Claude Bernard Horner Syndrome-Case Presentation
Introduction: The syndrome Claude Bernard-Horner (SH) is characterized by eyelid ptosis, pupillary miosis and anhidrosis, it is due to an interruption of the oculosympathetic pathway. The etiologies are multiple, including tumor, traumatic, iatrogenic or vascular. Sometimes it represents a medical emergency. For its diagnosis, eye drop tests are used, such as cocaine, hydroxyamphetamine or apraclonidine, and neuroimaging tests to establish the etiology. We present a case of HS associated with Hodkin Lymphoma (HL). Objective: Describe the clinical characteristics and the imaging study in a case with SH. Presentation of the case. A 24-year-old patient, with a clinical and histopathological diagnosis of HL, the tumor occupies the anterior mediastinum with lymphadenopathy in both supra and infraclavicular side chains of the neck, predominantly right. He presented with ptosis, miosis, and apparent enophthalmos. The diagnosis was based on clinical examination and pupillometry, in addition to images obtained by computed tomography (CT). Conclusions: The usefulness of the neuro-ophthalmological and imaging clinical examination in the identification of HS in this patient was demonstrated
Introduction
Horner syndrome (HS) was initially described in animals by the French physiologist Claude Bernard in 1854 and was subsequently discovered in a soldier who suffered a gunshot wound to the neck. However, the Swiss ophthalmologist Johann Friedrich Horner is credited with much of this discovery for being the first to fully describe this syndrome in 1869 and attribute its cause to oculosympathetic paresis [1, 2]. It manifests itself with the following triad: ptosis, miosis and anhidrosis, which does not occur in all cases because it depends on the level where the lesion is located [3, 4]. SH can be congenital or as a result of obstetric and acquired trauma (secondary to another disease) and idiopathic [5, 6].
Due to the acute loss of oculosympathetic vasomotor control, other clinical signs may occur, such as conjunctival injection, facial erythema, and congestive nasal mucosa. Enophthalmos is apparent and is due to the decrease in the palpebral fissure [7, 8]. Sometimes not all the signs of the classic triad are present, or other associated signs appear, such as mild elevation of the lower eyelid, vocal cord paralysis, heterochromia of the iris, or pain in the face or neck, which can help guide the picture [1, 2, 3]. Sympathetic innervation is believed to be necessary for melanin formation by stromal melanocytes, so disruption of innervation can lead to iris hypochromia on the affected side. This is a typical feature of congenital Horner syndrome [3].
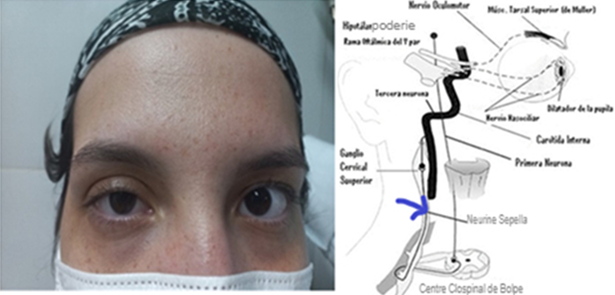
The oculosympathetic pathway is a circuit that includes three neurons. The first goes from the diencephalon to the spinal cord, the second or preganglionic ends in the cervical ganglion, and the third divides into two branches that innervate the eye and the ipsilateral face. Its axons ascend through the adventitia of the internal carotid, penetrate through the cavernous sinus, and together with the nasociliary branch of the trigeminal nerve, innervate the Mullerian muscle of the eyelids, the lacrimal gland, the iris dilator muscle, and the sweat glands. Facial and the small blood vessels of the skin [1, 2, 3, 4, 5, 6, 7, 8].
Horner syndrome can be classified into three groups depending on the location of the lesion. Central, which can occur in lesions of the hypothalamus, brain stem and spinal cord that affect the sympathetic pathway. The most frequently seen entities are Wallenberg syndrome and syringomyelia, among others. The preganglionic type may result from root lesions in the spinal cord, brachial plexus, trauma, lung apex lesions, or mediastinal tumors. Postganglionic lesion is related to diseases of the internal carotid artery, base of the skull, diseases of the cavernous sinus, superior orbital fissure and diseases of the orbital apex, among others [4].
In the case of third-order neuron injury, the sympathetic fibers responsible for the sudomotor function of the lower portion of the face separate from the oculosympathetic pathway before the superior cervical ganglion, therefore, anhidrosis will rarely be observed in this distribution. in postganglionic lesions, so sweating in the upper third of the face should be explored [9, 10, 11]. We can easily look for this information by applying talcum powder to the patient’s face and asking him to perform physical activity to observe if any side of the face does not present sweating, or in a better known way by using iodine [11].
