Safety and Performance of an Artificial Tear Containing Arabinogalactan, Trehalose and Hyaluronic Acid in the Treatment of Dry Eye in Subjects with Signs of Inflammation of the Ocular Surface
Background: In this study it has been evaluated the safety and the clinical performance of a new combination of topical solution based on arabinogalactan, trehalose and hyaluronic acid, in reducing symptoms and signs of inflammation in a selected population affected by dry eye disease. Methods: The study enrolled 25 patients (ranging from 57 to 71 years) with signs and symptoms of dry eye disease. They received a combination therapy with arabinogalactan, trehalose and hyaluronic acid one drop three times a day for the first week and subsequently according to their symptoms. Ocular surface disease index score, tolerability and adherence were used to evaluate subjective symptoms of dry eye disease at enrolment (T0), week 1 (T1) and week 4 (T2). Clinical signs were assessed at T0 and T2. The assessment plan included: slit-lamp examination of the anterior segment, uncorrected and corrected visual acuity, ocular protection index, tear film break up time, osmolarity, meniscometry, evaluation of conjunctival hyperemia according to Efron’s classification, the presence of MMP-9, conjunctival and corneal staining and intraocular pressure. Results: The study group showed significant improvement in several clinical parameters after treatment. Ocular surface disease index score was significantly lower at the end of the follow up period, also evaluation of tolerability (ocular burning, ocular itching and blurred vision), before and after instillation, showed a statistically significant improvement at T0 and T1. Improvements in tear film break up time, meniscometry results and conjunctival and corneal hyperemia were statistically significant in the study group (p <0.05). A statistically significant, decrease in MMP-9 levels was also observed. Conclusions: Preliminary findings suggest that the new combination of topical solution based on arabinogalactan, trehalose and hyaluronic acid, could be effective in reducing early inflammatory markers, symptoms and signs, associated with the progression of dry eye disease.
Introduction
Dry Eye Disease (DED) represents a heterogeneous group of conditions with functional tear deficiency, secondary to reduced tear production or excessive tear evaporation associated with ocular discomfort. This can have an impact on everyday activities [1]. Tear film plays an important role in maintaining high optical quality of the ocular surface by exerting trophic support to the epithelial cells in the cornea and conjunctiva, thus providing the anterior part of the eye a refractive and antimicrobial function. In 2017 the Tear Film and Ocular Surface Society (TFOS) published the Dry Eye Workshop (DEWS) II Diagnostic Methodology report, which identified the most appropriate steps and technique to perform diagnostic tests and monitor dry DED; it also provided guidelines for differential diagnosis [2]. This report highlighted a strategy for identifying DED in the adult population. DED tends to increase with age and higher rates have been reported in women than in men [3].
In the pathophysiology of chronic DED, a vicious circle of inflammation involving both innate and adaptive immune responses is now well recognized at the initial stage [4]. These findings identified metalloproteinase-9 (MMP9) and the lipopolysaccharide-induced secretion of leukotriene B4, as well as other proinflammatory cytokines/chemokine’s, among the others, as inflammatory mediators; an increased expression and activation of enzymes that lead to cellular and tissue damage was also shown [3]. Such mediators, together with tear hyperosmolarity, have been shown to cause the loss of goblet cells and damage to the epithelial glycocalyx; inflammatory mediators produced by activated T-cells, recruited to the ocular surface, enhance damage [3]. This cascade of events promotes punctate epitheliopathy in DED and tear film instability and breakup that exacerbates and amplifies tear hyper-osmolarity with the completion of the vicious circle that causes the perpetuation of the ocular surface damage [3].
Arabinogalactan (AG) is a polysaccharide abundant in most plants, but it is usually derived from the bark of the Larch trees (Larix occidentalis, Larix decidua) of Larix species. It is formed of arabinose and galactose in a ratio of 1:6, with a small amount of glucuronic acid [5]. Furthermore, despite AG has great morphological freedom, it generally has a rigid triple spiral helix structure while the lateral groups form flexible branches with many exposed hydroxyl groups; this is the reason underlying the mucoadhesive characteristics of the polymer and plays an important role in DED treatment [6]. Indeed, AG can interact with mucins, which have a key role in tear film stability and quality [4]. Trehalose is a disaccharide, which protects cells against multiple environmental stress factors, such as drying, dehydration, cold, heat and oxidation. Among these functions, protection against drying and dehydration has been widely studied in ophthalmic research in the treatment of dry eye disease [7, 8].
