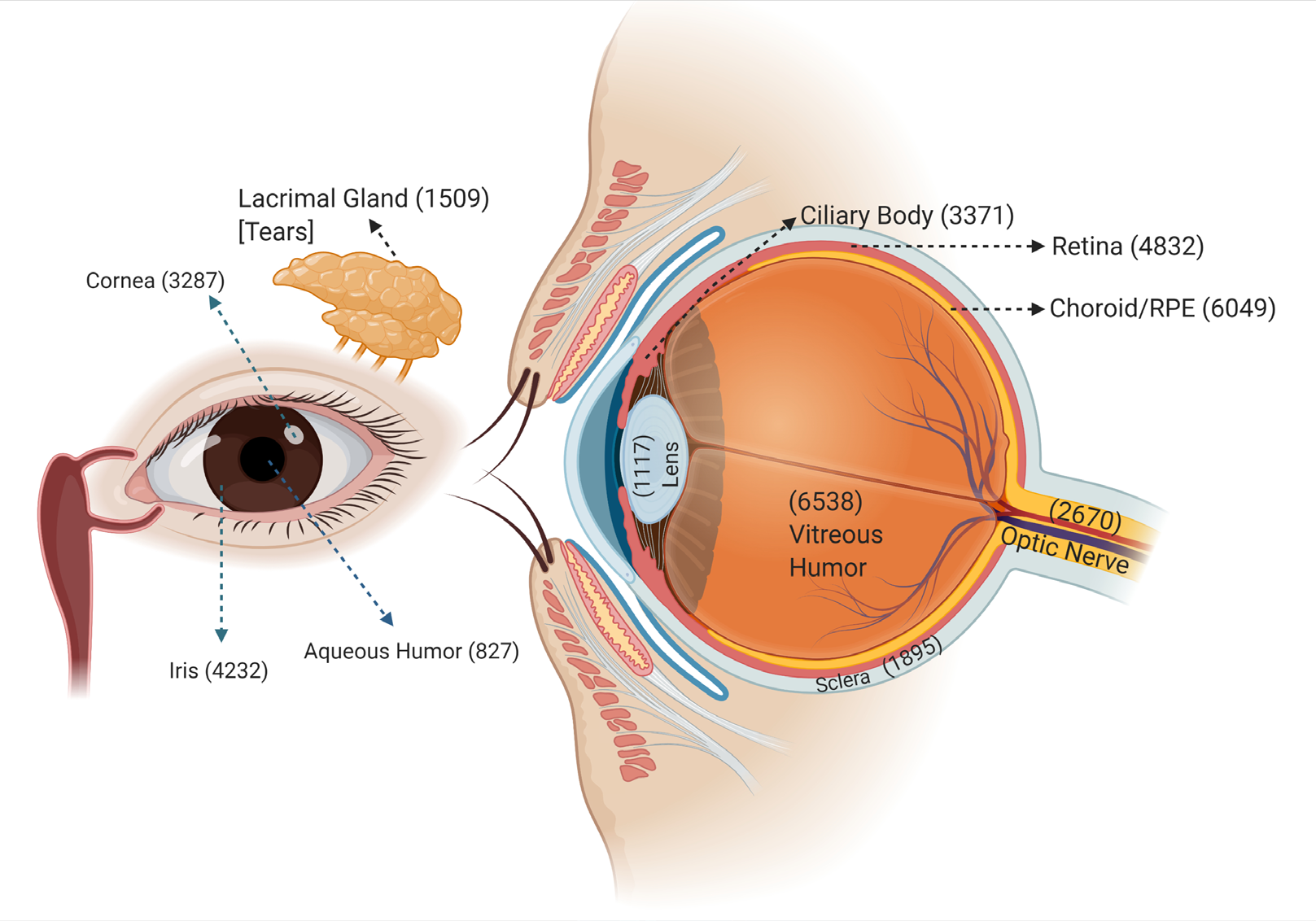
The anatomy of the orbit is complex. Within the 30- cc volume of the bony orbit is housed the eye itself, the six extraocular muscles that provide ocular motility, the eyelid retractor and protractor muscles, orbital fat, supporting fascial and septae, cranial nerves, vascular structures, and the lacrimal gland. Each of these structures may independently or in multiple and varied combinations, be involved in inflammation in the orbit. Further complicating the matter, structures adjacent to the orbit such as the paranasal sinuses, intracranial cavity with dura and brain, and the cavernous sinus may be sequentially or simultaneously involved with inflammatory processes. When specific anatomic structures are inflamed, they result in clinically and radiologically localizable findings. If the extraocular muscles are involved, pain and restriction with ocular movement as well as proptosis may be present.
