Corneal Hysteresis in Adult Indian Population
Purpose: To evaluate corneal hysteresis (CH) and to study its inter-ocular variability along with its association with gender and age using Ocular Response Analyzer (ORA) among healthy adult Indian population. Methods: This prospective, cross-sectional, observational study was conducted at a tertiary eye care centre in a medical university in India between July and December 2020. 300 healthy participants in age group between 18 to 60 years were recruited from amongst the residents, staff and patients coming for routine examination in Ophthalmology department. Participants with history of systemic/ocular disease, ocular surgery, pregnancy or spherical equivalent refraction >±1D were excluded from study. CH and corneal compensated intra-ocular pressure (IOP-cc) was assessed using ORA. Statistical analysis was done to calculate mean CH in study population. Inter-ocular and gender-wise variability in mean CH was analysed using independent-t test. Pearson correlation coefficient was calculated to study correlation of CH between eyes and with age, gender, IOP-cc and central corneal thickness (CCT). Results: 162 males and 134 females were recruited. The mean age was 37.5±11 years and mean CH in overall study population, males and females were 10.57±1.12, 10.25±0.90, 10.96±1.22 mm Hg. No significant difference in CH, IOP-cc and CCT was observed between eyes. A strong positive correlation was observed in CH between eyes (r=0.75, p<0.001). Conclusions: Mean CH among healthy Indian adult is 10.57±1.12 mm Hg. CH values are higher among females compared to males. CH values between the two eyes in normal individuals are coherent and positively correlated.
Introduction
Cornea is a visco-elastic structure, thereby implying that it possesses both elastic and viscous properties [1]. With the introduction of Ocular response Analyzer (ORA), in vivo analysis of corneal biomechanical property has become almost a routine [2]. Over the last decade, corneal biomechanical properties like Corneal Hysteresis (CH) and Corneal Resistance Factor (CRF) have been increasingly studied in relation with various corneal Ectatic disorders and glaucoma [3, 4]. CH is defined as the ability of the corneal tissue to absorb and dissipate energy during a bidirectional application process [5]. Alike central corneal thickness (CCT), CH is also considered crucial for accurate assessment of intra-ocular pressure (IOP) [6]. Over the years, CH role has evolved from a factor affecting assessment of IOP to being a risk factor for Glaucoma [7, 8]. CH values obtained using ORA
were found to be repeatable in individual eyes of the same person but varied between individuals [9]. Studies from the past have indicated various ocular and demographic factors to affect CH [10]. Intra-ocular pressure, refractive error, gender, age, ocular surgeries and systemic illnesses like Diabetes Mellitus have been found to affect CH [11]. Low CH value is not only been linked but is now considered as a risk factor for developing Glaucoma and Keratoconus [2, 5].
However, there is no universal guideline to define a normal CH value. A recent meta- study assessing relationship between CH and glaucoma stated a CH of 11 mmHg in healthy eyes [3]. Various studies from different countries have stated different normal CH values in healthy adults ranging between 10.1 to 10.6mmHg [12, 13, 14]. The distribution of normal CH values has been found to differ not only between people in different parts of world but also between people belonging to different ethnic groups in a given geographical area. In United States, healthy African-Americans were found to have lower CH values compared to white Americans [7]. In absence of a universal normal CH value, it is important to determine its value among healthy adults in Indian context. To the best of our knowledge (PubMed search on 8 June, 2020), there is very limited data for CH in healthy Indian adults [15]. This study may serve as a reference database for normal CH values in healthy adults in India.