Hyaluronic acid (HA) (also called hyaluronan) is a glycosaminoglycan formed by repetitive units of D-glucuronic acid and N-acetyl-D-glucosamine; it is an anionic, non- sulfated polymer and it is one of the most abundant components of the human connective tissue. HA has been extensively studied and used in artificial tear formulations because of its efficacy in dry eyes syndrome. This is due to its ability to increase wettability of the corneal epithelium and stability of the pre-corneal tear film, without altering the conjunctival epithelium [9, 10]. The purpose of this study was to evaluate safety and clinical performance over a period of four weeks, of an artificial tear containing arabinogalactan, trehalose and hyaluronic acid, in subjects with signs and symptoms of dry eye with documented inflammation of the ocular surface
Methods
We conducted a non-controlled, single center, prospective, cohort post-marketing study of an adult population at the private center Casa di Cura San Camillo in Lucca, Italy. Inclusion criteria were patient older than 30 years, subjects having signs and symptoms of dry eye for at least one month and who met at least three out of the following four criteria:
- OSDI cut off score 23, assessed with the Ocular surface disease index (OSDI) questionnaire, criteria of a previous diagnosis of dry eye.
- Non-invasive breakup time score (NIBUT) score<10 seconds in at least one eye.
- MMP9 levels in tears > 40 ng/ml, as assessed by inflammatory test in at least one eye.
- Conjunctival hyperemia score >1 and <4, based on the Efron classification system.
Exclusion criteria were the use of contact lenses, eyelid disorders (e.g., blepharitis, keratosis, history of trauma, hordeolum), patients who were participating in other clinical trials or being treated with medications that may interfere with clinical outcomes. Twenty-five patients were screened for eligibility; all patients had a clinical diagnosis of DED based on the inclusion criteria. This study was conducted in accordance with the Declaration of Helsinki and approved by the Regional Ethics Committee for clinical trials of the Tuscany Region, Sezione Area Vasta Nord Ovest (approval no.17690 dated on July 23rd, 2020). Informed consent was obtained from all participants.
The study group consisted of 25 patients with DED who were assigned to receive a combination ophthalmic solution, based on AG, trehalose and HA, one drop three times a day (T0) for seven days (T1), and subsequently according to their symptoms, until the fourth week (T2). The formulation used is a sterile, preservative free, lubricant ophthalmic solution containing AG, trehalose, HA sodium salt, D-panthenol, Vitamin E-TPGS, sodium tetraborate, boric acid and water for injections as inactive ingredient. The product owns an Int. Patent (PTC WO2021/074782A1), is currently authorized and marketed in several Countries as Class IIB Medical Device.
Ocular Examinations
A single examiner performed all ocular examinations. These included, at enrolment (T0) and after four weeks (T2): slit-lamp examination of the anterior segment, unaided and corrected visual acuity, NIBUT, osmolarity, meniscometry, ocular protection index (OPI), evaluation of conjunctival hyperemia according to Efron’s classification, the presence of MMP-9, conjunctival and corneal staining (Oxford score) and intraocular pressure. NIBUT was measured using Computerized Corneal Topography (OCT MS39 instrument, CSO) where Placido disk technology allows for the advanced analysis of the tear film. Performed for each eye, the results are provided directly by the diagnostic equipment. The specular image of a pattern projected onto the tear film, is examined. The time taken for the image to degrade, after the last blink, is defined as the NIBUT.
