Visual Outcome of Adult Cataract Small Incision Cataract Surgery in Northern Benin
Introduction: Cataract remains a public health problem in Africa. Its treatment remain essentially surgical. Several management techniques are available and the most adapted to a context with poor resources like lack of material and financial resources is small incision cataract surgery (SICS). Method: This was an exhaustive recruitment of the study population meeting the inclusion and non-inclusion criteria. Carried out from January 1st to May 30th of 2022 at Hôpital Saint André de Tinré (HOSAT) located in the Northern part of Benin. It involved patients aged 40 and above who underwent cataract surgery during the period of this study. Visual acuity was assessed before and after the surgeries at day 1 and day 30. Results: We included 213 eyes. The average age was 65.2 ± 9.1 years with a mean age of 65.2 ± 9.1 years. Comorbidities were dominated by arterial hypertension in 57.5% of cases. Preoperatively, all patients had at least in one eye a visual acuity of less than 1/20. The main intraoperative complication was posterior capsular tear with vitreous loss, found in 6% of cases. The average power of the implant was 21.4 ±1.7 diopters. The standard implant was used in 64.7% of patients. After one month, the visual acuity without postoperative correction was good in 32.1%; borderline visual acuity was 41.4% and poor visual acuity was 26.5%. Conclusion: Cataract remains the main cause of blindness in developing countries, particularly in rural areas. It is important to sensitize patients for early screening in order to improve theirs qualities of life
Introduction
Cataract, the leading cause of curable blindness, constitutes one of the target diseases of the “Vision 2020, the Right to Sight” initiative which aims to eliminate the causes of avoidable blindness by the year 2020 (WHO/9 February 25, 2000). it promote a world in which nobody is needlessly visually impaired, where those with unavoidable vision loss can achieve their full potential, intensify and accelerate prevention of blindness activities so as to achieve the goal of eliminating avoidable blindness by 2020 and Focus on diseases which are the main causes of blindness and for which proven cost effective interventions are available. Benin is one of the West African countries that had adopted this objective [1].
Cataract is the total or partial opacification of a normally transparent intraocular lens. It is responsible for a reduction in visual acuity [2]. Cataract treatment is essentially surgical. It consists in the ablation of the opacified lens nucleus [3, 4]. Several techniques exist but manual sutureless alternative phaco (PKA) is increasingly practiced in our country. Cataract surgery aims to obtain better visual acuity with a low rate of post-operative astigmatism. Thus, we conducted this study to evaluate the visual results of phacoalternative cataract surgery in Northern Benin.
Methods
This was a prospective cross-sectional study with descriptive and analytical aims. It started from January 1st to May 30th 2022 that is six months. It was carried out at the Hôpital Saint André de Tinré (HOSAT) located in northern Benin. Patients aged 40 and who had cataract surgery were included in the study.
Patients with traumatic cataract, retinal or optic nerve disease were excluded. A survey questionnaire was developed and filled in from the medical files and from interviewed patients. Variables from socio-demographic characteristics, medical history taking, pre-operative, intra and post-operative, post-operative and visual acuity finding was used.
All patients underwent A and B scan examination before surgery. Retrobulbar anesthesia was done to all patient for akinesia during surgery.
Superior side frown incision of 6 to 7 mm done follow by scleral tunnel was created starting 2 mm posterior to the limbus. A side-port incision was created to facilitate further intraocular manipulation. A can opener capsulotomy and hydrodissection were performed. Viscoelastic was injected above and behind the nucleus, which was then prolapsed into the anterior chamber then the nucleus is extracted by viscoelastic expression. The remaining cortex was manually removed with the Simcoe irrigation-aspiration cannula.
After implanting a poly methyl methacrylate (PMMA) lens into the capsular bag, the unsutured scleral pocket incision was confirmed to be watertight. The anonymity of the surgeon was respected. Visual acuity was assessed pre- and postoperatively on the 1st day (D1) and the 30th (D30). We adopted the WHO’s operational definitions implemented for the follow up of cataract operations [5].
- Visual acuity categories according to the WHO
- Good visual acuity: visual acuity above or equal to 3/10 and lower to 5/10.
- Borderline visual acuity: visual acuity lower than 3/10, but above 1/10.
- Poor visual acuity: visual acuity lower than 1/10 but higher than 1/20.
- Blindness: visual acuity less than 1/20.
- The variables studied were represented variables studied were classified in socio-demographic characteristics; clinical aspects, intraoperative incidents and postoperative complications. The graphs are created in Excel and the presentations are made using Word software.
Results
The mean age was 65.2 ± 9.1 years. The extremes of age were 49 and 92. The 60 to 69 age group (47.9%) was the most represented.
Of the 213 patients, 111 (51.6%) were male and 104 (48.4%) female, giving a sex ratio (M/F) of 1.06. A total of 10 out of 213 respondents had an ocular history other than cataract. These were mainly pterygium (80.0%). More than a third of respondents had a medical history. The predominant medical history was hypertension (57.5%).
