Retinal Arterial Macroaneurysm: Report of 3 Cases
Purpose: To report a clinical analysis of three cases of Retinal Macroaneurysm with their systemic involvement. Method: An observational case series of three cases of Retinal Arterial Macroanerysm (RAM) presented at Chittagong Eye Infirmary & Training Complex (CEITC). Detail history of systemic and ocular disease, thorough clinical examination, best corrected visual acuity, slit lamp biomicroscopy, indirect ophthalmoscopy, Fundus Fluorescein Angiography (FFA), Optical Coherence Tomography (OCT) scan were performed according to the cases. Diagnosis was made by ocular findings and appropriate ancillary tests. An internet search (medline search) and review of current literature on Retinal Arterial Macroanerysm were done and information relevant to our objectives was obtained. Result: Three patients presented with blurring of vision in affected eye. All of them were female & at or above sixty years of age. Three affected eyes of three patients were analyzed. Vision on presentation 6/60 or worse in affected eyes in all cases. Their anterior segment showed no abnormality. Fundus showed more than one RAM along upper temporal arcade of left eye in 1st patient, 2nd patient showed single RAM at macula along upper temporal arcade of right eye, 3rd one showed a round RAM surrounded with haemorrhage & exudates on macula along lower temporal arcade of right eye . Fundus fluorescin angiogram (FFA) revealed in all three patients hyper & hypo fluorescein at macular and surrounding area due to RAM and associated intra retinal haemorrhage and exudates. Opitcal Coherance Tomograhy (OCT) done in first 2 cases after laser therapy showed normal foveal thickening. Second case gets intravitreal injection avastin in addition to laser. After laser treatment first case showed visual improvement from counting finger ( CF) to 6/12, third case also showed improvement from 6/60 to 6/9 though short follow up, but second case showed visual deterioration fron 6/60 to counting finger with all the treatment. Conclusion: Though Retinal Macro anerysm is a rare disease but it can cause loss of vision due to foveal involvement. Proper and in time intervention may rescue the vision
Introduction
Retinal Macroaneurysm have been observed since 1808, In 1973 Robertson first described RAM with its characteristic features [1, 2, 3, 4]. RAMs are acquired disease [3].
Retinal arterial macroaneurysms (RAM) may be defined as fusiform (cuffed’) or saccular (‘blow-out’) dilatations of the retinal arteries, usually arising within the first three orders of retinal artery bifurcation [1, 2, 3, 4, 5]. The supratemporal artery is most commonly affected because patients with such involvement are more likely to have visual impairment [2]. In most reported cases RAM are unilateral and single, while 10% may be bilateral2 as well as some report noted multiple macroaneurysms [2]. Majority of reported cases showed female predominance [2, 5]. Commonly RAM occur at sixth and seventh decades of life [2, 5]. RAMs are strongly associated with systemic hypertension and atherosclerosis in approximately 75% of patients [1, 2, 3, 4, 5].Retinal arteriolar RAMs may be asymptomatic, if the macula is not involved. Deterioration of central vision occur as a result of macular edema, exudation or haemorrhage [2, 3, 4, 5, 6].
Natural history may lead to a spontaneous resolution of the lesion, but also have a number of vision- threatening complications, including subretinal, preretinal or vitreous haemorrhages, macular oedema, serous macular detachment, macular deposition of hard exudates, macular hole and branch retinal vein occlusion [3, 4, 5, 6].
Treatment is indicated when RAMs causing exudative manifestations or haemorrhage involving the fovea. Treatment of RAMs is still controversial [4, 5, 6]. Mostly threshold laser photocoagulation is carried out in an attempt to achieve the obliteration of the vascular lesion. Several studies evaluated laser treatment for exudative RAMs with 4 months of follow-up and showed that it improved visual acuity and central foveal thickness [3, 4].
Nevertheless, several complications have been related to direct threshold laser treatment (TLT) [3, 4, 5, 6]. So subthreshold laser treatment (STLT) has been proposed in an attempt to minimise the adverse aspects of conventional laser photocoagulation [4, 5, 6].
