Non-Surgical Pneumatic Repair of Stage 2 Macular Holes
Purpose: We report anatomical and functional outcomes of gas injection for small-medium full thickness macular holes (FTMH) with vitreomacular traction (VMT). Methods: This retrospective-comparative case series included patients with stage 2 FTMH who underwent intravitreal injection of perfluoropropane (C3F8) or sulfur hexafluoride (SF6) gas. Clinical evaluation included B-scan ultrasonography and spectral-domain optical coherence tomography (OCT) to assess post-procedure MH closure, vitreous status, and visual outcomes. Results: There were five men and seven women with a mean age of 63.75 years (range: 54-76). The median duration of symptoms was 8.5 months (range: 2-52 months). The mean BCVA at presentation was 0.51 LogMAR (Snellen equivalent 20/65). The mean macular hole aperture size was 206 (range: 127-334). In eight (67%) patients, FTMH closed after gas injection. All the four open holes underwent vitrectomy. The median follow-up was 11 months (range: 2-53 months). At the last follow-up, all the patients had type 1 MH closure; BCVA improved in 10 (83%). The mean post-treatment BCVA was 0.28 LogMAR (Snellen equivalent 20/38). One patient developed retinal tears, which were successfully treated with barrage laser photocoagulation. Conclusion: Intravitreal gas injection is a valid treatment modality for non-surgical macular hole closure, especially in smallmedium FTMH. Gas-assisted PVD induction and release of VMT provides a viable option for patients unwilling/unfit for vitrectomy, with no carry-over disadvantage in subsequent surgery in case of macular hole non-closure.
Introduction
Idiopathic macular holes are an important cause of visual loss in the elderly population. The Gass classification based on careful clinical examination divided macular holes (MH) into 4 stages [1]. Optical coherence tomography (OCT) enhanced the understanding of pathogenesis and progression of MH [2, 3]. The International Vitreomacular Traction Study (IVTS) Group classified macular holes based on role of vitreous traction, hole size and concurrent vitreomacular traction (VMT) [4]. The stage 2 macular hole of Gass classification paralleled primary small-medium sized MH with concurrent VMT. Although idiopathic macular holes may close spontaneously in about 3% to 11% of cases [5, 6, 7], surgical repair employing vitrectomy and release of causative tractional forces is an established procedure for the treatment of small macular holes. Overall success rates of macular hole surgery reported in the literature are over 90% after a single operation [8]. Since vitrectomy carries risks [9], a less invasive alternative may provide benefits in terms of safety, reduced morbidity, convenience, and cost. Pharmacological vitreolysis with Ocriplasmin has been considered in macular holes with concurrent VMT [10, 11, 12, 13, 14, 15], thereby avoiding surgery in these patients. Although the macular hole closure rate with Ocriplasmin was around 40%, the post-market safety concerns, limited access and prohibitive cost are significant limitations to its widespread use [11, 12, 14]. Intravitreal injection of expansile gas has been shown to induce release of vitreofoveal traction in stage 2 macular hole [16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29]. This treatment option may provide an alternative for patients who have difficulties with surgery and postoperative positioning. The present study aimed to incorporate OCT to evaluate anatomical & functional outcomes following intravitreal-gas-induced VMT separation in stage 2 MH.
Patients and Methods
This retrospective non-comparative case series included 12 eyes of as many patients with stage-2 macular holes with minimum aperture diameter < 400µ. All patients in the series underwent intravitreal injection of expansile gas (perfluoropropane, C3F8; or sulfur hexafluoride, SF6) to close the macular hole non-surgically. We report the anatomical and functional outcomes of the patients who completed post-procedure follow-up of at least 2 months. A waiver for this retrospective review of records was obtained from the institutional ethics committee. A detailed ophthalmologic examination was performed including best-corrected visual acuity assessment (BCVA), intraocular pressure recording, slit lamp bio microscopy and dilated indirect ophthalmoscopy with scleral depression. Special attention was given to any peripheral degenerations predisposing to retinal tear/detachment, which were duly barraged with laser photocoagulation, when present. Status of posterior vitreous detachment was assessed and graded using B-scan ultrasonography and spectral domain optical coherence tomography (OCT) (Topcon 3D-1000 Topcon, Tokyo, Japan or Heidelberg Retinal Analyzer, Heidelberg Engineering, Germany) [30, 31]. The stage of PVD was recorded as outlined by Johnson et al using ultrasonography and OCT [14]. All patients were offered the options of pneumatic macular hole repair or vitrectomy. The patients who were not compliant for primary vitrectomy were enrolled for the pneumatic procedure. The future need for vitrectomy in case of failure of the non-surgical procedure was clearly explained. After discussion of the head posturing requirements, a written informed consent was obtained from each of the patients in accordance with the tenets of the Declaration of Helsinki. All the procedures were performed in the operating room by either of the authors.