Tear osmolarity was measured in each eye using Tear lab (Tear Lab Corp., San Diego, CA, USA). The test card was inserted into the Tear lab system pen, which was used to collect 50 nL of tear fluid by the test card from the inferior lateral layer of the tear film. After collection, the system pen was docked into the system which displayed the result. Abnormal tear osmolarity was defined as an osmolarity value ≥308 mOsm/L in one eye, or a difference of ≥8 mOsm/L between the eyes [11, 12, 13]. Since osmolarity measurement can be affected by ambient temperature or humidity, tests were performed by a single examiner in a set location to minimize error. If the tear film break up time (TFBUT) is shorter than the inter-blink interval (IBI), the eyes are exposed to the risk of ocular surface damage. Ocular Protection Index (OPI) is the ratio between TFBUT and IBI (TFBUT/IBI), If the OPI score is < 1, patients have an exposed ocular surface, putting them at risk for the development of the signs and symptoms of dry eye, whereas if the OPI is >or=1.0, patients’ ocular surface is tear film protected.
Meniscometry testing was performed for each eye by using Tear check equipment by computerizing analysis of the high-definition images of the anterior segment of the eye. A rotatable projection system with a target comprising black and white stripes is projected onto the lower central tear film meniscus. Images are recorded and then transferred to a computer for calculation of the radius of tear meniscus curvature. Limbal and bulbar redness classification detects the fluidity of the blood vessels of the conjunctiva, Conjuntival hyperemia score was graded using a scale ranging from 0 (none) to 3 (severe).(Efron scale) [14]. A central picture must be taken to assess limbal redness. Therefore, nasal and temporal pictures must be taken to assess bulbar redness. Efron did not report mean healthy population values, although it was claimed that grade 0-1 was clinically normal. The clinical difference to detect is 0.5 grading [14]. For corneal and conjunctival staining, 4 µL of 1% fluorescein solution and 4 µL of 1% lissamine green were used; the results were scored based on the criteria of the Sjogren’s International Collaborative Clinical Alliance [15].
Based on fluorescein stain test, the extent of corneal epithelial injury (0-6) was scored as 0 if there were no punctate epithelial erosions, 1 if there were 1-5 erosive lesions, 2 if there were 6-30 erosive lesions, and 3 if there were >30 erosive lesions. In addition, 1 point each was added if confluent fluorescein staining was observed, if staining was observed in the pupil, or if at least 1 filament was observed. The total score was defined as the corneal staining score. Lissamine green staining of the conjunctiva was scored as 0 if there were 0-9 punctate erosive lesions, 1 if there were 10- 32 lesions, 2 if there were 33-100 lesions, and 3 if there were >100 lesions. The ocular staining score (OSS) was evaluated, out of a total of 12 points, as the sum of the corneal staining score and the nasal and temporal conjunctival staining scores.
For MMP-9 detection, Inflamma Dry (Rapid Pathogen Screening Inc., Sarasota, FL, USA) was used to obtain a single measurement from one eye; the patient didn’t receive any eye drops for 2 hours prior to tear collection. The lower lid was everted, and tears were collected from 8-10 points. The collected sample was combined with the included test cassette, the absorbent tip was immersed in the buffer solution for 20 seconds, and the results of the test were interpreted after 10 minutes. After 10 minutes, if the MMP-9 concentration is > 40 ng/mL, a red line and blue line are both observed in the result window, and the test is interpreted as positive for MMP-9 [16]. Although the intensity of the red line can vary, in this study a red test line was interpreted as positive, irrespective of intensity. Each patient was assessed by the same ophthalmologist at day 0 (enrollment, baseline) and after four weeks.
Questionnaire
Ocular surface disease index (OSDI) score, tolerability and adherence were used to evaluate subjective ocular symptoms at T0, T1 and T2.OSDI score ranged from 0 to 100 points. Higher scores indicated increased discomfort due to dry eye disease. Tolerability assessment included signs and symptoms of discomfort such as a burning sensation, itching and blurred vision with a range from 0 to 10 points. Adherence to treatment was assessed by the patient based on the subjective number of instillations calculated at baseline (T0), after one week (T1) and at the end of the follow-up period (T2).
Statistical Analysis
OSDI score, tolerability and adherence to treatment were evaluated at T0, T1 and T2 using a non-parametric Wilcoxon for paired data. Clinical parameters were evaluated at T0 and T2 using a non-parametric Wilcoxon for paired date. P value less than 0.05 was considered statistically significant.