Methods
The study was conducted at a tertiary eye care center in a medical university in India. The study was conducted according to the tenets of declaration of Helsinki. Ethical committee clearance was obtained from the institutional Ethics Committee (ECR/262/Inst/UP/2013/RR-19). This was a prospective, cross-sectional, observational study conducted over a period of six months from July 2020 to December 2020. Healthy participants in the age group between 18 to 60 years were recruited in the study after obtaining their informed consent. The participants were recruited from amongst the employees of department including residents, optometrist and other staff. Participants were also recruited from patients and their attendants presenting to out-patient department for routine eye check- up. All the study participants were asked about the presence of any systemic or ocular illness, pregnancy and history of any previous eye surgery and only those with no such history were included. Any person with spherical equivalent of refraction (SER) > ±1D or non-cooperative for examination using ORA or with IOP outside the range of 10 to 21 mmHg was excluded from the study. The demographic profile of the participants was recorded. All study participants underwent complete ophthalmic evaluation including visual acuity assessment, anterior segment and fundus evaluation using 90D slit-lamp bio microscopy and refraction using auto refractometer. CCT was evaluated using non-contact pachymeter by CEM 530 (Nidek Inc., Aichi, Japan). Ocular Response Analyzer by G-3 (Reichert Inc., NY, USA) model was used to evaluate CH, Goldman-correlated IOP (IOPg) and Corneal-compensated IOP (IOP-cc). Corneal Resistance Factor (CRF) could not be measured due to lack of software in the present model.
Corneal Hysteresis was recorded for both eyes of every participant. A minimum of three CH values were recorded for each eye and only those values with reliability scores of 5 and above were recorded. The mean of the three values was considered for analysis from each eye. Average of the values of the two eyes of each participant was considered for studying CH relationship with age and gender. Inter-ocular and gender-wise variability in mean CH was analyzed using independent-t test. Pearson correlation coefficient was used to study any correlation between mean CH values and age, IOP-cc and CCT. Confidence interval of 95% was selected and a ‘p’ value of <0.05 was considered significant. The statistical analysis was done using statistical package for social sciences software version 21.
Sample Size: Using the formula n=z2σ2/d2 for estimating the mean in a population and using a confidence coefficient of 0.95 (z=1.96), an estimated standard deviation of 2.5 units (σ= 2.5) in CH based on previous studies and a desired width of confidence interval as 0.4 (d=0.2) a sample size of 600 eyes was derived.
Results
Out of total of 300 (600 eyes) participants, 162 (54%) males and 138 (46%) females were recruited. The mean age of the study population was 37.5 (± 11.6) years (range: 18-60 years). The mean CH and CCT of the sample were 10.57(± 1.12) mm Hg and 539.08 (±24.17) mm respectively. Males were found to have lower corneal hysteresis 10.25(±0.90) mm Hg compared to females 10.96(±1.22) mm Hg (p<0.00). The mean corneal compensated IOP (IOP- cc) among males 15.38(±2.2) mm Hg was higher compared to females 14.55(±2.12) mm Hg (p<0.00). Females also had higher mean CCT compared to males; however, this was not statistically significant (p=0.42). There was no statistically significant inter-ocular difference in IOPcc, CH or CCT. Inter- eye comparison also revealed a statistically significant and strong positive correlation in corneal hysteresis between eyes (r=0.76, p<0.00) (Figure 1). There was weak but statistically significant negative correlation between corneal hysteresis with age (r=-0.23, p<0.001) (Figure 2) and IOP-cc (r=-0.24, p<0.001) whereas a weak positive but statistically significant correlation between age and IOP-cc (r=0.16, p=.004).
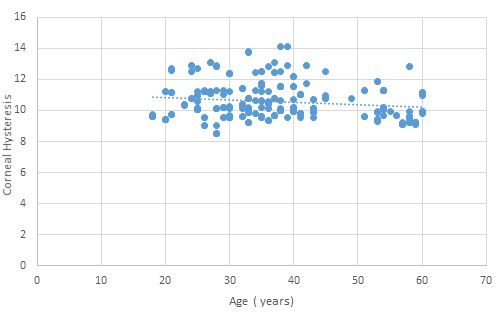
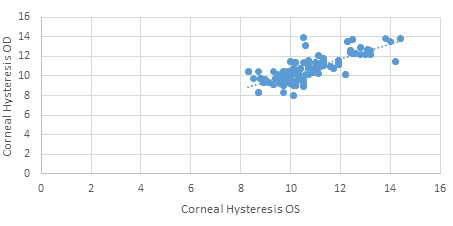
A weak positive correlation was also seen between CH and CCT, but this was statistically insignificant (r=0.10, p=0.08). Details of study results are summarized in the Tables 1-4.