After prepping and draping under topical anesthesia, a self-retaining wire speculum was inserted to avoid eye lashes in the surgical field. After anterior chamber paracentesis, 0.3-0.4 cc of pure C3F8 or 0.5mL of SF6 gas was injected 3.5 mm posterior to the surgical limbus using a ½-inch 30-gauge needle. We preferred C3F8 gas in myopic eyes to achieve a greater arc of contact. When the axial length was 25mm or longer, we used 0.4mL of C3F8. After injection, all patients were instructed to maintain face-down position for 7-10 hours a day. The patients were first reviewed at 6-8 hours, subsequently at days 1,7 and 14 postoperatively, and monthly thereafter. All patients underwent dilated fundus examination and intraocular pressure assessment at each visit. Ultrasonography and OCT were performed at each visit after week 2 postoperatively. The following information was retrospectively recorded after reviewing patient charts: age, gender, prior ocular history, duration of symptoms, BCVA, phakic status, macular hole dimensions, and status of PVD at presentation and the most recent follow-up, complications, and duration of follow-up. The aperture size of the macular hole was measured using the caliper function of OCT at the narrowest horizontal width in the mid retina, parallel to the retinal pigment epithelium [4]. Hole closure was defined as complete apposition of the edges with central continuity of photoreceptor layer. Statistical analysis was performed using STATA 11.1 (Texas, USA) software Mean (SD) and frequency (percentage) was used for continuous and categorical variables respectively. Paired t-test test and Wilcoxon sign- rank test were used to compare difference in means between preoperative and final visits. Mann-Whitney U test was used to compare means between two groups. Pearson correlation was used to determine correlation between two continuous variables. Kruskal-Wallis H test was used to compare means between more than two groups. The P-value less than 0.05 were considered statistically significant.
Results
This retrospective interventional study included 5 men and 7 women with a mean age of 63.75 years (range, 54 to 76 years) at the time of the interventional procedure. Eight (66.7%) of the 12 study eyes had previously undergone cataract surgery with implantation of posterior chamber intraocular lens. The median duration of symptoms was 8.5 months (range: 2-52 months, Mean: 14.4 months). The macular hole was bilateral in 2 patients, in whom the fellow eye had stage 4 macular hole. The mean logMAR BCVA at presentation was 0.51. Eight (66.7%) patients had BCVA worse than 0.3 in the study eye prior to the procedure. The mean macular hole aperture size was 206µ (range, 127 to 334µ). Two eyes had myopic axial length (24mm
and 24.5mm) and received 0.5mL C3F8 gas. Vitreofoveal separation was observed by ultrasonography in all the patients at 2 weeks. The macular holes gradually closed over the following 3-4 weeks (Figure 1).
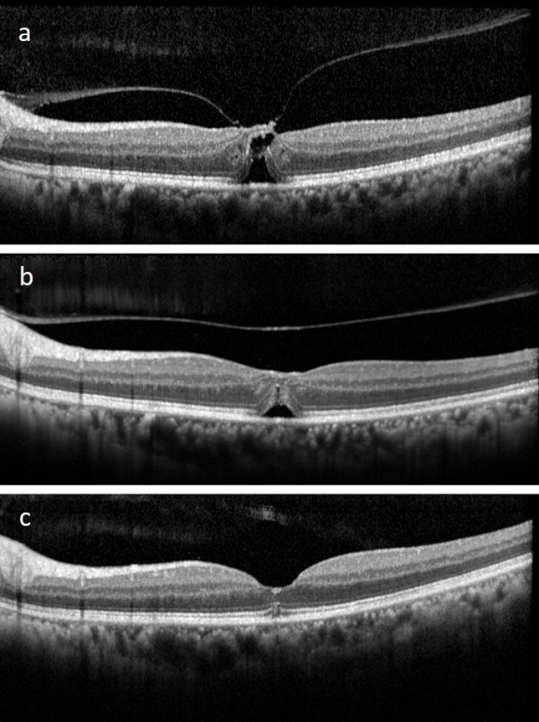
Figure 1: This 74-year-old lady (Case 8) had visual decline in her left eye for about a year. The best-corrected visual acuity (BCVA) was 20/120. a) Optical coherence tomography (OCT) revealed a small full-thickness macular hole (128µ) with vitreofoveal traction. b) A month after intravitreal injection of 0.4mL 100% sulfur hexafluoride gas, the vitreofoveal traction was released, with closure of macular hole. c) Remodeling of the foveal contours continued 3 months post-procedure with a central continuity of the photoreceptor layer. The ellipsoid zone was still interrupted centrally. BCVA had improved to 20/80. Status quo was maintained over the following year.
