Management of Arteritic Anterior Ischemic Optic Neuropathy Post Renal Transplant
This case report helps us to understand, in a comprehensive manner, the management of anterior ischemic optic neuropathy using a multidisciplinary approach. The case taken for this study involves a young female who underwent a kidney transplant due to chronic kidney disease and presented to us with a unilateral painless loss of vision. It has been reported that prompt administration of steroids may be associated with partial recovery of the eye involved. But otherwise, the prognosis in such cases is usually poor. However, since our patient was post-renal transplant and was already taking immunosuppressive drugs, the fear of impending infections due to severely compromised immunity by both steroids and immunosuppressive therapy was there. Hence, a multidisciplinary approach was applied, involving a nephrologist, a physician, and an anesthetist as well. The recommendation for admission in a hygiene room with a dialysis facility in the hospital, monitoring of immunosuppressive therapy, and pulse-dose steroids to be started under the care of an anesthesiologist was the appropriate management.
Introduction
Anterior ischemic optic neuropathy (AION) is an acute optic neuropathy that occurs predominantly in elderly patients with metabolic derangements. AION occurs due to inflammation and subsequent thrombosis of the short posterior ciliary artery, which originates from the ophthalmic artery and results in optic nerve head ischemia. Urgent management is required in such cases, and the overall visual prognosis remains extremely guarded [1]. Our patient was a known case of chronic kidney disease post- renal transplant (live kidney recipient: father was the donor) before two months. Patients with chronic kidney disease are predisposed to thrombosis and accelerated atherosclerosis due to increased oxidative stress, a state of inflammation and malnutrition, endothelial dysfunction, anemia, and disrupted calcium and phosphate metabolism, apart from traditional risk factors. This case depicts a multidisciplinary approach to management of such cases with the involvement of a nephrologist, an anesthesiologist, and a physician.
Case Report
A 24 year old female nursing student, a known case of chronic kidney disease, presented with sudden painless loss of vision in her right eye for one week. The patient gave a history of renal transplant (end stage renal disease secondary to hypertension) before two months, after which she was kept on oral steroids and immunosuppressive therapy. On examination, the best-corrected visual acuity (BCVA) of right eye (OD) was 20/800 and left eye (OS) was 20/20. Intraocular pressure (IOP) was 12 and 14 mm Hg in OD and OS respectively. On anterior segment examination, relative afferent pupillary defect (RAPD) was noted in the OD, rest of the examination was within normal limits. On OD fundus examination (Figure 1a), the disc margin appeared blurry with severe ischemia in form of whitish superficial exudates resembling cotton wool spots, and superficial hemorrhages were seen. Vascular tortuosity and sclerosis were also noted at the posterior pole. Over the macula, a patch of greyish white retina was seen under the fovea, along with early arterial ischemic changes. An OCT scan of the OD (Figure 1b) was advised, which showed severe hyper-reflectivity of the inner retina and sub-retinal fluid with whitish hyper- reflective deposits. OS was within normal limits.
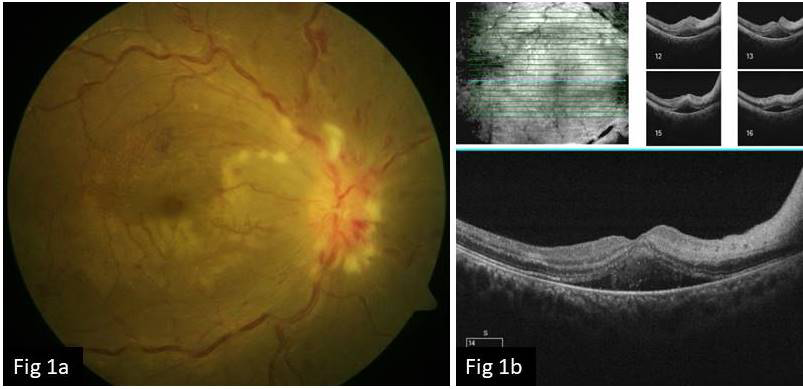
Figure 1a, b: Right eye fundus photo a) shows the disc margin appears blurry with severe ischemia in form of whitish superficial exudates resembling cotton wool spots, superficial hemorrhages, vascular tortuosity and sclerosis at the posterior pole. Over the macula, a patch of grayish white retina is seen under the fovea, along with early arterial ischemic changes. An OCT scan. b) of the right eye shows severe hyper-reflectivity of the inner retina and sub-retinal fluid with whitish hyper-reflective deposits.
On the basis of these findings, a diagnosis of Anterior Ischemic Optic Neuropathy and branched retinal artery occlusion was established. She was advised to begin intravenous pulse dose steroid therapy followed by tapering doses of oral steroid. The aim of therapy here was to salvage the existing vision, and guarded visual prognosis was clearly explained. Since she was already on immunosuppressive therapy, the dilemma here was to manage the dosage in a way so that she doesn’t succumb to infection in view of her extremely suppressed immunity. Her treating nephrologist was consulted in this regard. She recommended admission in a hygiene room with an in-house dialysis facility and resuscitation kit, continuation of immunosuppressive therapy, and pulse dose steroids to be started under the care of an anesthesiologist. After one month post treatment, the BCVA improved to 20/200 and the IOP was 16 mm Hg in both eyes. The disc edema had subsided and pallor had set in. The peripapillary vessels appeared sclerosed, vessel tortuosity had reduced, and the peripheral hemorrhages had subsided. There were sub retinal yellow deposits over the macula with evident foveal thinning (Figure 2a). The OCT revealed resolution of the inner layer hyperreflectivity and serous retinal detachment and the foveal thinning with central foveal thickness of 110 microns (Figure 2b), accounting for the 20/200 vision. The OCT-A (Figure 3a, 3b) corresponds to the loss of capillaries mainly in the deep retinal plexus, which justifies the significant ischemia and subsequent permanent loss of vision.