Recently, intravitreal injections of anti–vascular endo- thelial growth factor (VEGF) drugs have been considered as a treatment option for RAMs [6]. In this report we analyse three patients with RAMs who were followed up for period ranging from four months to four years. All three patients presented with dimness of vision due to chronic decompensation due to an exudative response.
Case Reports
Case I
A 60 years old female presented to Retina Clinic, CEITC on 04-01-09 with complaints of gradual painless dimness of vision in left eye for 2 years. Patient was hypertensive but non diabetic and no history of ocular trauma or other systemic disease.
On examination, her BCVA (Best Corrected Visual Acuity) was 6/9 in right eye and CF (Counting Finger) in left eye. Anterior segment was normal except bilateral immature cataract. Intra Ocular Pressure (GAT) 14 mmHg in both eyes.
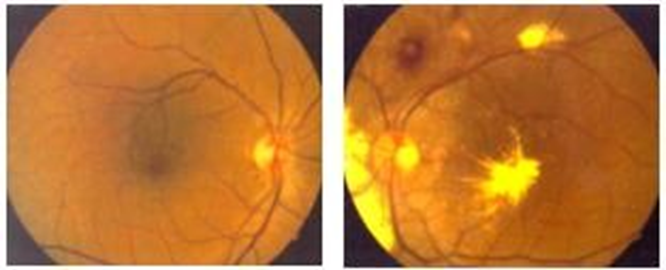
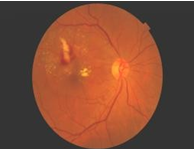
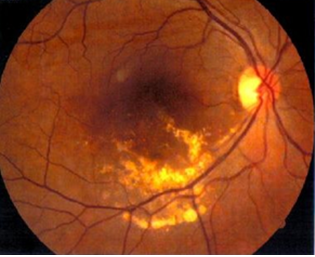
Fundoscopy revealed normal findings in right retina, left retina showed two macroaneurysms, one located one disc diameter above the optic disc with retinal haemorrhage around it, another located within the macula and extensive deposition of hard exudates in the fovea , above the upper arcade and on nasal retina (Figure 1).
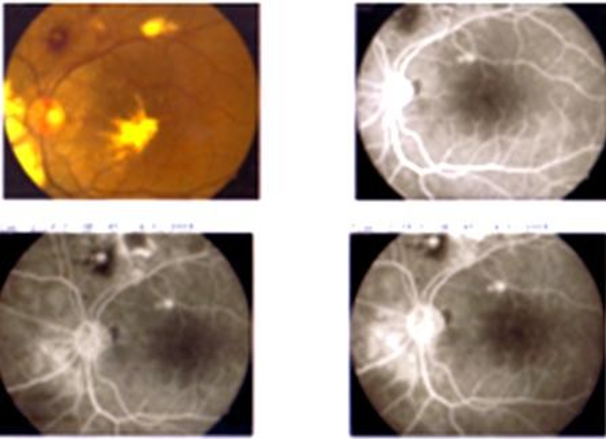
FFA of left eye showed two round hyperfluorescin spot representing the RAMs more clearly (Figure 2). Her Blood Pressure was 160/100 mm of Hg. Her lipid profile was, Serum Cholesterol: 161 mg /dl, Serum Triglyceride: 105 mg/ dl, Serum HDL: 34.0 mg/dl, Serum LDL: 108.0 mg/dl, Serum Urea: 19 mg/dl, Serum Creatinine: 0.9 mg/dl. Her Fasting Blood Sugar was 100 mmol /l and Corresponding Urine Sugar was nil.
So our probable diagnosis was Right Eye within Normal Limit and Left Eye Retinal Arterial Macroaneurysm with exudative features.
We applied Threshold Laser Treatment (TLT) directly to macroaneurysms as well as Subthreshold Laser Treatment (STLT) to surrounding retina of the left eye on 21-01-09.
One month post laser treatment on 25-02-09, her BCVA was 6/9 in right eye and was 6/60 in left eye. Her IOP (GAT) was 12 mmHg in right eye and 14 mmHg in left eye. Fundoscopy revealed reduction of macular oedema and hard exudates in left eye (Figure 3).