| Frequency (Percentage) | Mean ±SD | Range | |
|---|---|---|---|
| Age | - | 37.5 ± 11.6 years | 18-60 years |
| Females | 138 (46%) | 36 ± 10 years | 20-60 years |
| Males | 162 (54%) | 38 ± 12 years | 18-60 years |
| Corneal Hysteresis (CH) | 600 eyes | 10.57 ± 1.12 mm Hg | 8.30-14.4 mm Hg |
| Central Corneal Thickness (CCT) | 600 eyes | 539.08 ± 24.17 µm | 483-612 µm |
| Corneal Compensated IOP (IOP-cc) | 600 eyes | 15 ± 2.22 mm Hg | 10-20 mm Hg |
| Males( n =162) | Females (n=138) | P- value | |
| Mean Age( ± SD)* | 38 ( ± 12) | 36 (± 10) | 0.118 |
| Mean CH (+ SD)** | 10.25 ( ± 0.90) | 10.96 (± 1.22) | <0.001 |
| Mean IOP cc ( + SD)** | 15.38 ( ± 2.2) | 14.55 (± 2.12) | <0.001 |
| Mean CCT (±SD)*** | 538.04 (±25.75) | 540.31 (±22.21) | 0.419 |
Table 1: Demographic and clinical profile of the study participants.
| Right Eye | Left Eye | P-value | |
|---|---|---|---|
| Mean CH (±SD)* | 10.58 ( ± 1.18) | 10.57 ( ± 1.20) | 0.82 |
| Mean IOP cc (± SD)* | 15.10 ( ± 2.48) | 14.91 ( ± 2.33) | 0.96 |
| Mean CCT (±SD)** | 537.36 (± 25.02) | 540.88 (±24.07) | 0.079 |
Table 2: Inter-ocular variability in corneal hysteresis (CH), corneal compensated intra-ocular pressure (IOP-cc) & central cornea
| Clinical Parameter | ‘R’ value (Pearson Coefficient) | P-value |
|---|---|---|
| Age | -0.23 | <0.001 |
| IOP-cc* | -0.24 | <0.001 |
| CCT** | 0.1 | 0.08 |
| Contralateral CH*** | 0.76 | <0.001 |
Table 3: Correlation of corneal hysteresis with other clinical parameters. *Corneal compensated intra-ocular pressure **Central c
Discussion
With increasing evidence of role of reduced CH in pathogenesis of glaucoma and corneal ectatic disorders, it is imperative to have a reference for normal CH values [3, 4]. We have evaluated 600 eyes of 300 healthy adults, making this one of the largest studies from India for evaluating CH (PubMed search). The mean CH of participants in this study was 10.57 ±1.12 mm Hg which is lower than observed in Caucasian, Egyptian, Arabian and Brazilian populations [12, 16, 17, 18]. It was comparable to Chinese and Americans whereas was greater than Japanese and African populations [9, 11, 13, 14, 19]. Varied ethnic and genetic differences among populations may explain this variation as has been observed with varied trabecular meshwork height, CCT and facial anthropology [20, 21]. Differences in the gender ratio, mean age and refractive status of participants between studies may also explain varied CH values. Thus, with such variation in values, our study provides the Indian standard for normal CH. There was a statistically significant difference in CH and IOP-cc values between males and females. Females had higher CH consistent with other studies [16, 22]. Though uncertain, hormonal differences between sexes could affect the corneal biomechanics. In a recent study on porcine cornea, estrogen had relaxing effect on cornea reducing its stiffness [23]. In our study, CCT among females was also higher though statistically insignificant. This may also explain higher CH among them.
