Modified Samuel Masket’s Technique
Despite recent advances in techniques and technology, phacoemulsification in a rock hard nucleus is challenging, even for an experienced surgeon. Incidence of capsularzonular complications, corneal edema wound burn and post-operative inflammation is high. However, the operating surgeon can achieve gratifying results if a proper and effective surgical strategy is adopted. Samuel Masket’s technique is one such technique which makes a surgeon’s life easier with managing hard cataract. In this video, we present our modification of Samuel Masket’s technique [1].
Introduction
Despite recent advances in techniques and technology, phacoemulsification in a rock hard nucleus is challenging, even for an experienced surgeon. Incidence of capsular- zonular complications, corneal edema wound burn and post-operative inflammation is high. However, the operating Clinical Note surgeon can achieve gratifying results if a proper and effective surgical strategy is adopted. Samuel Masket’s technique is one such technique which makes a surgeon’s life easier with managing hard cataract. In this video, we present our modification of Samuel Masket’s technique [1].
Material and Methods
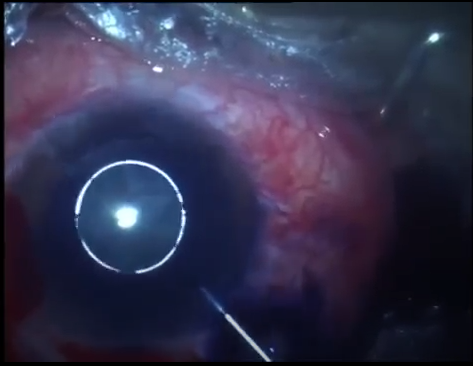
After a careful capsulorrhexis, gentle hydro dissection is done to detach the hard nucleus from its surrounding attachment and avoiding pressure on already weak zonules while doing so. A small, eccentric, vertical trench is made by placing the probe in the center and beginning the trench from the center like drawing a radius in a circle. This radius is eccentric as we want to divide the nucleus into one smaller half and one bigger half. Now without cracking this nucleus is then rotated 180 deg and in the “chop” mode, using the starting point of the trench as “chop-wall”, an attempt to cop the smaller half is made. Because of the trench behind this smaller half ea silly cracks and is then emulsified without putting too much pressure on the zonules. Once the smaller half is emulsified, there is lot more space in the bag for the bigger half to move without breaking the zonules or the posterior capsules. The bigger half can then be emulsified using a “direct-chop” or a “stop and chop” technique.
Discussion
Managing a hard cataract really “cracks” the brain of any phaco surgeon. Any inadvertent complication can lead to worse consequences in an otherwise good outcome surgery. Advantages of using an eccentric trench in Samuel Masket’s technique ensure a positive outcome even in beginner hands which are not well-versed with “direct-chop” technique. Because the smaller half is emulsified first, the rest of the nucleus can be emulsified fast too using less energy and without creating too much pressure on the posterior capsule.
Conclusion
Avoidable complications, when avoided can lead to a better patient outcome in and otherwise challenging cases. Our modification of Samuel Masket’s technique of creating an eccentric trench unlike the original ensures fewer incidences of corneal and capsular zonular complications.
References
-
Dudani AI, Dudani AA, Dudani K, Dudani AA (2022) Half stop and chop, petal by petal deflowering of hard cataracts. Indian J Ophthalmol 70(8): 3157.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report