On 23-01-11, 2 years later her BCVA 6/9 in right eye and 6/18 in left eye. IOP (GAT) 14 mmHg in right 16 mmHg in left eye. Anterior segment reaveled normal.Left retina showed minimum residual hard exudates with laser scar (Figure 4). FFA showed no fluorescin dye leakage only staining of laser scars (Figure 4).
Optical coherence tomography (OCT) of left eye at the end of follow-up showed normal foveal thickness with no accumulation of fluid. (Figure 5) OCT showed 253 micro meter central subfoveal thickness in left eye.
Case II
A 60 yrs old female presented to Retina Clinic, CEITC on 19-05-10 with complaints of gradual painless, loss of vision in right eye for 2 years. Patient was diabetic and hypertensive for sixteen years. No history of ocular trauma nor other systemic disease. Her Blood Pressure was 130/100 mm of Hg. She was disbetic for 16 years. On examination her BCVA was 6/60 in right eye and was 6/18 in left eye. Anterior segment was normal except immature cataract in both eyes. IOP (GAT) 14 mmHg in both eyes.
Fundoscopy revealed, right RAM, surrounded with retinal haemorrhage and hard exudates, RAM located near the fovea with huge foveal oedema, left fundus showed mild NPDR.
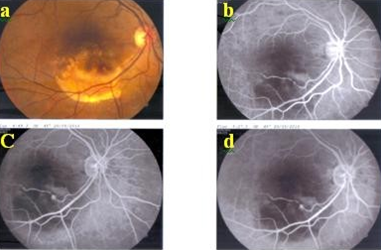
The patient was diagnosed as right eye RAM with macula oedema and bilateral mild NPDR (Non proliferative retinopathy) Direct Laser and Inidrect laser was performed for treat the RAM. But after one month response to laser treatment was poor, there was much more macular oedema with huge accumulation of hard exudate (Figure 6).
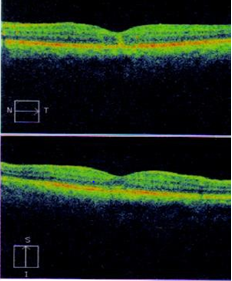
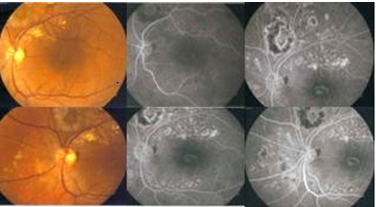
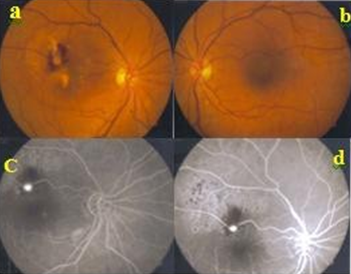
Figure 6: a,b) Color Fundus Photos both eyes after laser therapy, right fundus showed macroaneurysms,surrounded with retinal haemorrhage and hard exudates located near the fovea, left fundus normal. c,d) The fluorescein angiogram showed hyperfluorescence that corresponds to the retinal macroaneurysm, did not respond well to laser and the hypo fluorescence that corresponds to the retinal haemorrhage.
The FFA after 1 month of laser, revealed both hyperfluorescence and hypofluorescence. Hyper fluorescence corresponds to the retinal macroaneurysm and the hypofluorescence corresponds to the retinal hemorrhage (Figure 6). At this point we decided to go for intravitreal injection Avastin (Bivacizumab) 1.25mg in 0.05ml three doses at two months apart.
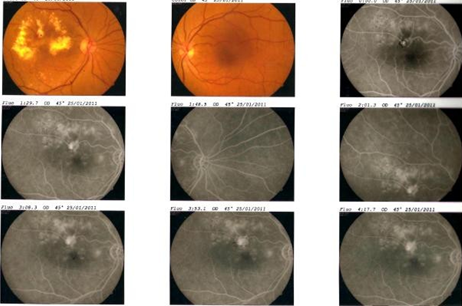
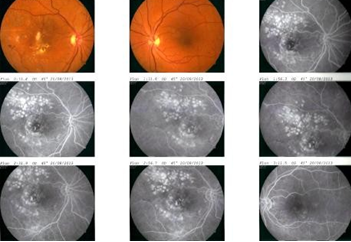
One month after completion of injection on 8th December 2010, her BCVA right eye was CF 2 ft. and was 6/9 in left eye. Anterior segment revealed normal .Right fundus showed fibrosed RAM with reduction of retinal haemorrhage and macular oedema but appearance of new hard exudate and mild NPDR in both eye (Figure 7).