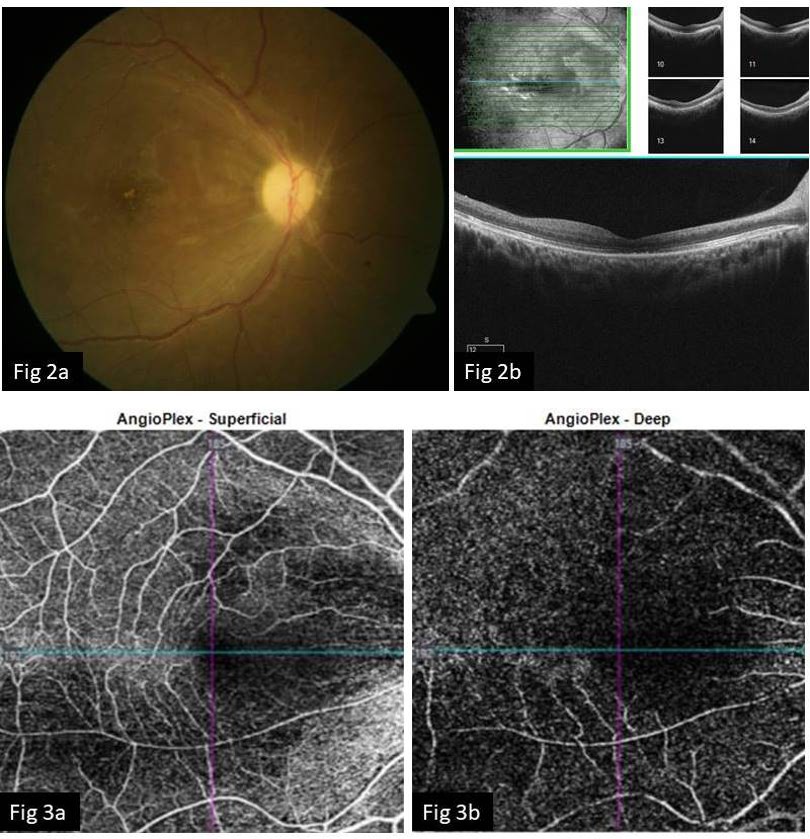
Figure 2a, b: Right eye fundus photo post treatment a) shows subsided disc edema and secondary pallor. The peripapillary vessels appear sclerosed, vessel tortuosity has reduced, and the peripheral hemorrhages have subsided. There are sub retinal yellow deposits over the macula with evident foveal thinning. The OCT scan b) reveals resolution of the inner layer hyper reflectivity and serous retinal detachment and the foveal thinning with central foveal thickness of 110 microns, accounting for the 20/200 vision.
Figure 3a, b: The OCT-A scan post treatment shows the loss of capillaries in the superficial and in the deep retinal plexus (significant in the deep plexus), which justifies the significant ischemia and loss of vision.
Discussion
Anterior ischemic optic neuropathy is a disease of old age most commonly associated with giant cell arteritis, which can be of arteritic or non-arteritic variety. In our case, the patient was a young female with chronic kidney disease who was post-renal transplant. In such patients, there is an increased tendency of atherosclerosis of blood vessels due to hypercalcaemia and an increased tendency towards inflammation and thrombosis of vessels due to an increased fibrinogen level to compensate for platelet dysfunction. Dendritic cells residing in the vessels walls are the key contributors to the AION, in addition to macrophages recruiting T cells. A significant immune response is initiated by a variety of interleukins, which are the cause of the severe onset of inflammation. Since this can also cause axonal flow blockage, irreversible damage to the optic nerve head and macula is destined if not treated timely. Platelet count is often elevated acutely in AION and can be used in conjunction with elevated ESR and CRP levels to make a preliminary diagnosis [2].
The acute inflammation can be suppressed with glucocorticoids or immuno-modulatory drugs. In the post- kidney transplant period, recipients receive induction immunosuppression in the form of depleting (Anti- thymocyte globulin) or non-depleting agents (basiliximab) depending on the immunological risk. From there on, patients are usually on maintenance immunosuppression with three drugs: steroids, an antiproliferative agent like mycophenolate mofetil (MMF) or azathioprine, and either a calcineurin inhibitor or a mTOR inhibitor [3]. In the early post-transplant period, patients with any immune mediated phenomenon, including rejection, are treated by increasing the immunosuppression. In this case, the patient received pulse IV MPS 1 gram for 3 days (during which oral steroids were withheld) and was switched to oral prednisolone 1 g/ kg/day in a tapering dose over 4 weeks. She was kept on tacrolimus and MMF. An immune-mediated phenomenon in the early post-transplant period without rejection of the graft kidney is rare. This case is a rarity in terms of its occurrence as well as the outcome achieved. For ophthalmologists, it’s extremely important to have a multidisciplinary approach in such cases to achieve the best possible outcome.
Conclusion
This report highlights a multidisciplinary approach in cases of AION post renal transplant in an ophthalmology clinic and depicts the importance of a multidisciplinary management by involving a nephrologist, physician, and anesthetist in such cases.
References
-
Hayreh SS (2011) Management of Ischemic Optic Neuropathies. Indian J Ophthalmol 59(2): 123-136.
-
Hayreh S (1990) Anterior Ischaemic Optic Neuropathy Differentiation of Arteritic from non-arteritic type and its management. Eye 4( Pt 1): 25-41.
-
Thongprayoon C, Hansrivijit P, Leeaphorn N, Acharya P, Ortiz AT, et al. (2020) Recent Advances and Clinical Outcomes of Kidney Transplantation. J Clin Med 9(4): 1193.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report