Pupillary symptoms are usually subtle, since anatomically the pupil in its nervous control (sympathetic and parasympathetic) has a 30:1 ratio of parasympathetic and sympathetic fibers. Therefore, anisocoria is not very evident in mesopic conditions [2, 3]. It is extremely important to know if the involvement is pre- or postganglionic and if it involves the fibers that follow the course of the external carotid and its branches, where the control of sweating and piloerection of the hemiface lies. The symptoms and signs due to this condition (anhidrosis and dry skin) occur initially and then disappear [4].
To diagnose and localize HS, cocaine or anesthetic eye drops (tetracaine) can be used. When instilled in the eye, it inhibits the reuptake of norepinephrine (neurotransmitter of the sympathetic system), previously released in the myoneural junction, therefore it induces mydriasis when a drop of this eye drop is instilled in patients with the oculosympathetic pathway intact. which produces dilation in the normal eye but not in the affected eye? Apraclonidine (commercially available alpha-2 agonist -Iopimax- as an ocular hypotensive agent). It has recently been discovered that apraclonidine 0.5%, an antiglaucomatous drug that is very easy to obtain in any ophthalmology clinic, has high sensitivity and specificity to confirm this syndrome, making it an excellent option in case of clinical suspicion [4, 5]. Apraclonidine is a weak α-1 and strong α-2 agonist; In the presence of HS, there is hypersensitivity due to denervation of the α-1 receptors of the palpebral Müller muscle and the iris, so the instillation of this drug in both eyes causes a resolution of the ptosis and a relative mydriasis on the affected side [4].
The technique of choice to establish the etiology is angio-tomography, which allows detecting vascular alterations such as dissections or carotid thrombosis, which can endanger the patient’s life. Other tests such as Computed Tomography (CT), Magnetic Resonance (MRI) with or without contrast, arteriography, chest x-ray or Doppler ultrasound, can be used in a personalized way in each case [1, 5]. Hydroxyamphetamine (enhances the release of norepinephrine in the postganglionic endings) delimits the location of the lesion, since if it is preganglionic it produces dilation in both eyes, but if the lesion is postganglionic, there is no pupillary reaction (dilation) in the affected eye8. With the aim of describing the manifestations that occur in these cases and carrying out a bibliographic review, a patient with HS in the evolutionary course of Hodgkin Lymphoma is presented. Lymphoma was described for the first time in 1856 by the English doctor Thomas Hodgkin. Years later, Samuel Wilks published a series of 45 cases that included the five described by Hodgkin and proposed the term Hodgkin’s disease in his honor8. Lymphomas are solid tumors of lymphoid cells, they constitute a heterogeneous group of malignant diseases characterized by neoplastic proliferation of the lymphoreticular portion of the reticuloendothelial system, which mainly affects the cells of the lymphocytic series and histiocytes, which are subdivided into: lymphoma Hodgkin (HL) and non-Hodgkin lymphoma (NHL). NHL is more common and has several subtypes [7, 8].
Clinical Case
A 24 year old female patient In March 2021, the clinical and histopathological diagnosis of Hodkin Lymphoma (HL) was made. And nodular sclerosis stage II BX (bulky mediastinal mass approximately 10x15 cm). She has received polychemotherapy with the regimen: ASUD (adamycin, biemycin, vinbiastine, dacarbazine), partial remission was achieved, so she was switched to the second-line regimen called ICE. (carroplatin, vp-16, ifosfamide, mesna), for six cycles. Subsequently, the E-SHAP regimen (vp-16, cisplatin, cytosar, methylprednisolone) was continued for 2 cycles with good clinical response. Biological agents such as Rituximab were used due to the presence of giant lymphadenopathy of the entire right cervical chain.
The patient was in intensive care due to the severity of the condition. The family detects the drooping or palpebral ptosis of the right eye, but they do not attend the Neuro- ophthalmology consultation until a month after the disease is stabilized. During the interrogation, she referred to dryness of the skin on the right side of her face, but it is known that this sign disappears over time, due to autonomic self-regulation.
An ophthalmological examination was performed, with slit lamp (SLT) evaluation and pupillometry with an infrared camera: ptosis and miosis were evident. Figure 1 shows the eyelid ptosis of the right eye (OD), which was classified as mild, due to a drop of 2 millimeters (mm) with respect to the physiological eyelid level. The left eye (LE) was normal.