Diffuse orbital inflammation involving the orbital fat and connective tissue will cause pain, edema, and proptosis. If the connective tissue at the posterior globe surface is involved, posterior scleritis develops. Inflammation in the posterior orbit can result in orbital apex or cavernous sinus syndrome resulting in multiple cranial neuropathies and potentially vision loss. When the lacrimal gland is inflamed, it may enlarge; causing mechanical ptosis or proptosis, and its physiological function is often altered due to infiltration of the glandular tissue. The most common symptoms include a painful mass and dry eye due to likely alteration in tear volume and composition. Granulomatous inflammation can present as an orbital soft tissue mass simulating a neoplasm. Neoplastic disease can also cause secondary inflammation of the orbit. As mentioned earlier, anatomic structures can either be involved in isolation or combination providing a wide variety of clinical presentations.
Inflammation of the orbit is not a specific diagnosis but a physiological end response to multiple disease processes. Several systemic, immune-mediated diseases can involve the orbit [1]. Entities that cause orbital inflammation include infections that may be bacterial, viral or fungal in etiology, systemic autoimmune diseases such as Graves’ disease (thyroid eye disease, TED) [2], sarcoidosis [3], systemic lupus, IgG4 disease [4], granulomatosis with polyangiitis (GPA) [5], neoplastic diseases, and as a diagnosis of exclusion, non-specific orbital inflammation (NSOI; idiopathic orbital inflammation, orbital pseudotumor) [5, 6].
Each of these disease processes can present in varying severities. When there is impending vision loss from optic nerve compression, vascular compromise with the risk of infarction from vasculitis or orbital apex or cavernous sinus involvement, or significant disability due to pain, intractable diplopia or ocular surface damage from exposure, there is a great impetus to quickly and accurately diagnose and treat these diseases.
The differential diagnosis of orbital inflammation can be narrowed using epidemiologic data on age distribution and the probability of diseases. For example, the most common causes of orbital inflammation are infection and thyroid eye disease. According to a recent review, the thyroid gland is the most common organ affected by autoimmunity [7]. Graves’ disease affects about 1% of the US population, half of whom have ophthalmopathy [8], although the eye disease is markedly symptomatic in only about 10% of those affected [9].
There are various forms of diseases that involve the orbit and therefore the discussion of those disorders are often organized in line with the etiology (e.g., infection, inflammation, neoplasm) or by anatomic location.
Findings on examination that warrant imaging studies include pain on eye movement, afferent pupillary defect, limited extraocular motions, resistance on retropulsion, and arterialization of conjunctival blood vessels. Image findings in pre-septal cellulitis include the following:
- Swelling of the eyelid and adjacent pre-septal soft tissues
- Obliteration of the fat planes or details of the pre-septal soft tissues
- Absence of orbital inflammation The term cellulitis in general parlance refers to non- suppurative invasive infection (most commonly bacterial) of subcutaneous tissue. Spreading infection, poor localization in addition to cardinal signs of inflammation are the hallmark of cellulitis. Cellulitis can be complicated by spread of infection to the underlying deeper structures with progressive tissue destruction & ulceration with release of bacterial toxins. Orbital cellulitis is an infection of the fat and ocular muscles of the orbit posterior to the orbital septum. It is classically distinguished clinically from pre-septal cellulitis by the presence of pain with eye movement and proptosis on physical examination.