Results
In this study, it has been evaluated a group of 25 patients with dry eye and documented symptoms and signs of inflammation of the ocular surface. Patients’ age ranged from 57 to 71 years. At baseline, the study group had homogenous demographic characteristics (Table 1).
| Demographics and screening data | Total | M | F |
|---|---|---|---|
| Patient number | 25 (100%) | 5 (20%) | 20 (80%) |
| Age, median (IQR) | 63 (57-71) | 70 (61-72) | 63 (57-70) |
| Current and past eye conditions or eye surgery events? | |||
| NO | 24 (96%) | 5 (100%) | 19 (95%) |
| YES | 1 (4%) | 0 (0%) | 1 (5%) |
| Systemic diseases present | |||
| Connective tissue pathologies | 1 (4%) | 0 (0%) | 1 (5%) |
| Diabetes mellitus | 1 (4%) | 0 (0%) | 1 (5%) |
| Hepatitis C | 0 (0%) | 0 (0%) | 0 (0%) |
| Acne | 0 (0%) | 0 (0%) | 0 (0%) |
| High blood pressure or heart disease | 5 (20%) | 0 (0%) | 5 (25%) |
| Depression or psychosis | 1 (4%) | 0 (0%) | 1 (5%) |
| Oncological pathologies | 0 (0%) | 0 (0%) | 0 (0%) |
| Thyroid disease | 3 (12%) | 1 (20%) | 2 (10%) |
| Menopause or ovarian dysfunction | 0 (0%) | - | 0 (0%) |
| Allergy | 1 (4%) | 0 (0%) | 1 (5%) |
| Vitamin deficiencies | 0 (0%) | 0 (0%) | 0 (0%) |
Table 1: This table shows the characteristics of the 25 enrolled patients at baseline.
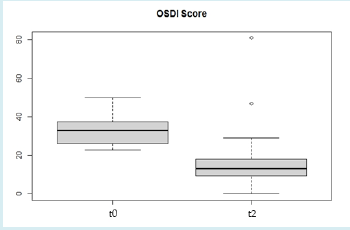
OSDI score showed a statistical reduction at T1, maintained at T2. Tolerability (burning sensation, itchy eyes and blurred vision) showed a marked improvement at T1. This improvement was not statistically significant between T1 and T2 because eye drops reduced symptoms). The evaluation of eye drops use showed that, at T1, all patients used them 3 times a day, at T2 this percentage dropped to 76%, since a lower dose demonstrated improvements. At the baseline the Study group OSDI score had a mean value of 32.9 at T2 there was a statistically significative reduction (value of 17.3) (Figure 1).
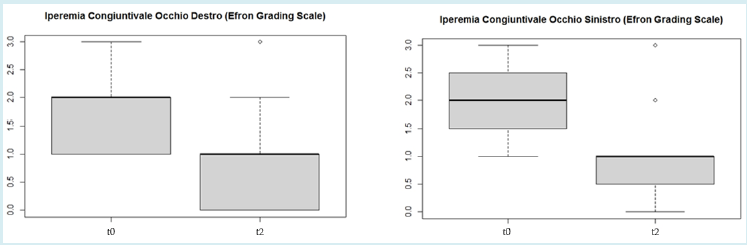
Conjunctival hyperemia grading by Efron scale showed a mean value of 1.9 in the right eye and 2 in the left eye, at the baseline, with a statistically significant reduction in both eyes after treatment (T2 right eye: 0.9, T2 left eye: 1) (Figure 2).
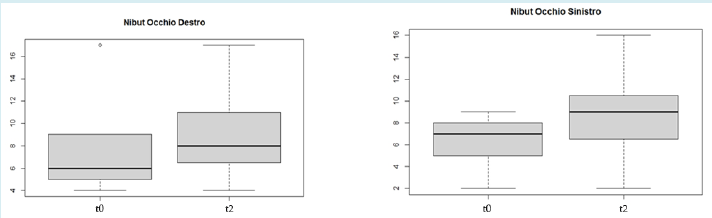
NIBUT showed a mean value of 7 at baseline in the right eye and 6.4 in the left eye, with a statistically significant improvement in both eyes after the treatment (p <0.05) (Figure 3).