Clinical Aspects
Arterial hypertension represented the predominant medical history with 57.5%. Preoperatively, all patients had at least in one eye a visual acuity of less than 1/20 according to the World Health Organization. The cataract was total white in 48.9% of cases, corticonuclear in 12.1% of cases, nuclear in 17.3% of cases, and posterior subcapsular in 20.0% of cases. The average implant power was 21.4 ±1.7 diopters with extremes of 17 and 25 diopters. The standard implant was used in 64.7% of patients.
Peroperative Complication
Intraoperative complication occurred in 21 eyes, or 9.8%. This mainly involved capsular tear in 13 eyes or 6% (Table 1).
| Peroperative Complication | Number (N=21) | Percentage |
|---|---|---|
| Early entry | 2 | 0,95 |
| Iris prolapsus | 3 | 1.43 |
| Vitreous issue | 3 | 1.43 |
Table 1: Shows the distribution of the eyes of the respondents according to intraoperative incidents.
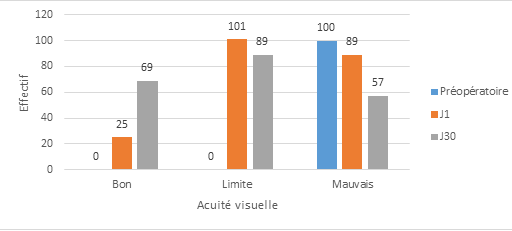
Postoperative Visual Acuity
On postoperative day 1, we noted 11.6% good visual acuity, 46.9% borderline visual acuity and 41.3% poor visual acuity.
On postoperative day 30, we noted 32.1% good visual acuity, 41.4% borderline visual acuity and 26.5% poor visual acuity. (Figure 1) shows the evolution of postoperative visual acuity.
Postoperative Complications
On day 1 postoperative follow up, corneal edema was central in 38.1% of eyes. The implant was dislocated in 9.8% of eyes. An anterior capsular remnant was observed in 5.1% of eyes.
On day 30 cornea was transparent in 85.6% of eyes.. The implant was centered in 93.5% of the eyes because of day 1 implant reposition done. A residual mass was observed in 0.3% of eyes. Table 2 presents the distribution of postoperative complications according to progression.
| Number of Patients | Percentage | Number of Patients | Percentage | |
|---|---|---|---|---|
| Day 1 | Day 30 | |||
| Cornea | ||||
| Keratitis | 2 | 0.9 | 1.4 | |
| Corneal Edema | 82 | 38.1 | 25 | 13.1 |
| Anterior Chamber | ||||
| Athalamia And Hypothalamia | 10 | 4.7 | 5 | 3.3 |
| Hyphema | 10 | 2.3 | 2 | 0.9 |
| Pupil | ||||
| Myosis | 4 | 1.9 | 1 | 0.5 |
| Mydriasis | 9 | 4.2 | 4 | 1.9 |
| Pupillary Deformation | 13 | 6 | 14 | 6.5 |
| Iris | ||||
| Iris Pigments On The Endothelium | 7 | 3.3 | 4 | 1.9 |
| Implant | ||||
| Dislocated | 5 | 2.3 | 2 | 0.9 |
| Iris Pigments On The Anterior Surface Of The Implant | 16 | 7.4 | 12 | 5.6 |
| Residual Mass | ||||
| Abundant | 1 | 0.5 | 2 | 0.9 |
| Moderate | 8 | 3.7 | 5 | 2.3 |
| Anterior Capsule | ||||
| Remaining Peripheral Capsule | 8 | 3.7 | 5 | 3.3 |
| Posterior Capsule | ||||
| Central And Peripheral Opacity | 11 | 5.2 | 4 | 1.9 |
| Broken | 13 | 6 | 13 | 5.6 |
Table 2: Distribution of post-operative complications according to progression.
Discussion
Sociodemographic Characteristics
In our series, the average age of patients was 65.2 ±9.1 years. This result is similar to those reported in the literature by Diallo et al. [6] in Burkina Faso as well as Dohvoma et al. [7] in Cameroon found an average age of 66±9.93 years and 66.87±15.10 years respectively. Cataract is evenly distributed according to gender. On the other hand, other studies have reported a female predominance [6, 7]. This could be accounted by the fact that decision to go to eye care come from the man.
This high proportion of cataract surgery on blind patients in our country could be explained by the fact that patients wait until they are blind before consulting a doctor, but also because they are people with limited financial means. Most studies [6, 7, 8] on cataract surgery in sub-Saharan Africa have reported a high blindness rate on admission.
The evaluation of the functional result without optical correction revealed good visual acuity of 11.6% to 32.1% from postoperative day1 to day30. These values are below the standards recommended by the WHO. Several factors influence visual acuity postoperatively. In our patients, biometrically compliant implants were not always available. Thus, standard implants were used in 46.4% of patients. These results are close to those reported by Diallo which is 40.33% placement of a standard implant. This could affect the functional results of surgery by inducing ametropia. Other factors such as intraoperative and postoperative complications, refraction of the eye before and after cataract surgery, particularly astigmatism, could also influence the functional results. We limited the assessment of visual acuity to one month without optical correction because our study was carried out in a rural area but also most of the patients were financially deprived and had little intellectual activity.