As the cellulitis spreads with involvement of deeper orbital structures, there is proptosis, conjunctival chemosis, limitation of ocular motility, drop in visual acuity, with progressive optical nerve dysfunction, reduced corneal & periocular sensation. Chandler's classification describes staging of orbital cellulitis from stage 1- preseptal cellulitis. stage 2- orbital cellulitis, stage 3- Orbital subperiosteal abscess/intraorbital abscess, stage 4- Cavernous sinus thrombosis and a relatively chronic course. stage 5- subdural empyema and guides the management of orbital cellulitis till date. Lacrimal gland pyoadenitis/pyomyositis of the extraocular muscles are also pyogenic complications of orbital cellulitis and relatively rarer clinical presentations (not included in Chandler's classification) The other interesting fact to consider that probably contrasts generalized and orbital cellulitis are the systemic complications secondary to hematogenous spread, occurrence of systemic inflammatory response syndrome seen commonly in generalized cellulitis while intracranial complications due to local contiguous spread rather than hematogenous spread is the pattern seen repeatedly in the orbital region. The possible reason to consider here are the uniqueness of vascular supply in the orbital region. The eyelids are supplied by the external carotid system with good collateral circulation while the orbital and adnexal tissues are supplied by the internal carotid system characterized by specific end organ vessel branches. This probably reduces the chances of direct systemic spread from the orbital region and at the same time increases the risk of intracranial complications if managed inadequately.
Discussion
A multiple-case series compilation of orbital disorders by Wilson and Grossniklaus, and later by Shields et al were based on a review of biopsy specimens, whereas Henderson
et al, Kennedy et al, Rootman, and Shields studies were based on clinical practice. “A retrospective review of 6328 consecutive patients with orbital disease in south India” included all comprehensive descriptions and reviews of orbital disorders (Table 1). The main outcome measured was the incidence of orbital diseases as determined by clinical and pathological criteria. In this study of 6328 patients, 34.1% had inflammatory orbital disease with 2161 patients including 1473 idiopathic orbital inflammation, 270 infection, 126 dacryoadenitis, and 292 other etiologies. Among the 1965(31%) patients presenting with systemic diseases involving the orbit, 1938 were diagnosed with thyroid orbitopathy [10].
| Shields | Kennedy | Henderson | Rootman | Wilson | Aravind |
|---|---|---|---|---|---|
| Systemic | 54 (6.6) | 52 (3.8) | 682 (49) | 10 (3.2) | 1965 (31.0) |
| Inflammatory | 132 (20.5) | 142 (17.3) | 129 (9.2) | 45 (14.5) | 2161 (34.1) |
| Trauma | 107 (3.0) | 76 (5.4) | 13 (4.1) | 308 (4.8) | |
| Congenital | 194 (30.1) | 69 (8.4) | 101(7.1) | 23 (7.3) | 600 (9.4) |
| Vascular | 4 (06) | 26 (2.2) | 40 (2.8) | 7 (2.2) | 17 (0.2) |
| Primary neoplasia | 229(35.5) | 345(42) | 109(34,9) | 109(34,9) | 1155(18.2) |
| Secondary neoplasia | 70(11.1) | 51 (6.2) | 44(3.1) | 90 (28.7) | 82 (1.3) |
| Metastases | 16 (2.5) | 27 (3.3) | 38 (2.7) | 15 (4.8) | 39 (0.6) |
| Total | 645 | 821 | 1409 | 312 | 6328 |
Table 1: Summary of orbital lesions. Kim UR, Khazaei H, Stewart WB, Shah AD. Spectrum of orbital disease in South India: an Aravi
Imaging studies are commonly used to determine the specific location of the disease within the orbit, anatomic structures involved, degree of inflammation, the shape of infiltrated tissues, and involvement of sinuses, nasal passages, and intracranial structures. Radiographic examination of the orbit usually involves computerized tomography scan (CT), and magnetic resonance imaging (MRI) with intravenous contrast and is incredibly useful in narrowing the differential diagnoses and assessing the location and extent of the disease process [11]. Orbital ultrasound also has a wide range of clinical indications. For example, following examination of a patient with ocular discomfort or pain, clinicians can use ultrasonography to help confirm a diagnosis of scleritis, orbital myositis, or dacryoadenitis. Clinicians can use ultrasonography to evaluate retrobulbar tissue, including the extraocular muscles, in a patient with exophthalmos and suspected soft tissue expansion secondary to Graves’ disease [12].
Although imaging can help narrow the range of diagnoses to consider, images are only useful in that they reveal patterns and locations of tissue involvement which may statistically be more common in certain disease entities. Imaging is often not specific enough to verify exact disease entities or obviate a biopsy.
Additional investigations involve the use of blood testing. Blood tests should be guided by clinical suspicion and available tests include complete blood counts, erythrocyte sedimentation rate (ESR), serum protein electrophoresis, C-reactive protein, antinuclear antibody (ANA), angiotensin- converting enzyme (ACE), antineutrophil cytoplasmic antibodies either peri-nuclear (pANCA) or cytoplasmic (cANCA), and thyroid function studies. Although very helpful when positive, false negatives still contribute to the dilemma of a specific diagnosis. Some of the listed tests are also non- specific and only confirm the presence of an inflammatory process and there may be overlap among disease entities.