A primary type 1 closure of the macular holes was observed in 5/5 eyes with C3F8 and 4/7 eyes with SF6 gas respectively. However, one macular hole in the C3F8 group re-opened after 8 months; and was closed successfully with vitrectomy, internal limiting membrane peeling and SF6 gas tamponade. Three macular holes that failed to close with SF6 injection were also similarly closed with vitrectomy. The final success rate purely with gas injections was therefore 67% (8/12 eyes). The median duration of follow-up was 11 months (range, 2 to 53 months, mean: 20.5 months). At the last follow-up, all the patients had type 1 macular hole closure. None of the patients experienced an increase in intraocular pressure during any of the post-procedural examinations. The mean post-treatment BCVA was 0.3 (Snellen BCVA 20/40); ten (83%) patients improved to this or better BCVA. Four (25%) eyes improved to a BCVA of 0.1(Snellen ≈20/25) or better. The difference between mean preoperative and final LogMAR BCVA was statistically significant (p= 0.002). There was no significant difference in the final BCVA in eyes with intact ellipsoid band (p=0.143) or myoid band (p= 0.643) and those with disrupted ellipsoid and myoid bands respectively. The results are summarized in the Table 1. One of the study eyes developed horse-shoe tears related to the development of PVD following the procedure. Since he had already undergone a prophylactic laser photocoagulation for lattice degeneration, the tears failed to cause a retinal detachment (RD). The barrage laser photocoagulation was reinforced; the patient maintained a stable retinal attachment. No other major complications like lens injury, intraocular hemorrhage, epiretinal membrane, visual field defects or endophthalmitis were observed.
| S. No. | Age (years) | Sex | Symptom duration (weeks) | Eye | Initial LogMAR BCVA | MH | Follow-up (months) | Final LogMAR BCVA | Gas | MH status post- gas | MH status Final | Ellipsoid band integrity | Myoid band integrity |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Size (µ) | |||||||||||||
| 1 | 59 | F | 26 | Right | 0.3 | 201 | 7 | 0.1 | C3F8 | Closed | Closed | Present | Present |
| 2 | 55 | M | 2 | Left | 0.6 | 260 | 2 | 0.6 | C3F8 | Closed | Closed | Absent | Present |
| 3 | 58 | M | 3 | Left | 0.48 | 127 | 33 | 0.3 | C3F8 | Open | Closed | Absent | Absent |
| 4 | 72 | M | 25 | Left | 0.3 | 209 | 53 | 0 | C3F8 | Closed | Closed | Absent | Absent |
| 5 | 76 | M | 3 | Left | 0.3 | 223 | 41 | 0.18 | C3F8 | Closed | Closed | Absent | Absent |
| 6 | 56 | F | 3 | Left | 0.48 | 187 | 2 | 0 | SF6 | Closed | Closed | Present | Present |
| 7 | 59 | F | 18 | Left | 0.6 | 194 | 15 | 0.3 | SF6 | Closed | Closed | Present | Present |
| 8 | 74 | F | 52 | Left | 0.78 | 128 | 12 | 0.6 | SF6 | Closed | Closed | Absent | Present |
| 9 | 63 | M | 9 | Left | 0.6 | 248 | 10 | 0.3 | SF6 | Open | Closed | Absent | Present |
| 10 | 54 | F | 9 | Left | 0.6 | 131 | 30 | 0 | SF6 | Open | Closed | Present | Present |
| 11 | 70 | F | 8 | Right | 0.3 | 238 | 7 | 0.18 | SF6 | Open | Closed | Absent | Present |
Table 1: Demographics & post-pneumatic repair outcomes in stage 2 small-medium macular holes. BCVA: best-corrected visual acuity;
Discussion
Vitreomacular traction plays an important role in the pathogenesis of idiopathic macular hole [1, 2, 3, 32, 33, 34]. Early- stage small macular holes are associated with a small rate of spontaneous closure [7, 35, 36]. Despite its high success rates, macular hole surgery may be associated with intraoperative (retinal tears, lens touch, retinal hemorrhage) and postoperative (acceleration of nuclear sclerosis, field defects, retinal detachment) complications [6, 7, 9]. In addition, peeling of internal limiting membrane may be associated with reduced retinal sensitivity (on microperimetry), nerve fiber layer trauma (swelling or dissociated nerve fiber layer defects) and potential dye-related toxicity [37, 38]. Enzymatic vitreolysis with Ocriplasmin, albeit carrying a lower success rate than vitrectomy, may provide an alternative for patients who have overriding travel needs that preclude a gas injection; or who prefer to avoid cataract surgery. However, its lower success rate and high cost limit the cost-effectiveness as compared to surgical vitrectomy in treatment of vitreomacular adhesions and macular