It has been proposed that thicker corneas may have higher pressure dampening ability and thus exhibit greater hysteresis [2, 5, 10]. A study comparing CH between American Blacks and White stated 2.14 mm Hg rise in CH with every 100 µm increase in CCT [9]. In our study, a weak positive correlation was observed between CH and CCT. In accordance with other studies we also observed a small yet statistically significant negative correlation between CH and IOP-cc [5, 9, 14]. A lower IOP-cc among females could also be attributed to higher CH among them in our study. We observed a weak negative yet statistically significant correlation between CH and age. Ageing is known to alter corneal structure and in turn affect corneal biomechanics [24]. Various studies from the past have shown reduction in CH and rise in IOP with age [25, 26, 27]. A weak positive correlation between age and IOP-cc has also been observed in our study. The mean CH value reported in present study is higher compared to another Indian study on relationship of corneal biomechanics and IOP with spectrum of glaucoma [15]. A relatively young cohort in our study (Mean Age 37.5 year’s vs. 51.9 years) may be the reason for us observing higher CH. Another finding of our study has been lack of any statistically significant difference in CH between eyes in individuals. Furthermore, there was strong positive and significant correlation in CH between eyes. Unilateral
pterygium and anisometropic high myopes have been reported to present with asymmetric CH [28, 29]. We have in our study found that, low but bilaterally similar CH may be observed even in normal eyes. This lack of interocular variability in CH was also reported in another Indian study [15]. Rather than only reduced CH, subsequent studies may confirm bilateral asymmetry in CH as abnormal. One of the main limitations of our study was not considering corneal resistance factor (CRF) while studying CH. This was because of lack of the required technology for assessing CRF. Though CRF and CH have been correlated, clinical utility of CH alone has been extensively documented [4, 11, 12].
Another limitation in our study has been a limited sample size. In spite of being one of the largest studies from India, a larger sample would have given better estimates on CH. Furthermore, it would have allowed us to perform age wise analysis of CH data and provide normative data according to age. We found certain healthy individuals with low CH values in our study. It would be interesting to see if these individuals end up on developing any corneal abnormalities or glaucoma later in life. A longitudinal study in future may be planned in among healthy individuals with low CH scores to study if low CH scores in apparently healthy individuals can predispose them to glaucoma or corneal ectatic disorder later in life.
Conclusion
Mean CH of healthy Indian adults is 10.57±1.12 mm Hg. CH values are higher among females (10.96±1.22 mm Hg) compared to males (10.25±0.90 mm Hg). A positive correlation is present between CH and CCT whereas CH is negatively correlated with age and IOP-cc. CH values between eyes in normal individuals are coherent and positively correlated.
Declaration of Interest
We wish to confirm that there are no known conflicts of interest associated with this publication that could have influenced its outcome.
Funding
We also declare that there has been no financial support for this work that could have influenced its outcome.
References
-
Kobayashi AS, Staberg LG, Schlegel WA (1973) Viscoelastic properties of human cornea. Exp Mech 13: 497-503.
-
Luce DA (2005) Determining in vivo biomechanical properties of the cornea with an ocular response analyzer. J Cataract Refract Surg 31(1): 156‐162.
-
Shah S, Laiquzzaman M, Bhojwani R, Mantry S, Cunliffe I (2007) Assessment of the biomechanical properties of the cornea with the ocular response analyzer in normal and keratoconic eyes. Invest Ophthalmol Vis Sci 48(7): 3026‐3031.
-
Liang L, Zhang R, He LY (2019) Corneal hysteresis and glaucoma. Int Ophthalmol 39(8): 1909‐1916.
-
Kaushik S, Pandav SS (2012) Ocular Response Analyzer. J Curr Glaucoma Pract 6(1): 17‐19.
-
Franco S, Lira M (2009) Biomechanical properties of the cornea measured by the Ocular Response Analyzer and their association with intraocular pressure and the central corneal curvature. Clin Exp Optom 92(6): 469‐475.
-
Wells AP, Heath DFG, Poostchi A, Wong T, Chan KC, et al. (2008) Corneal hysteresis but not corneal thickness correlates with optic nerve surface compliance in glaucoma patients. Invest Ophthalmol Vis Sci 49(8): 3262‐3268.
-
Dulac AG, Saad A, Abitbol O, Febbraro JL, Azan E, et al. (2012) Assessment of corneal biomechanical properties in normal tension glaucoma and comparison with open- angle glaucoma, ocular hypertension, and normal eyes. J Glaucoma 21(7): 486‐489.
-
Montanes JM, Maldonado MJ, Garcia N, Mendiluce L, Gomez PJG, et al. (2008) Reproducibility and clinical relevance of the ocular response analyzer in nonoperated eyes: corneal biomechanical and tonometric implications. Invest Ophthalmol Vis Sci 49(3): 968‐974.
-
Leite MT, Alencar LM, Gore C, Weinreb RN, Pamela A, et al. Comparison of corneal biomechanical properties between healthy blacks and whites using the Ocular Response Analyzer. Am J Ophthalmol 150(2): 163‐168.