In the clinical management of these patients with orbital inflammation, it is common for empiric treatment or treatment with only limited data for guidance. The most frequent practice is to treat with antibiotics if there is suspicion of bacterial infection supported by fever, elevated WBC, and if fortunate, positive bacterial culture from swabbing of discharge. If there is no response to antibiotics or the suspicion for infection to be the causative factor of the inflammation is low, a trial of systemic corticosteroids, or non-steroidal anti-inflammatories, may be instituted, and the patient followed for clinical response. If there is complete response and no recurrence with a taper, then the patient may simply be observed for any recurrence. However, the response is often incomplete or there is a relapse of the inflammation. This may imply a more resilient form of an inflammatory process or more ominously, a secondary finding of occult malignancy. In such cases of poor response, relapse, or recurrence, the default next step in care due to diagnostic uncertainty is tissue biopsy.
Biopsy of involved orbital tissue is usually an open surgical procedure. Fine needle aspiration for cytology is highly dependent upon the skill of the reading cytologist and a lesion location amenable to safe biopsy, thus having a limited role in orbital diagnostics. An open surgical biopsy may be straight forward such as when obtaining a biopsy from the orbital lobe of the lacrimal gland or anterior orbital fat. These areas are relatively low risk for biopsy. However, if the affected tissue involves the optic nerve sheath, the orbital apex, or cavernous sinus, a biopsy could result in greater morbidity than the disease process itself. Even with obtaining adequate tissue for study, there are cases that may still be read as non-specific chronic or acute inflammation. Classic H&E histopathology is not specific enough to determine all the different entities causing orbital inflammation. Therefore, histopathology is not a reliable method to discriminate among the many orbital inflammatory diseases. However, knowledge of and determination of the genes expressed within a tissue specimen can augment and narrow down the diagnoses [13]. We have previously reported that NSOI is a heterogeneous collection of diseases based on gene expression profiling [14]. Despite an improved ability to study cell markers and gene expression within tissue specimens, diagnosis of cases of NSOI is still a clinical challenge due to the range of presentation within NSOI and the variable responses to different treatments. This may suggest that the category of diseases deemed to be NSOI actually is still comprised of a varied number of specific diseases not yet identified. Given the need for additional diagnostic studies with greater specificity and sensitivity along with the goal of decreasing morbidity of open surgical biopsy, the evaluation of the tear proteome may be a fruitful area of investigation. As stated earlier, inflammation within the orbit can directly involve the lacrimal gland. This would very likely change the composition of the tear secretions. Even when not directly involved, inflammatory processes within the orbit can potentially affect the adjacent lacrimal gland through the contiguous inflammatory spread and local release of inflammatory cytokines. This could also affect the tear composition and possibly in a manner that is distinct from inflammation directly occurring in the lacrimal gland. Thus, studying the proteomic profile of the lacrimal secretions in normal patients and across the spectrum of patients with varied inflammatory diseases may enable the creation of tear proteomic profiles specific to each disease. Such data could be used to better diagnose patients with orbital inflammation and potentially decrease the need for a surgical biopsy.
Conclusions and Future Needs
Idiopathic orbital inflammation may be a multifarious illness with a wide spectrum of clinical, radiological, and histopathological presentations. By accurately diagnosing and managing them in a timely manner we can avoid permanent vision loss and even save a patient’s life. Additionally, in-depth knowledge of pathological processes holds the promise of improved therapies supporting this molecular understanding, which has both practical and theoretical implications.
The adherence to a strict criterion is important to boost the understanding of the pathophysiology of eye disease and to lead the initiation of new preventive and therapeutic modalities. One key factor is whether those tear biomarkers are specific to certain diseases. Most proteins in tears originate from the lacrimal gland, but they may also be released from epithelial cells that are shed or leaked from blood vessels during inflammation, injury, or irritation.