The results of pupillometry with an infrared camera are as follows: in scotopic conditions (light off): OD.4.0 mm, OI: 5.0 mm and in photopic conditions (light on): OD: 3.5 mm, OI: 4 mm. When the anesthetic eye drops were instilled, there were no changes in the RE and a dilation of one mm was observed in the LE. The reduction in the pupil diameter of the RE in the dark was evident, with respect to the LE, which shows the involvement of the dilator muscle, innervated by the sympathetic system, with conservation of the light reflex, mediated by the parasympathetic that stimulates the recruitment of the sphincter of the pupil. Enophthalmos
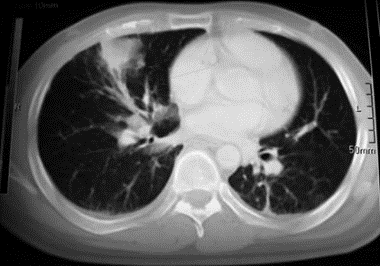
was apparent, according to the result of exophthalmometry, which showed no differences between both eyes. Vision and fundus were normal in this patient. SH was diagnosed during the course of HL. It was based on the clinical examination in LH and pupillometry in addition to the images obtained in CT angiography of the chest and neck, where giant cervical lymphadenopathy was evident throughout the lymph node chain. The patient and her family reported signs of dryness of the right side of the face, but this could not be verified by the doctor. The blue arrow points to the affected neuron in the oculosympathetic chain (Figure 2).
Discussion
According to the clinical examination and the diagnostic means used in this case, SH was proposed during the course of HL with involvement of the second neuron, due to the increase in volume of the cervical lymph nodes and the compression of the mediastinum by the tumor. The diagnosis of the patient seen in the Neuro-ophthalmology clinic was based first of all on the clinic, on pupillometry with an infrared camera, in addition to imaging studies such as CT angiography of the chest and neck.
Most authors [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12] agree that malignant tumors in the neck and chest region are the most common cause of HS. In most cases the second neuron (preganglionic pathway) is involved, the involvement of the third or postganglionic pathway is less frequent (10%) and in a lower percentage the first neuron or sympathoparesis is expressed in Wallenberg syndrome. SH is an exceptional form of presentation of HL, of which only eight cases have been described in adult patients. The findings associated with HS are a consequence of the loss of sympathetic innervation of the face and the ipsilateral eye according to the involvement of the oculosympathetic pathway [8].
In 2017, Abascal C, et al. [8] presented the case of a 19-year-old man who attended the Ophthalmology department due to conjunctival irritation and treatment with anti-allergy eye drops for two months. Ptosis and miosis were detected, without anhidrosis, which is why it is proposed that it illustrates a rare presentation of HL that could be the first well-documented case of injury to the third neuron of the oculosympathetic pathway in the course of HL. In the study carried out, HL of the mediastinum and cervical lymph node chain was diagnosed. The aforementioned authors are based on the absence of anhidrosis, which only occurs in conditions below the stellate ganglion (second neuron), however, this case was evaluated with at least 2 months of evolution of the first symptoms, so This sign could disappear, which is temporary due to the hypersensitivity of the receptors of the denervated blood vessels to circulating adrenergic substances with resulting vasoconstriction and disappearance of anhidrosis.
Conjunctival hyperemia may also disappear; it occurs due to the acute loss of oculosympathetic vasomotor control on the affected side and recovers in a manner similar to anhidrosis. It may appear accompanied by epiphora and nasal discharge and may initially be confused with allergic conjunctivitis, as described in the case history of Abascal C, et al [8].
Tumors are one of the Most Common Causes of SH.
In 2016, Camos-Carreras A, et al. [3] published the case of a 63-year-old woman referred to the ophthalmology service.
On examination, a 2 mm ptosis of the right upper eyelid was observed; pupillary miosis was also evident on that side, which is why it is concluded as SH. In the examinations performed, a multinodular goiter with cervical lymph node chain compression was detected. Martínez-Mayorquín V, et al. [9] presents the case of a 38-year-old woman who presented with ptosis of the upper eyelid of the right eye of 2 months’ duration. Major Anisocoria in the dark and right miosis were observed, so it was concluded like a SH. When following the lymph node chain involved, involvement of the axillary lymph nodes was detected, which are suggestive of a malignancy of breast origin? A chest examination was performed and a lesion highly suggestive of breast cancer was found.
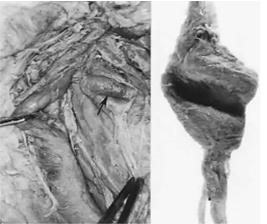
In elderly patients with cardiovascular risk factors, smoking and high blood pressure, the atheromatous and tortuous internal carotid artery can make a groove or indentation in the stellate ganglion, which manifests itself with the characteristics of HS due to involvement of the second neuron, without any tumor being detected on examination, therefore, it is classified as idiopathic SH [2]. Figure 3 shows the aforementioned through a cadaveric dissection, where the affected carotid is separated. The node is shown in a magnified anteroposterior view to demonstrate indentation.