Meniscometry test showed a mean value of 0.4 mm in the right eye and 0.3 mm in the left eye at baseline, with an increase of 0.5 mm in the right eye and 0.4 mm in the left eye after treatment (Figure 4).
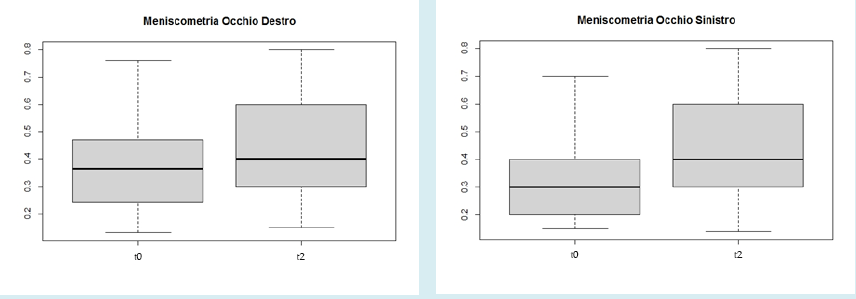
(A) (B) Figure 4: Meniscometry showed a statistically significant improvement in the study group after treatment in right eye (A) and in left eye (B) (*p<0.05).
Corneal-conjunctival staining grading by Oxford scale (mean value 0.6 in both eyes) showed a statistically significant reduction in both eyes after treatment. MMP9 test showed a statistically significant reduction of metalloproteinases in both eyes, at baseline all eyes tested positive (50 eyes of 25 patients) (it showed a mean value of 25 in both eyes) and, after four weeks, only 15 right eyes and 16 left eyes tested positive.(a value of 15 in the right eye and 16 in the left eye) (p<0.05). The other clinical parameters, although improved, did not show statistically significant changes.
Discussion
Dry eye disease is a common ocular disorder in daily clinical practice, and it is a growing challenge with a significant negative impact on quality of life and productivity [17, 18]. Epidemiological studies, made difficult by the heterogeneity and the lack of standardization in the definition of the disease and in diagnostic algorithms [19], have shown that DED prevalence ranges from 5% to 50% respectively [17, 18]. DED prevalence increases with age [18]. This study included a group of patients with clinical diagnosis of dry eye disease and presence of initial signs of inflammation. Parameters such as NIBUT, meniscometry, conjunctival hyperemia grading by Efron’s scale, osmolarity, corneal and conjunctival staining score, OSDI score and MMP9 test, have been evaluated at baseline and after four weeks of treatment. The Study group received a combination eye drop product based on, arabinogalactan, trehalose and hyaluronic acid.
This study shows a statistically significant improvement in OSDI score, conjunctival hyperemia grading by Efron’s scale, NIBUT meniscometry values, Oxford score and MMP9 results after treatment. This study explored the pathophysiological hypothesis of a relationship between inflammation and DED and demonstrated significant improvements from baseline on the inflammatory markers (especially MMP9). Inflammation, including innate immune response and adaptive response, is a key element of the vicious circle of DED. Mitogen-activated protein kinases and NF-kB signaling pathways, generation of inflammatory cytokines such as IL-1 and TNF-a and the up regulation of matrix metalloproteinase (MMP) produced by epithelial cells are involved in acute response. Adaptive response is triggered by the activation and migration of resident antigen-presenting cells to the regional draining lymph nodes, in which they stimulate naive T cells (Th0), leading to the expansion of IL-17-g and IFN-g-secreting Th17 (Th17/1) cells [20, 21]. Proteolytic enzymes, in particular MMP-9, play a key role in DED pathogenesis by disrupting epithelial cells tight junctions, leading to a breakdown of the ocular surface epithelial barrier. MMP-9 has recently been proposed as one of the best biomarkers of DED severity [22] and as a diagnostic biomarker that can be assessed by a point-of-care immunoassay [23]. The use of HA significantly improved tear production in patients suffering from ocular surface disorders. Multiple studies have highlighted these properties of hyaluronic acid through in vivo evaluations comparing groups of patients who used HA versus patients who did not use it [24].