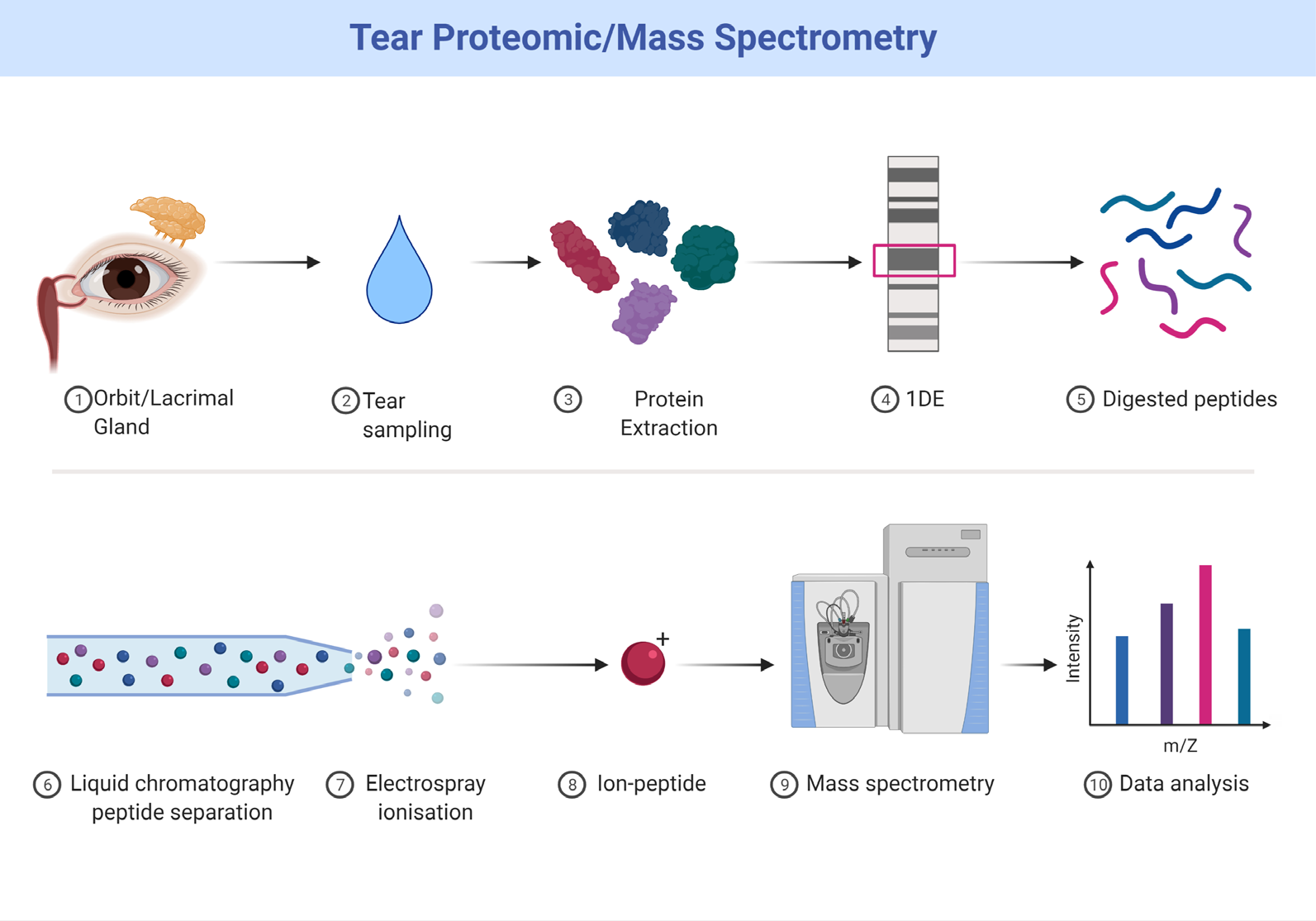
Clinically useful biomarkers in orbital inflammatory diseases (OID) are rare. An ideal molecular biomarker would be minimally invasively obtained allowing for repeat testing, specific to the disease with high sensitivity, with quantitative measurements, and inexpensive. Potential biofluids to test include blood, urine, or tears. Geographically, tears are the closest to the location of disease in OID with theoretically the highest concentration of potential biomarkers. They are also the most readily accessible body fluid and much less complex than blood or urine. With technological advancements, the ability to identify subtle differences increases the chance to find such a biomarker.