SH is a rare neurological disorder associated with serious systemic diseases, so diagnosis and treatment must be immediate. In 2023, Walburg Z, et al. [10] published the case of a 63-year-old woman with right retroocular pain, photophobia, dizziness, and signs of neurological focalization, ptosis and miosis on the same side. Radiological studies diagnosed a dissection of the internal carotid artery. In a patient with SH and ocular pain, suspect this serious, potentially fatal vascular condition.
The clinical diagnosis of HS is difficult, because in the majority of patients it is asymptomatic and the classic triad does not manifest: ptosis, miosis and anhidrosis. The onset of anisocoria is not well defined, which is discovered accidentally because dark or brown iris color predominates in our environment. The eye drops used for diagnosis and localization of the affected neuron in the oculosympathetic chain, such as apraclonidine and hydroxyamphetamine, are not available in clinics and emergency centers, and false positives and negative results are reported if they are not used in diluted solutions (0.5 or 1%) and with the established time interval between these diagnostic eye drops and the kitchen [11].
Currently, an algorithm for diagnosis and treatment has been established. It is based on the neuro-ophthalmological clinical examination; subsequently, it is proposed to perform a single neuroimaging study of the entire oculosympathetic pathway with cranial MRI extending to the T2 level, with a concomitant MRI of the neck. If the presentation is acute or if MRI is contraindicated, CT and angiotomography of the brain and neck are performed [7, 8, 9, 10, 11, 12].
Conclusions
The patient suffers from Horner syndrome of the second neuron, in the course of mediastinal Hodkin Lymphoma and the cervical lymph node chain. The usefulness of the neuro- ophthalmological clinical examination was demonstrated in the identification of Horner syndrome, which may be the first manifestation of mediastinal Hodkin Lymphoma. Determining the etiology of SH is of utmost importance to preserve the patient’s quality of life and in some cases avoid death.
References
-
Dafereras M, Sapouridis H, Laios K, Chrysikos D, Mavrommatis E, et al. (2020) The pioneer ophthalmologist Johann Friedrich Horner (1831-1886) and the clinical anatomy of the homonymous syndrome. Acta Chir Belg 120(5): 363-365.
-
Slamovits T, Glaser J, Mbekeani J (2006) The Pupils and Accommodation. Chapter 15: In: Duane, et al. (Eds.), Clinical Ophthalmology 2nd (Edn.), CD ROM, Lippincott William Wilkins.
-
Camos-Carreras A, Fontana S, Ortiz-Perez S (2018) What would you do when faced with a patient with Horner syndrome? Family Medicine. Semergen 44(2): 131-134.
-
Patel S, Ilsen P (2003) Acquired Horner’s syndrome: clinical review. Optometry 74: 245-256.
-
Silverman A, Beres S (2022) Child Neurology: Horner Syndrome in an Otherwise Well-Appearing Infant. Neurology 99(23): 1053-1056.
-
Vera ORB, Fernandez L, Arias AP, Ballarinoa D, Jaraa A (2018) Congenital Horner syndrome. Clinical case. Arch Argent Pediatr 116(1): e85-e87.
-
Keita IK, Nazario-Dolz AM, Falcon-Vilarino GC, Castillo- Toledo L, Rodriguez-Fernandez Z, et al. (2020) Considerations regarding mediastinal tumors. Rev Colomb Cir 35: 472-482.
-
Abascal C, Abarzuza R, Cortaire P, Ramos P (2017) Horner syndrome: unusual ophthalmological presentation of Hodking lymphoma. An Syst Sanit Navar 40(3): 461-466.
-
Martinez-Mayorquin V, Lozano-Elizondo D, Moreno- Anda R, Pesci-Eguia L, Miranda-Sanchez K, et al. (2019) Horner syndrome as a reason for consultation in a patient with a breast tumor Case report. Rev Mex Oftalmol 93(5): 258-261.
-
Walburg Z (2023) Acute Painful Horner Syndrome as the First Presenting Sign of Carotid Artery Dissection. Fed Pract 40(5): 160-166.
-
Davagnanam I, Fraser C, Miszkiel K, Daniel C, Plant G (2013) Adult Horner’s syndrome: a combined clinical, pharmacological, and imaging algorithm. Eye 27(3): 291-298.
-
Maamouri R, Ferchichi M, Houmane Y, Gharbi Z, Cheour M (2023) Neuro-Ophthalmological Manifestations of Horner’s Syndrome: Current Perspectives. Eye Brain 15: 91-100.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report