The main intraoperative complication was the posterior capsular tear found in 6% of cases. This result is higher than that of Alamou et al. [5] in southern Benin who found 4.1% posterior capsular tear. As other intraoperative incidents, there was also vitreous loss with a rate of 1.43%. This result is similar to those found respectively by Diallo et al and [6] and Guirou et al. [9] i.e. 1.33% and 1.83%.
Most authors [6, 7] agree on the fact that frequent complications during alternative SICS are vitreous loss and tear of the posterior capsule. They are mainly due to factors such as the quality of the technical approach and the experience of the surgeon, vitreous syneresis in the elderly.
Early Postoperative Complications
Corneal edema constituted the main early postoperative complication recorded at a rate of 38.2%. Several authors have made the same observation but with lower proportions. These were Diallo et al. [6] as well as Maneh et al. [11] who reported 26.33% and 35.75% respectively.
In several studies, corneal edema is the first and main postoperative complication regardless of the surgical technique used.
Its frequency varies from 10.9% to 30% [12]. It is most often due to manipulations in the anterior chamber and especially during manual expulsion of the crystalline lens nucleus.
Late Postoperative Complications
In our study, corneal oedema was the main late postoperative complication (11.2%). This could be explained by the fact that our patients were reviewed at day1 post-op which is related to temporary high pressure by viscoelastic retention in the anterior chamber and received treatment for lowering pressure before being reviewed at day30.
Opacification of the posterior capsule was the second late postoperative complication in our study. Alamou et al. [13], in a study carried out in Benin found no statistically significant difference between the occurrence of posterior capsular opacification and the technique used in performing SICS. Secondary cataract (posterior capsular opacification) would represent a real problem, hampering the functional results of cataract surgery. It is a complication that is most often unpredictable.
Conclusion
Cataract remains a public health problem in our regions where most patients seek care in a state of blindness. The results of surgery must be improved by strengthening the technical platform and the availability of implants as well as the establishment of a universal health insurance plan.
References
-
Abba-Kaka Y, Diori N, Roufaye I (2021) Comparative study of surgical techniques in cataract surgery in Niger. European Scientific Journal 17(17): 180.
-
Bella AL, Bensaid P (2020) Blind pathologies in Africa: the example of Cameroon. In Zanlonghi X. Visually impaired and blind. How to render service to our patients. SOP- SFO joint relationship. Paris: Elsevier Masson 35-40.
-
Sanou J, Meda N, Ahnoux-Zabsonre A, Rigal K (2014) Cataract surgery without sutures. Pan Afr Med J, pp: 20- 25.
-
Abenhaim A, Assouline M (2018) Cataracts. Etiologies, diagnoses, principles of treatment. Practitioner’s Journal 44: 1811-1816.
-
Alamou S, Sounouvou I, Tchabi S (2006) Extra capsular extraction of crystalline: experience of CNHU-HKM from Cotonou. Benin Medical 32: 16-22.
-
Diallo JW, Meda N, Ahnoux-Zabsonre A, Yameogo C, Dolo M, et al. (2015) Functional results of cataract surgery for phacoalternative with implantation in the postoperative room for 300 cases in Bobo Dioulasso. Pan Afr Med J 20(1): 1-10.
-
Dohvoma VA, Ndongo J, Ebana MSR, Mvilongo Tsimi C, Nguena MB (2018) Health Sci and Dis. Functional results of cataract surgery for the small manual incision technique 19(4): 27-30.
-
Djiguimde PW, Diomande IA, Ahnoux-Zabsonre A, Koffi KV, Meda TA, et al. (2015) Results of advanced cataract surgery for tunneling: based on 262 cases performed in the CHR of Banfora. Pan Afr Med J 14(22): 366-368.
-
Guirou N (2013) Functional Outcomes of Adult Cataract Surgery. J Fr Ophthalmol 36: 19-22.
-
Alwan A, Mohammed R (2017) Morganian Cataract. Practitioner’s Journal 28: 104-110.
-
Maneh N, Banla M, Nonoon KB, Balo KP (2015) Small manual incision cataract surgery: an alternative in Sub- Saharan Africa. Research 2: 1-29.
-
Meda N, Daboue A, Nagallo Y, Ouedraogo PA, Ramde B, et al. (2019) Interest of extracapsular cataract extraction with artificial lens implantation. Burkina Medical 13(2): 14-17.
-
Alamou S, Yehouessi L, Bra’eyatcha BN (2015) Epidemiological and clinical aspect of blinding diseases in the national teaching hospital CNHU- HKM) in Cotonou. J Ophthalmic Pathol 5: 50-69.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report