holes [39, 40]. Studies exploring the utility of intravitreal injection of expansile gas in the treatment of stage 2 macular holes demonstrated its safety and efficacy [16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29]. Both C3F8 and SF6 in volumes of 0.2-0.5cc have been used to induce a separation of vitreofoveal traction with few side effects [11, 12, 13]. However, recent studies have used C3F8 almost universally [19, 20, 21, 22, 23, 24, 25], most likely because of its greater bang for buck value: a wider arc of contact with a lower volume of injection. This is especially useful in myopic eyes, where an early dissolution of gas could cause treatment failure. Han, et al. in fact extended the prone positioning for another week with C3F8 if the macular hole didn’t close within a week [25]. This strategy is not possible with SF6 and thus may contribute to its lesser efficacy in inducing VMT release [26]. However, a recent DRCR Net trial was aborted because of an unacceptably high rate of complications (14% RD) with C3F8 injection, notwithstanding a modest success rate (29%) in very small (average diameter: 79µ) macular holes [24]. Notably, they didn’t mention preoperative prophylaxis for retinal degenerations, and paracentesis was optional. We chose the gases according to axial length and obtained a high success rate of 67% (75%; if we discount the late re-opening of closed macular hole, which can occur even after vitrectomy). However, we didn’t suffer the same complications, especially RD [24, 25], probably because of careful inspection and prophylactic treatment of any peripheral lesions before gas injection. This precaution saved a certain RD in a myopic eye where retinal tears developed within already well-barraged lattices. The advice to maintain facedown positioning was short-term (3-7 days) and liberal (as much as patients could comfortably manage). The rapid release of VMT within hours or days also suggests a mechanical separation rather than vitreolysis, a term commonly used in recent literature. It can be implied that macular hole closure isa consequence of vitreofoveal traction release and not dependent on the contact of gas bubble to the posterior pole.
Despite this undemanding approach, two-thirds of the patients expected to undergo vitrectomy could avoid undergoing macular hole surgery. The final post-vitrectomy BCVA of one-third persistent FTMH was not statistically different from those which closed after the pneumatic procedure. On OCT, we found no association between the ellipsoid band and myoid band integrity with postoperative anatomical or functional outcomes. Admittedly, distant visual acuity is a poor indicator of macular function. Patient quality of life measures and microperimetry study along with analysis of outer retinal structures are likely to provide a more accurate structure-function correlation. Advantages of a pneumatic approach to stage 2 macular hole include simplicity of procedure, enhanced patient comfort, easy accessibility, relative inexpensiveness, and lack of unfavorable effect on the subsequent macular hole surgery. Furthermore, its relative non-invasiveness expands treatment indications for patients with very small FTMH and better BCVA, especially those unfit or unwilling for primary vitrectomy. The limitations of this study include its retrospective design, absence of control group, small number of patients and variable follow-up. Nevertheless, this is the first study to titrate the use and concentration of short- and long-acting gases in small-medium sized macular holes and obtain excellent visual and anatomical outcomes employing a simple, inexpensive, non-invasive procedure with minimal complications.
Declaration of Interests
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants, patents received or pending, or royalties.
References
-
Gass JD (1995) Reappraisal of biomicroscopic classification of stages of development of a macular hole. Am J Ophthalmol 119(2): 752-759.
-
Gaudric A, Haouchine B, Massin P, Paques M, Blain P, et al. (1999) Macular hole formation: new data provided by optical coherence tomography. JAMA Ophthalmology 117(6): 744-751.
-
Haouchine B, Massin P, Gaudric A (2001) Foveal pseudocyst as the first step in macular hole formation: a prospective study by optical coherence tomography. Ophthalmology 108(1): 15-22.