Tear proteomics in OID allows us to monitor patients longitudinally, clarify disease pathogenesis, develop new therapeutic targets, predict response and optimal timing of therapy, as well as determine which patients will go on to develop sight threatening disease. Thyroid eye disease (TED) is the most prevalent OID leading itself to research. To our knowledge, there are no tear studies in other OID [15]. Studying OID together will allow for selection of unique disease specific biomarkers and determine possible existence of shared pathogenesis, which may lead to therapeutic expansion.
Declaration of Helsinki
This review is adhered to the ethical principles outlined in the Declaration of Helsinki as amended in 2013. (https:// www.wma.net/what-we-do/medical-ethics/declaration-of- helsinki/).
Funding: None
Conflict of Interest: None
Authors’ Contribution Acknowledgement
HK drafted the manuscript. All the authors edited the manuscript jointly and approved the final manuscript. The authors thank Dr. Kaneez Abbas for critical feedback and helping to develop the search strategy and proof reading. Figure 1 &2 were designed and created in BioRender.com
References
-
Sharma SM, Choi D, Planck SR, Harrington CA, Austin CR, et al. (2009) Insights in to the pathogenesis of axial spondyloarthropathy based on gene expression profiles. Arthritis Res Ther 11(6): R168.
-
Bahn RS (2010) Graves’ Ophthalmopathy. New Engl J Med 362(8): 726-738.
-
Rosenbaum JT, Choi D, Wilson DJ, Grossniklaus HE, Harrington CA, et al. (2015) Parallel Gene Expression Changes in Sarcoidosis Involving the Lacrimal Gland, Orbital Tissue, or Blood. JAMA Ophthalmol 133(7): 770- 777.
-
Wong AJ, Planck SR, Choi D, Harrington CA, Troxell ML, Houghton DC, et al. (2014) IgG4 immunostaining and its implications in orbital inflammatory disease. PLoS One 9(10): e109847.
-
Rosenbaum JT, Choi D, Wilson DJ, Grossniklaus HE, Harrington CA, et al. (2015) Orbital pseudotumor can be a localized form of granulomatosis with polyangiitis as revealed by gene expression profiling. Exp Mol Pathol 99(2): 271-278.
-
Rosenbaum JT, Sibley CH, Choi D, Harrington CA, Planck SR (2015) Molecular Diagnosis: Implications for Ophthalmology. Progress in retinal and eye research 50: 25-33.
-
McAleer JP, Nguyen NL, Chen K, Kumar P, Ricks DM, et al. (2016) Pulmonary Th17 Antifungal Immunity Is Regulated by the Gut. Microbiome J Immunol 197(1): 97-107.
-
Sharma S, Wheelan S, Marchionni L, Harrington CA, Choi D, et al. (2015) Identification of a gene expression profile specific to non-infectious uveitis using high throughput microarray data and a novel pipeline of in-silico methods. Invest Opthalmol Vis Sci Invest 56(7): 1719.
-
van Elburg RM, Uil JJ, Mulder CJ, Heymans HS (1993) Intestinal permeability in patients with coeliac disease and relatives of patients with coeliac disease. Gut 34(3): 354-357.
-
Khazaei H, Seethapathy G (2022) Spectrum of orbital inflammatory disorders. International Journal of Medical and All Body Health Research, pp: 35–38.
-
Yuen SJA (2003) Idiopathic Orbital Inflammation. ArchOphthalmol 121(4): 491.
-
Khazaei H, Khazaei D, Ashraf D, Mikkilineni S, Ng JD (2022) Overview of Orbital Ultrasonography. Ann Ophthalmol Vis Sci 5(1): 1028
-
Jakobiec FA, Font RL (1986) Non-infectious orbital inflammation. In: Spencer WH, (Ed), Ophthalmic Pathology: An Atlas and Textbook. 3, Philadelphia: W.B. Saunders, pp: 2777.
-
Rosenbaum JT, Choi D, Harrington CA, Wilson DJ, Grossniklaus HE, et al. (2017) Gene Expression Profiling and Heterogeneity of Nonspecific Orbital Inflammation Affecting the Lacrimal Gland. JAMA Ophthalmol 135(11): 1156-1162.
-
Khazaei H, Khazaei D, Verma R, Ng J, Phillip A, et al. (2021) The potential of tear proteomics for diagnosis and management of orbital inflammatory disorders including Graves’ ophthalmopathy, Experimental Eye Research 213: 108813.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report