After two months, of completion of injection and post laser, on 25th January 2011, her BCVA in both eyes remain as before,right eye was CF 2 ft. and 6/9 in left eye Right fundus revealed fibrosis of RAM, laser scar and huge hard exudate.
Mild NPDR in both eyes. FFA right eye showed no leakage only window defect corresponds to RPE atrophy and staining of laser scar (Figure 8).
Patient was lost from follow up but after one year on 28th march 2012, she came back with similar stable vision that was BCVA right eye was CF 2 ft. and 6/9 in left eye. Anterior segment revealed no abnormalities.Right Fundus showed fibrosed RAM with scar.and it was surrounded by a large ring of hard exudate (Figure 9) and mild NPDR was detected in both eye.OCT showed no accumulation of fluid and 270 micro meter central subfoveal thickness Figure 9. So we did not go for further intervension.
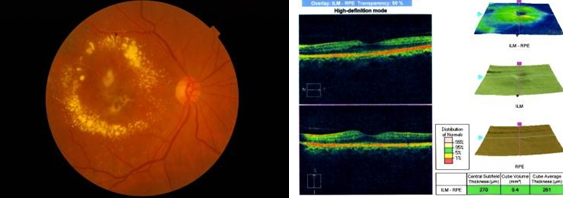
Figure 9: Fibrosed RAM centred in aflorid circinate ring of exudate extending remotely from the aneurysm to reach the macular area. OCT right macula showed no fluid accumulation and central subfoveal thickness 270 micro meter. After one and half year at last visit on 20th August, 2013, her BCVA remain stable, right BCVA was CF 2 ft. and left eye BCVA was 6/9. Anterior segment remain normal as before. Right retina showed fibrosed RAM with reduced hard exudate with resolved macular oedema, mild NPDR both eyes. FFA showed no leakage in all the phages of angiogram that ment there was no sign of activation, there was only RPE defect and scar staining (Figure 10).
Case III
A 65 year’s old female presented to Retina Clinic, CEITC on 18-05-10 with complaints of gradual painless dimness of vision in righr eye for 3 months. Patient was hypertensive but non diabetic. She did not give any history of ocular trauma nor other systemic disease. On examination her BCVA was 6/60 in right eye and was 6/9 in left eye. Anterior segment was normal except immature cataract in both eyes. Posterior segment examination revealed a fusiform RAM along the inferior arcade, the RAM surrounded with huge hard exudates.There was diffuse macular oedema (Figure 11).
FFA detected a fusiform hyper fluorescent lesion correspond to RAM along inferior arcade, and block choroidal corresponds to hard exudates. Figure 11 IOP (GAT) 14 mm Hg in both eyes.
This was diagnosed as a case of right RAM with exudative features. Direct and indirect laser photocoagulation was done on RAM of right eye.
One month after laser on last followup at 27th July 2010 her BCVA was 6/9 in both eyes. Anterior segment was normal as before except mild immature cataract in both eyes. Fundus examination revealed obliteration of RAM with marked reduction of hard exudates along the inferior arcade. There was resolution of macular oedema (Figure 12).
She was asked for review after six months. But patient was lost from follow up.
Discussion
Retinal arterial macroaneurysms (RAM) may be defined as fusiform or saccular dilatations of the retinal arteries, usually arising within the first three orders of bifurcation and at AV crossings [1, 2, 3, 4, 5]. The most common involvement is along the superotemporal or inferotemporal arcades, with the nasal vessels more rarely involved. Macroaneurysm have also been reported in cilioretinal arteries and on the optic nerve head1. The diameter of macroaneurysm is 100 to 250 micron3. Our first and second case had RAM along the superotemporal arcade and third case showed RAM along inferotemporal arcades (Table 1).