-
Porta NG, Fernandes P, Queiros A, Borges JS, Mato MP, et al. (2014) Corneal biomechanical properties in different ocular conditions and new measurement techniques. ISRN Ophthalmol 2014: 724546.
-
Kamiya K, Hagishima M, Fujimura F, Shimizu K (2008) Factors affecting corneal hysteresis in normal eyes. Graefes Arch Clin Exp Ophthalmol 246(10): 1491‐1494.
-
Fontes BM, Ambrosio R, Alonso RS, Jardim D, Velarde GC, et al. (2008) Corneal biomechanical metrics in eyes with refraction of -19.00 to +9.00 D in healthy Brazilian patients. J Refract Surg 24(9): 941‐945.
-
Narayanaswamy A, Chung RS, Wu RY, Park J, Wong WL, et al. (2011) Determinants of corneal biomechanical properties in an adult Chinese population. Ophthalmology 118(7): 1253‐1259.
-
Kaushik S, Pandav SS, Banger A, Aggarwal K, Gupta A (2012) Relationship between corneal biomechanical properties, central corneal thickness, and intraocular pressure across the spectrum of glaucoma. Am J Ophthalmol 153(5): 840‐849.
-
Morel MD, Jamart J, Hautenauven F, Pourjavan S (2012) Comparison of the corneal biomechanical properties with the Ocular Response Analyzer® (ORA) in African and Caucasian normal subjects and patients with glaucoma. Acta Ophthalmol 90(2): e118‐e124.
-
Ali AA (2017) Corneal hysteresis values in normal Egyptian population. Kasr Al Ainy Med J 23(1): 38-42.
-
Arfaj KA, Yassin SA, Dairi WA, Shamlan FA, Jindan MA (2016) Corneal biomechanics in normal Saudi individuals. Saudi J Ophthalmol 30(3): 180‐184.
-
Chua J, Nongpiur ME, Zhao W, Yih Tham C, Gupta P, et al. (2017) Comparison of Corneal Biomechanical Properties between Indian and Chinese Adults. Ophthalmology 124(9): 1271‐1279.
-
Chen RI, Barbosa DT, Hsu CH, Porco TC, Lin SC (2015) Ethnic differences in trabecular meshwork height by optical coherence tomography. JAMA Ophthalmol 133(4): 437‐441.
-
Farkas LG, Katic MJ, Forrest CR, Alt KW, Bagic I, et al. (2005) International anthropometric study of facial morphology in various ethnic groups/races. J Craniofac Surg 16(4): 615‐646.
-
Allam RS, Khalil NM (2015) Evaluation of sex differences in corneal hysteresis. Eur J Ophthalmol 25(5): 391‐395.
-
Walter E, Kormas RM, Marcovich AL, Lior Y, Sui X, et al. (2019) The effect of estrogen and progesterone on porcine corneal biomechanical properties. Graefes Arch Clin Exp Ophthalmol 257(12): 2691‐2695.
-
Daxer A, Misof K, Grabner B, Ettl A, Fratzl P (1998) Collagen fibrils in the human corneal stroma: structure and aging. Invest Ophthalmol Vis Sci 39(3): 644‐648.
-
Hashemi H, Kashi AH, Fotouhi A, Mohammad K (2005) Distribution of intraocular pressure in healthy Iranian individuals: the Tehran Eye Study. Br J Ophthalmol 89(6): 652‐657.
-
Kotecha A, Elsheikh A, Roberts CR, Zhu H, Heath DFG (2006) Corneal thickness- and age-related biomechanical properties of the cornea measured with the ocular response analyzer. Invest Ophthalmol Vis Sci 47(12): 5337‐5347.
-
Kamiya K, Shimizu K, Ohmoto F (2009) Effect of aging on corneal biomechanical parameters using the ocular response analyzer. J Refract Surg 25(10): 888‐893.
-
Vanathi M, Goel S, Ganger A, Agarwal T, Dada T, et al. (2018) Corneal tomography and biomechanics in primary pterygium. Int Ophthalmol 38(2): 663‐671.
-
Xu S, Xu A, Tao A, Wang J, Fan F, et al. (2010) Corneal biomechanical properties and intraocular pressure in high myopic anisometropia. Eye Contact Lens 36(4): 204-209.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report