-
Duker JS, Kaiser PK, Binder S, Smet MDD, Gaudric A, et al. (2013) The International Vitreomacular Traction Study Group Classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology 120(12): 2611-2619.
-
Hikichi T, Yoshida A, Akiba J, Trempe CL (1995) Natural outcomes of stage 1, 2, 3, and 4 idiopathic macular holes. Br J Ophthalmol 79(6): 517-520.
-
Freeman WR, Azen SP, Kim JW, WE Haig, Mishell DR, et al. (1997) Vitrectomy for the treatment of full-thickness stage 3 or 4 macular holes: Results of a multicentered randomized clinical trial. The Vitrectomy for Treatment of Macular Hole Study Group. Arch Ophthalmol 115(1): 11-21.
-
Ezra E, Gregor ZJ, Morfields Macular Hole Study Ggroup Report No. 1 (2004) Surgery for idiopathic full-thickness macular hole: two-year results of a randomized clinical trial comparing natural history, vitrectomy, and vitrectomy plus autologous serum: Morfields Macular Hole Study Group RAeport no. 1. Arch Ophthalmol 122(2): 224-236.
-
Francisco S (2014) American Academy of Ophthalmology Retina/Vitreous Panel. American Academy of Ophthalmology, Preferred Practice Pattern® Guidelines: Idiopathic Macular Hole.
-
Banker AS, Freeman WR, Kim JW, Munguia D, Azen SP (1997) Vision-threatening complications of surgery for full-thickness macular holes: Vitrectomy for Macular Hole Study Group. Ophthalmology 104(9): 1442-1452.
-
Stalmans P, Benz MS, Gandorfer A, Kampik A, Girach A, et al. (2012) MIVI-TRUST Study Group: Enzymatic vitreolysis with ocriplasmin for vitreomacular traction and macular holes. N Engl J Med 367(7): 606-615.
-
Jackson TL, Haller J, Blot KH, Duchateau L, Lescrauwaet B (2021) Ocriplasmin for treatment of vitreomacular traction and macular hole: a systematic literature review and individual participant data meta-analysis of randomized, controlled, double-masked trials. Survey Ophthalmol 67(3): 697-711.
-
Chen X, Li M, You R, Wang W, Wang Y (2022) Efficacy and safety of Ocriplasmin use for vitreomacular adhesion and its predictive factors: A systematic review and meta- analysis. Front Med 8: 759311.
-
Steel DHW, Patton N, Stappler T, Karia N, Hoerauf H, et al. (2021) INJECT study investigators Ocriplasmin for vitreomacular traction in clinical practice: the INJECT study. Retina 41(2): 266-276.
-
Nefendorf JE, Kirthi V, Pringle E, Jackson TL (2017) Ocriplasmin for symptomatic vitreomacular adhesion. Cochrane Database of Syst Rev 10(10): CD011874.
-
Paul C, Muller HH, Raber T, Bertelmann T, on behalf of the EXPORT study group (2022) Calculating the individual probability of successful ocriplasmin treatment in eyes with vitreomacular traction-Validation and refinement of a multivariable prediction model. PLoS ONE 17: e0270120.
-
Chan CK, Wessels IF, Friedrichsen EJ (1995) Treatment of idiopathic macular holes by induced posterior vitreous detachment. Ophthalmology 102(5): 757- 767.
-
Jorge R, Costa RA, Cardillo JA, Uno F, Bonomo PP, et al. (2006) Optical coherence tomography evaluation of idiopathic macular hole treatment by gas-assisted posterior vitreous detachment. Am J Ophthalmol 142(5): 869-871.
-
Mori K, Saito S, Gehlbach PL, Yoneya S (2007) Treatment of stage 2 macular hole by intravitreous injection of expansile gas and induction of posterior vitreous detachment. Ophthalmology 114(1): 127-133.
-
Rodrigues IA, Stangos AN, McHugh DA, Jackson TL (2013) Intravitreal injection of expansile perfuoropropane (C3F8) for the treatment of vitreomacular traction. Am J Ophthalmol 155(2): 270-276.
-
Guber J, Rusch C, Guber I, Scholl PNH, Valmaggia C (2021) Indications and outcomes for intravitreal injection of C3F8 gas for symptomatic vitreomacular traction. Sci Rep 11: 18089.
-
Steinle NC, Dhoot DS, Ruiz CQ, Castellarin AA, Pieramici DJ, et al. (2017) Treatment of vitreomacular traction with intravitreal perfluoropropane (C3F8) injection. Retina 37(4): 643-665.