| Patient No | Age | Sex | Systemic History | Retinal Artery Involved | BCVA | Treatment Given | Follow Up Period | |
|---|---|---|---|---|---|---|---|---|
| 1 | 60 | F | HTN | Lt ST | Counting finger | 06-Dec | Green laser photocoaulation | 4 Year |
| 2 | 60 | F | HTN+DM | Rt ST | Jun-60 | Counting finger | Green laser photocoagultion+ Iv Injection Avastin | 3 Year |
| 3 | 65 | F | HTN | Rt IT | Jun-60 | 06-Sep | Green laser photocoaulation | 4 month’s |
Table1: Demographic and clinical profile of three patients. HTN-Hypertension DM- Diabetes Malitus, ST- Superior Temporal IT- Inferior Temporal. BCVA- Best corrected visual acuity.
RAMs are associated with exudation and hemorrhage, which may result in decreased visual acuity if it involves the central macula. In all three of our cases, RAM predominantly associated with exudation not haemorrhage involves the central macula.All of them came with huge deterioration of vision (Table-1).
Several series have reported on the natural history and treatment response of macroaneurysms [1, 2, 3] Approximately 10 % of macroaneurysms are pulsatile on initial presentation. (can be a sign of impending rupture). Formation of retinal macroaneurysms is associated with systemic hypertension and atherosclerotic disease, serum lipid abnormalities. Some author postulate that person have focal arterial wall atheroma occurring at defects in the wall, which may be at risk sites of aneurysm formation. After acute hemorrhage, there may be spontaneous thrombosis and closure of the aneurysm lead to resolution of the condition; in some cases, the artery may return to normal [2]. Older woman (Female : male-3:1), usually greater than 60 yrs of age with established history of systemic hypertension are mostly affected [1, 2, 3, 4] Our all three cases were female. Two of the cases were 60 years old and third one was 65 years old. All of them had history of hypertension and second one had diabetes also (Table-1).
The vision threating complications are cystoid macular edema, diffuse /focal macular edema, hemorrhage at different layers like sub retinal pigment epithelial (RPE) hemorrhage sub internal limiting membrane (ilm) and vitreous hemorrhage,secondary epiretinal membrane, serous retinal detachment,macular lipid exudation, branch retinal vein occlusion [3, 4]. The visual prognosis is good in cases presenting with bleeding, poor in those presenting with macular edema, exudation or hemorrhage leading to damage of photoreceptor and scarring [1, 2]. All three cases of this report presented with reduced vision and RAMs with macular oedema and exudate.
The Differential Diagnosis are - Exudative age- related macularm, degeneration(AMD), Branch retinal vein occlusion, Diabetic macular edema, Choroidal melanoma, Diabetic retinopathy, Retinal telangiectasis, Leber’s miliary aneurysms, Von Hippel’s angiomatosis, Capillary hemangioma, Cavernous hemangioma, Radiation retinopathy.
Fluorescein angiography is particularly important in making the diagnosis when there is hemorrhage (which obscures the vasculature). Late fluorescein leakage from within the areas of hemorrhage is characteristic of the aneurysms and may assist in the diagnosis when the vasculature is not visible on direct exam.
A quiet macroaneurysm that is asymptomatic without visible leakage should not be treated, monitored until spontaneous fibrosis occurs. Aneurysms that leak fluid or exudate, or both, and threaten to involve or already involve the central macula may be considered for therapy [4, 5]. Because, the long-term persistence of exudative manifestations or hemorrhages leads to a progressive photoreceptor damage with functional impairment [3, 5]. So in case of indication, early treatment may be desirable in attempting to avoid irreversible structural and functional damage [2, 3, 4, 5].
But there is no clear indication for treatment with laser photocoagulation has been established, and the beneficial effects of such treatments have not been proven [2].
The best approach to treat RAMs is still a matter of controversy and at present there is no general consensus about the optimum approach [1, 2, 3, 4]. The most commonly employed approach is conventional threshold laser treatment (TLT) [1, 2, 3, 5]. In TLT there is direct treatment of the aneurysm with moderately heavy argon green or yellow dye laser with large spot size (500 m) and long duration (0.5 s). But this technique has many complications, like enlargement of the laser scar, and scarring with possible retinal traction, choroidal neovascularization, and subretinal fibrosis, branch retinal artery occlusion, increased retinal exudation have been reported [3, 4, 5].