Trehalose is one of the osmoprotectants found in Nature. It is a disaccharide present in numerous non-mammalian species; it allows cells to live in unfavorable environments. In fact, it is involved in anhydrobiosis, the ability of some plants and animals to resist prolonged drying periods. It has high water retention capacities and a exerts dual property, bioprotection and osmoprotection, by preserving corneal epithelial cells from oxidative damage induced by UV rays, accelerating healing and reducing conjunctival inflammatory cytokines (this property was demonstrated in a mouse model of DED); it helps restore osmotic balance of the ocular surface as well as prevents denaturation of the lipid bilayer and cell membrane proteins, in order to maintain corneal cell homeostasis.
Multiple in vitro and in vivo studies have shown that trehalose protects corneal epithelial cells from drying out and corneal and conjunctival epithelial cells from apoptosis. The first action is important because, by preserving epithelial cells from dehydration, cell membranes are in a liquid-crystal state even when the water content is very low. At the same time, it protects epithelial cells from hyperosmolarity of tear film, restoring cell volume [24]. A clinical study conducted in 2019 [25] published in Ocular Surface, demonstrated the efficacy of trehalose at a concentration of 1.2%, in improving the discomfort of patients with dry eye. This study compared trehalose 1.2 % with carboxymethylcellulose. Nine patients with dry eye syndrome were treated twice daily, in one eye, with carboxymethylcellulose and, in the contralateral, with trehalose for a period of thirty days. Inflammatory and autophagic cell markers were analyzed in vitro (cornea exposed to TNF-ά stress and drying) and in vivo (BUT and Schirmer test values in treated patients’ eyes). In vitro procedure confirmed that trehalose can reduce cytokine levels in cells and tear cytokine levels. In vivo procedure showed that trehalose can reduce eye symptoms compared to the contralateral eye treated with carboxymethyl cellulose. These results agree with those of previous studies, demonstrating the in vivo efficacy of both components: HA 0.25% with high molecular weight and trehalose 2%.
Arabinogalactan is a polysaccharide abundant in most plants, but it is usually derived from the bark of the Larch trees (Larix occidentalis, Larix decidua) of species. It is formed of arabinose and galactose in a ratio of 1:6 and a small amount of glucuronic acid [5]. The macromolecule, with a molecular weight ranging from 10.000 Da to 120.000 Da, has been approved by the FDA for oral consumption, even in large quantities (FDA, 2000). Arabinogalactan dispersions in ophthalmic solution (from 0.2% to 10%) have been investigated showing a Newtonian rheologic behavior and viscosity values ranging from 1.00 to 1.58 mPa*s. Viscosity of tear fluid is 1.02-1.93 mPa*s [11] and thickener agents are commonly added to ophthalmic formulations to prolong their retention time on the ocular surface. Arabinogalactan (5% w/w) has been reported as a novel mucoadhesive polysaccharide which can be used for the treatment of dry eyes and corneal wounds and to heal the dry spots on cornea [26]. In this concentration, arabinogalactan drops did not show any cytotoxicity effect on the rabbit corneal epithelium, whereas 0.01% w/w benzalkonium chloride was highly toxic.
After 24 h the arabinogalactan-treated cornea was well differentiated as an organized structure and after 48 h it was normal, marked by the presence of microvilli and glycocalyx, an unorganized structure of cells of different sizes, lack of microvilli and glycocalyx were found in the control formulation even after some days of administration [27]. A recent study [28] showed that the combination of AG and HA can produce a synergic effect and contribute to the reduction/inhibition of the xanthine + xanthine oxido- reductase reaction, thus the uric acid formation. The synergic effect of AG and HA is statistically proven. The uric acid inhibition due to the AG and HA combination is statistically superior to the sum of the single component inhibition. The same behavior has been observed in the reduction of ROS: the combination of AG and HA entails a significant reduction of free radicals, higher than the sum of the single component inhibition. This study demonstrated the synergic effect of AG and HA on the XOR complex and these results may represent a rationale to further clinical investigations on the beneficial effect of such eye drop formulation on the mitigation of the inflammatory process leading to the worsening of dry eye disease.