-
Baumann CE, Sabatino F, Zheng Y, Malek NJ, Maier M, et al. (2022) Anatomical and functional outcomes of pneumatic vitreolysis for the treatment of vitreomacular traction with and without macular holes. Graefe’s Arch Clin Exp Ophthalmol 260(7): 2209-2215.
-
Nefendorf JE, Simpson ARH, Steel DHW, Desai R, McHugh DA, et al. (2018) Intravitreal gas for symptomatic vitreomacular adhesion: a synthesis of the literature. Acta Ophthalmol 96(7): 685-691.
-
Chan CK, Mein CE, Glassman AR, Beaulieu WT, Calhoun CT, et al. (2021) Pneumatic vitreolysis with perfluoropropane for vitreomacular traction with and without macular hole: DRCR Retina Network Protocols AG and AH. Ophthalmology 128(11): 1592-1603.
-
Han R, Zhang C, Zhao X, Chen Y (2019) Treatment of primary full-thickness macular hole intravitreal injection of expansile gas. Eye 33(1): 136-143.
-
Cokl N, Petrovic MG (2018) Intravitreal injection of perfluoropropane is more efficacious than sulfur hexafluoride in releasing vitreomacular traction. Acta Clin Croat 57(2): 327-334.
-
Mehta N, Gupta L, Jansen M, Rosen R, Lee J (2020) Immediate release of vitreomacular traction after pneumatic vitreolysis followed by the drinking bird technique. Journal of Vitreo Retinal Diseases 4(4): 320- 324.
-
Fukumoto M, Sato T, Oosuka S, Kida T, Oku H, et al. (2020) Clinical features of vitreomacular traction syndrome with peripheral vitreoretinal adhesion. Clinical Ophthalmology 14: 281-286.
-
Yu G, Duguay J, Merra KV, Gautam S, Guern GL, et al. (2016) Efficacy and safety of treatment options for vitreomacular traction: A case series and meta-analysis. Retina 36(7): 1260-1270.
-
Johnson MW (2010) Posterior vitreous detachment: Evolution and complications of its early stages. Am J Ophthalmol 149(3): 371-382.
-
Hikichi T, Akiba J, Trempe CL (1993) Effect of the vitreous on the prognosis of full-thickness idiopathic macular hole. Am J Ophthalmol 116(3): 273-278.
-
Kishi S, Hagimura N, Shimizu K (1996) The role of the premacular liquefied pocket and premacular vitreous cortex in idiopathic macular hole development. Am J Ophthalmol 122(5): 622-628.
-
Johnson MW, Newkirk MRV, Meyer KA (2001) Perifoveal vitreous detachment is the primary pathogenic event in idiopathic macular hole formation. Arch Ophthalmol 119(2): 215-222.
-
Spaide RF, Wong D, Fisher Y, Goldbaum M (2002) Correlation of vitreous attachment and foveal deformation in early macular hole states. Am J Ophthalmol 133(2): 226-229.
-
Kim JW, Freeman WR, Haig WE, Maguire AM, Arevalo JF, et al. (1995) Baseline characteristics, natural history, and risk factors to progression in eyes with stage 2 macular holes. Results from a prospective randomized clinical trial. Vitrectomy for Macular Hole Study Group. Ophthalmology 102(12): 1818-1829.
-
Kim JW, Freeman WR, Azen SP, Haig WE, Klein DJ, et al. (1996) Prospective randomized trial of vitrectomy or observation for stage 2 macular holes. Vitrectomy for Macular Hole Study Group. Am J Ophthalmol 121(6): 605-614.
-
Tadayoni R, Svorenova I, Erginay A, Gaudric A, Massin P, et al. (2012) Decreased retinal sensitivity after internal limiting membrane peeling for macular hole surgery. Br J Ophthalmol 96(12): 1513-1516.
-
Gelman R, Stevenson W, Ponce CP, Agarwal D, Christoforidis JB (2015) Retinal damage induced by internal limiting membrane removal. J Ophthalmol 2015: 939748.
-
Chang JS, Smiddy WE (2014) Cost evaluation of surgical and pharmaceutical options in treatment for vitreomacular adhesions and macular holes. Ophthalmology 121(9): 1720-1726.
-
Gupta B, McHugh D (2011) Pneumatic retinopexy for the management of impending macular hole: an optical coherence tomography study. Int Ophthalmol 31(1): 23- 24.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report