So recently some author employed indirect laser photocoagulation with Subthreshold Laser Treatment (STLT) to surrounding retina around RAM [3, 4, 5]. STLT may lead to an improved balance in cytokines release,perhaps including an up regulation of basic fibroblast growth factor, thus, STLT may act on the complex interaction among the different molecules implicated in the vascular permeability,promoting a vascular repair together with an improved fluid reabsorption.4 Subthreshold laser treatment (STLT) was reported to be effective in achieving the cessation of leakage, Associated with functional improvement [3]. In M N Abdel-Khalek et al. 1 series of 10 treated eyes two showed improvement in visual acuity. Seven eyes showed no alteration in vision.They1 treated RAM directly either with xenon arc or laser and did not observed any untoward sequelae. Direct treatment speeds the rate of absorption of perianeurysmal exudates and seals the RAMs itself1. The question of direct or indirect treatment of RAMs, however, remains controversial [1, 3, 4]. Recently, several case reports have shown encouraging results of intravitreal anti-VEGF agents for retinal arterial macroaneurysms [5, 6]. It reduces the vascular permiability and act on coagulation cascade ,thus it promote obliteration of RAM and absotption of fluid and exudates.
In our cases we used both TLT and SLT. In 2nd case we also gave additional anti VEGF injection (Bivacijumab). Our 1st and 3rd case showed visual improvement and 2nd case showed visual deterioration.1st case visual improvement from counting finger to 6/12 snellen chart (Table 1). 3rd case showed improvement from 6/60 to 6/9 Snellen chart. 3rd case could not regain vision may be due to late presentation and RAM located near to fovea.
Conclusion
RAMs are probably commoner than is realised. They may confront the ophthalmologist in one of two ways: (1) sudden loss of vision due to rupture of RAMs causing haemorrhage that obstract the vision: (2) grdual loss of vision due to macular oedema and hard exudate.
Acknowledgement
We acknowledge with thanks the expert and industrious help of Mr Michael Strachan, medical photographer, Mohammad Shamsal Islam, Research officer, (Dr. Ahmadur Rahman Research Centre, ICO, CU) and the following consultants who were kind enough to refer cases:.
References
-
Abdel-Khalek MN, Richardson J (1986) Retinal macroaneurysm: natural history and guidelines for treatment Br. J Ophthalmol 70(1): 2-11.
-
Emily YC, Murphy RP (2006) Retinal Vascular Disease: Acquired Retinal Macroaneurysms. Medical Retina, 17th (Edn.), Merck Research Labora-tories, Whitehouse Station (NJ), Section 2.
-
Parodi MB, Iacono P, Pierro L, Papayannis A, Kontadakis S, et al. (2012) Subthreshold laser treatment versus threshold laser treatment for symptomatic retinal arterial macroaneurysm. Invest Ophthalmol Vis Sci 53(4): 1783-1786.
-
Parodi MB, Iacono P, Ravalico G, Bandello F (2011) Subthreshold laser treatment for retinal arterial macroaneurysm. Br J Ophthalmol 95(4): 534-538.
-
Cho HJ, Rhee TK, Kim HS, Han JI, Lee D, et al. (2013) Intravitreal Bevacizumab for Symptomatic Retinal Arterial Macroaneurysm. Am J Ophthalmol 155(5): 898-
-
Pichi F, Morara M, Torrazza C, Manzi G, Alkabes M, et al. (2013) Intravitreal Bevacizumab for Macular Complications From Retinal Arterial Macroaneurysms. Am J Ophthalmol February 155(2): 35-43.
-
Nadel AJ, Gupta KK (1976) Macroaneurysms of the retinal arteries. Arch Ophthalmol 94: 1092-1096.
-
Campbell FP (1976) Coats’ disease and congenital vascular retinopathy. Trans Am Ophthalmol Soc 74: 366- 424.
-
Robertson DM (1973) Macroaneurysms of the retinal arteries. Ophthalmology (Rochester) 77: 55-67.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report