This synergic effect has been further confirmed by the measurement of diffusion coefficients D of water protons by DOSY (Diffusion Ordered Spectroscopy), the determination of viscosity and the investigation of the affinity of a small molecule molecular probe versus AG/HA mixtures in the presence of bovine sub maxillary mucin (BSM) by 1HNMR spectroscopy [29]. Enhanced mucoadhesive properties, decreased mobility of water and decreased viscosity were observed at the increase of AG/HA ratio and of total concentration of AG. This recent experiment confirmed, by using different methodologies, the virtuous interaction between AG and HA, which is supposed to form stable supramolecular aggregates able to incorporate more water molecules that result in less mobility in the end. In this clinical study was demonstrated, for the first time in the literature, the synergic effect of the three main components: AG, trehalose and HA. In this study we confirmed previous results on the use of trehalose and hyaluronic acid and, for the first time, we confirmed in vivo the results obtained in vitro with the use of AG and HA.
Conclusion
This is the first study to document the effectiveness of the combination of topical solution based on arabinogalactan, trehalose and hyaluronic acid in patients with DED. Preliminary findings suggest that this eye drops formulation can be effective in reducing dry eye evolution, in presence of signs and symptoms of inflammation. Patients did not experience any adverse event. Further studies with larger sample sizes and extended follow-up periods are needed to validate these results in real life setting
Ethics Approval and Consent to Participate
The included studies have been approved by the local ethics committees.
Consent for Publication
The study has been conducted in accordance with the declaration of Helsinki. Informed consent was obtained from all participants.
Additional Information Competing Interests
The authors declare that they have no competing interests.
Acknowledgements
This study was managed by MD Italy, Via Cancelliera 12, 00040 Albano Laziale, Roma (Italy) and CRO Hippocrates Research SrL, Via XX Settembre 30/12, 16121 Genova (Italy).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this study by a research grant of Bruno Farmaceutici SpA, Via delle Ande 15, 00144, Roma (Italy).
Trial Registration
This trial was registered at ClinicalTrials.gov Identifier: NCT04633863.
References
-
Smith RE (2005) The tear film complex: Pathogenesis and emerging therapies for dry eyes. Cornea 24(1): 1-7.
-
Wolffsohn JS, Arita R, Chalmers R, Djalilian A, Dogru M, et al. (2017) TFOS DEWS II diagnostic methodology report. Ocul Surf 15(3): 539-574.
-
Sullivan DA, Rocha EM, Aragona P, Clayton JA, Ding J, et al. (2017) TFOS DEWS II sex, gender and hormones report. Ocular Surf 15(3): 284-333.
-
Baudouin C, Irkec M, Messmer EM, Castillo JMBD, Bonini S, et al. (2018) Impact of inflammation in dry eye disease: proceedings of ODISSEY group meeting. Acta Ophthalmol 96(2): 111-119.
-
Dion C, Chappuis E, Rippol C (2016) Doe’s larch arabinogalactan enhance immune function? A review of mechanistic and clinical trials. Nutr Metabol 13(1): 28.
-
Chandrasekaran R, Janaswamy S (2002) Morphology of Western larch arabinogalactan. Carbohydr Res 337(21- 23): 2211-2222.
-
Fujishima H, Toda I, Shimazaki J, Tsubota K (1996) Allergic conjunctivitis and dry eye. Br J Ophthalmol 80(11): 994-997.
-
Pflugfelder SC, Jones D, Ji Z, Afonso A, Monroy D (1999) Altered cytokine balance in the tear fluid and conjunctiva of patients with Sjogren’s syndrome keratoconjunctivitis sicca. Curr Eye Res 19(3): 201-211.
-
Boulton M, Johnson ME, Murphy PJ (2005) Effectiveness of sodium hyaluronate eyedrops in the treatment dry eye. Graefes Arch Clin Exp Ophthalmol 244(1): 109-112.
-
Stuart JC, Linn JG (1985) Dilute sodium hyaluronate in the treatment of ocular surface disorders. Ann Ophthalmol 17(3): 190-192.
-
Lemp MA, Bron AJ, Baudouin C, Castillo JMBD, Geffen D, et al. (2011) Tear osmolarity in thediagnosis and management of dry eye disease. Am J Ophthalmol 151(5): 792-798.
-
Jacobi C, Jacobi A, Kruse FE, Cursiefen C (2011) Tear film osmolarity measurements in dry eye disease using electrical impedance technology. Cornea 30(12): 1289- 1292.
-
Sullivan B (2014) Challenges in using signs and symptoms to evaluate new biomarkers of dry eye disease. Ocul Surf 12(1): 2-9.
-
Efron N (1998) Grading scales for contact lens complications. Ophthalmic Physiol Opt 18(2): 182-186.
-
Whitcher JP, Shiboski CH, Shiboski SC, Heidenreich AM, Kitagawa K, et al. (2010) A simplified quantitative method for assessing keratoconjunctivitis sicca from the Sjogren’s Syndrome International Registry. Am J Ophthalmol 149(3): 405-415.
-
Kaufman HE (2013) The practical detection of MMP-9 diagnoses ocular surface disease and may help prevent its complications. Cornea 32(2): 211-216.
-
Patel DS, Arunakirinathan M, Stuart A, Angunawela R (2017) Allergic eye disease. BMJ 359: j4706.
-
Stapleton F, Alves M, Bunya VY, Jalbert I, Lekhanont K, et al. (2017) TFOS DEWS II epidemiology report. Ocul Surf 15(3): 334-365.
-
Leonardi A, Doan S, Fauquert JL, Bozkurt B, Allegri P, et al. (2017) Diagnostic tools in ocular allergy. Allergy 72(10): 1485-1498.
-
Chen Y, Chauhan SK, Shao C, Omoto M, Inomata T, et al. (2017) IFN-g-expressing Th17 cells are required andfor development of severe ocular surface autoimmunity. J Immunol 199(3): 1163-1169.
-
Komi DEA, Rambasek T, Bielory L (2018) Clinical implications of mast cell and involvement in allergic conjunctivitis. Allergy 73(3): 528-539.
-
Fraga JP, Salamanca AED, Calonge M, Garca MJG, Migue AL, et al. (2018) Severity, therapeutic, and activity tear biomarkers in dry eye disease: An analysis from a phase III clinical trial. Ocul Surf 16(3): 368-376.
-
Messmer EM, Lindenfels VV, Garbe A, Kampik A (2016) Matrix metalloproteinase 9 testing in dry eye disease using a commercially available point-of-care immunoassay. Ophthalmology 123(11): 2300-2308.
-
Yang YJ, Lee WY, Kim YJ, Hong PY (2021) A meta-analysis of the efficacy of hyaluronicacid eyes drops for the treatment of dry eye syndrome. Int J Environ Res Public Health 18(5): 2383.
-
Panigrahiac T, Shivakumar S, Shetty R, D’souzab S, Nelson EJR, et al. Trehalose augments autophagy to mitigate stress induced inflammation in human corneal cells. Ocul Surf 17(4): 699-713.
-
Burgalassi S, Nicosia N, Monti D, Falcone G, Boldrini E, et al. (2007) Larch arabinogalactan for dry eye protection and treatment of corneal lesions: investigations in rabbits. J Ocul Pharmacol Ther 23(6): 541-550.
-
Burgalassi S, Nicosia N, Monti D, Falcone G, Boldrini E, et al. (2011) Arabinogalactan as active compound in the management of corneal wounds: in vitro toxicity and in vivo investigations on rabbits. Curr Eye Res 36(1): 21-28.
-
Silvani L, Bedei A, Grazia GD, Remiddi S (2020) Arabinogalactan and hyaluronic acid in ophthalmic solution: Experimental T effect on xanthine oxidoreductase complex as key player in ocular inflammation (in vitro study). Exp Eye Res 196: 108058.
-
Mola AD, Summa FF, Oliva P, Lelj F, Remiddi S (2021) Synergistic Properties of Arabinogalactan (AG) and Hyaluronic Acid (HA) Sodium Salt Mixtures. Molecules 26(23): 7246.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report